You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5806)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
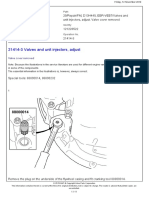
- 21414-3 Valves and Unit Injectors, AdjustDocument11 pages21414-3 Valves and Unit Injectors, AdjustTeguh Imam Adri100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Quadratic EquationsDocument29 pagesQuadratic EquationsKristine Joyce ArinaboNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Barclay SilencersDocument12 pagesBarclay SilencerspostboxsgNo ratings yet
- Eco7 Case AnalysisDocument18 pagesEco7 Case AnalysisShashin Singh67% (3)
- RTN 950 Configuration GuideDocument1,722 pagesRTN 950 Configuration GuideWilliam Fernandes100% (2)
- Harlem Renaissance Tone and Diction EssayDocument2 pagesHarlem Renaissance Tone and Diction EssayTheTwelfthDocNo ratings yet
- Quarter Two Live Play ReviewDocument2 pagesQuarter Two Live Play ReviewTheTwelfthDocNo ratings yet
- Booker T. Washington and W.E.B. DuBois EssayDocument3 pagesBooker T. Washington and W.E.B. DuBois EssayTheTwelfthDocNo ratings yet
- Booker T. Washington and W.E.B. DuBois EssayDocument3 pagesBooker T. Washington and W.E.B. DuBois EssayTheTwelfthDocNo ratings yet
- Report On Cordect TechnologyDocument22 pagesReport On Cordect TechnologyAnkush JamthikarNo ratings yet
- Exercise 1 Linked List: Datastructures and Algorithm Using C++ - Practical Exercise 1Document7 pagesExercise 1 Linked List: Datastructures and Algorithm Using C++ - Practical Exercise 1aryanboxer786No ratings yet
- While LoopDocument2 pagesWhile LoopNisha PoudelNo ratings yet
- Types of Residential PropertyDocument32 pagesTypes of Residential PropertyAlex CruzNo ratings yet
- EDUSE161121-Practical Accounting in The GST REgime For Acctg Staff-AnisDocument4 pagesEDUSE161121-Practical Accounting in The GST REgime For Acctg Staff-AnisMahwiah JupriNo ratings yet
- AniscalMA - Learning Activity 4.1 4.3Document7 pagesAniscalMA - Learning Activity 4.1 4.3HeliNo ratings yet
- Local Government Marketing ModelDocument160 pagesLocal Government Marketing ModeladiNo ratings yet
- OPT A2 T2M Unit 12 WorksheetDocument1 pageOPT A2 T2M Unit 12 Worksheetmaria jose lopezNo ratings yet
- 1 s2.0 S0308521X23000616 MainDocument18 pages1 s2.0 S0308521X23000616 MainInpecta BalramNo ratings yet
- Manual: CODE No: 8608Document40 pagesManual: CODE No: 8608Aamir FurqanNo ratings yet
- Promoters Influence On Corporate Governance: A Case Study of Tata GroupDocument9 pagesPromoters Influence On Corporate Governance: A Case Study of Tata GroupAaronNo ratings yet
- Survey: Group Iii M.Voc TMCDocument8 pagesSurvey: Group Iii M.Voc TMCRohith MohanNo ratings yet
- Electronics Projects Traffic Light Lamp Blow Monitoring - SingaporeDocument5 pagesElectronics Projects Traffic Light Lamp Blow Monitoring - SingaporeAllan Abobon BulataoNo ratings yet
- Case 5 - Proton Full AssignmentDocument42 pagesCase 5 - Proton Full AssignmentShaa Didi100% (1)
- MVDKerala - RT Office PH No.sDocument2 pagesMVDKerala - RT Office PH No.sVidyaVasudevanNo ratings yet
- Bill Presentment Architecture in Oracle ReceivablesDocument42 pagesBill Presentment Architecture in Oracle Receivablessrees_15No ratings yet
- Full-Wave Controlled Rectifier RL Load (Continuous Mode)Document6 pagesFull-Wave Controlled Rectifier RL Load (Continuous Mode)hamza abdo mohamoud100% (1)
- Cobre Panamá - Feasibility (2010)Document188 pagesCobre Panamá - Feasibility (2010)Nicolas CarrascoNo ratings yet
- Honeywell 5800CO-Installation-InstructionsDocument4 pagesHoneywell 5800CO-Installation-InstructionsIzah FriendsNo ratings yet
- Catalog Tranzistori NPN de PutereDocument4 pagesCatalog Tranzistori NPN de PutereSmigun CorneliuNo ratings yet
- UFMC 2.8 User Manual PDFDocument173 pagesUFMC 2.8 User Manual PDFDario CastiglianoNo ratings yet
- Liquid Drainer PN16 / PN40: Forged SteelDocument14 pagesLiquid Drainer PN16 / PN40: Forged SteelErdincNo ratings yet
- Blue BrainDocument12 pagesBlue BrainPulak MandalNo ratings yet
- EDPS - (Guidelines) On Processing PI in Whistleblowing Procedure A 17-12-19Document16 pagesEDPS - (Guidelines) On Processing PI in Whistleblowing Procedure A 17-12-19Mario Gomez100% (1)
- Check of Speed SensorDocument7 pagesCheck of Speed SensorSteven ManuputtyNo ratings yet