You might also like
- Biophysical Characterization of Dry Facial Skin: J. L. Leveque, G. Grove, J. de Rigal, P. CorcuffDocument8 pagesBiophysical Characterization of Dry Facial Skin: J. L. Leveque, G. Grove, J. de Rigal, P. CorcuffLanna HarumiyaNo ratings yet
- 10 0000@Www Jstage JST Go jp@Article@Jat@23@11@2335436@ArticleDocument9 pages10 0000@Www Jstage JST Go jp@Article@Jat@23@11@2335436@ArticleLanna HarumiyaNo ratings yet
- Gloomy LifeDocument6 pagesGloomy LifeLanna HarumiyaNo ratings yet
- Click To Edit Master Subtitle StyleDocument4 pagesClick To Edit Master Subtitle StyleLanna HarumiyaNo ratings yet
- Click To Edit Master Subtitle StyleDocument4 pagesClick To Edit Master Subtitle StyleLanna HarumiyaNo ratings yet
- Presentation TitleDocument4 pagesPresentation TitleLanna HarumiyaNo ratings yet
- Click To Edit Master Title StyleDocument4 pagesClick To Edit Master Title StyleLanna HarumiyaNo ratings yet
- Frans Sarumpaet, Dr. Pembimbing: Bayu Rusfandi, DR., SPPDDocument13 pagesFrans Sarumpaet, Dr. Pembimbing: Bayu Rusfandi, DR., SPPDLanna HarumiyaNo ratings yet
- Title: SubheadingDocument7 pagesTitle: SubheadingLanna HarumiyaNo ratings yet
- Tentative Acara Workshop SimpoDocument7 pagesTentative Acara Workshop SimpoLanna HarumiyaNo ratings yet
- Kol Ditz 2016Document3 pagesKol Ditz 2016Lanna HarumiyaNo ratings yet
- Related InfectionDocument3 pagesRelated InfectionLanna HarumiyaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Chapter 11: Re-Situating ConstructionismDocument2 pagesChapter 11: Re-Situating ConstructionismEmilio GuerreroNo ratings yet
- GHMC Results, 2009Document149 pagesGHMC Results, 2009UrsTruly kotiNo ratings yet
- 7wonders ZeusDocument18 pages7wonders ZeusIliana ParraNo ratings yet
- 4-Cortina-Conill - 2016-Ethics of VulnerabilityDocument21 pages4-Cortina-Conill - 2016-Ethics of VulnerabilityJuan ApcarianNo ratings yet
- Archbishop Averky Taushev - Stand Fast in The TruthDocument14 pagesArchbishop Averky Taushev - Stand Fast in The Truthdorin_jambaNo ratings yet
- Communication and Design Portafolio - Vanessa CerviniDocument34 pagesCommunication and Design Portafolio - Vanessa CerviniVanCerRNo ratings yet
- Adobe Scan 03-May-2021Document22 pagesAdobe Scan 03-May-2021Mohit RanaNo ratings yet
- "If It Ain't Cheap, It Ain't Punk": Walter Benjamin's Progressive Cultural Production and DIY Punk Record LabelsDocument21 pages"If It Ain't Cheap, It Ain't Punk": Walter Benjamin's Progressive Cultural Production and DIY Punk Record LabelsIsadora Mandarino OteroNo ratings yet
- Architecture AsiaDocument84 pagesArchitecture AsiaBala SutharshanNo ratings yet
- Comprehensive Problem Excel SpreadsheetDocument23 pagesComprehensive Problem Excel Spreadsheetapi-237864722100% (3)
- Consolidated Terminals Inc V Artex G R No L 25748 PDFDocument1 pageConsolidated Terminals Inc V Artex G R No L 25748 PDFCandelaria QuezonNo ratings yet
- 01-Cost Engineering BasicsDocument41 pages01-Cost Engineering BasicsAmparo Grados100% (3)
- Sailpoint Training Understanding ReportDocument2 pagesSailpoint Training Understanding ReportKunalGuptaNo ratings yet
- BCLTE Points To ReviewDocument4 pagesBCLTE Points To Review•Kat Kat's Lifeu•No ratings yet
- Final Draft RTS On SADocument84 pagesFinal Draft RTS On SAjose pazNo ratings yet
- Financial Amendment Form: 1 General InformationDocument3 pagesFinancial Amendment Form: 1 General InformationRandolph QuilingNo ratings yet
- International PositioningDocument37 pagesInternational PositioningMansi A Kathuria100% (1)
- Loan AgreementDocument6 pagesLoan AgreementSachin ShastriNo ratings yet
- CHAPTER - 3 - Creating Responsive Supply ChainDocument23 pagesCHAPTER - 3 - Creating Responsive Supply Chainsyazwani aliahNo ratings yet
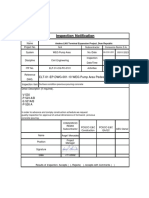
- In-CIV-201 INSPECTION NOTIFICATION Pre-Pouring Concrete WEG Pump Area PedestalsDocument5 pagesIn-CIV-201 INSPECTION NOTIFICATION Pre-Pouring Concrete WEG Pump Area PedestalsPedro PaulinoNo ratings yet
- Tail Lamp Left PDFDocument1 pageTail Lamp Left PDFFrancis RodrigueNo ratings yet
- 6 Chase Nat'l Bank of New York V BattatDocument2 pages6 Chase Nat'l Bank of New York V BattatrNo ratings yet
- Revision of Future TensesDocument11 pagesRevision of Future TensesStefan StefanovicNo ratings yet
- Uniform Civil Code and Gender JusticeDocument13 pagesUniform Civil Code and Gender JusticeS.P. SINGHNo ratings yet
- FRA - Project - NHPC - Group2 - R05Document29 pagesFRA - Project - NHPC - Group2 - R05DHANEESH KNo ratings yet
- The History of Land Use and Development in BahrainDocument345 pagesThe History of Land Use and Development in BahrainSogkarimiNo ratings yet
- Lecture 3 Islamic StudiesDocument10 pagesLecture 3 Islamic StudiesDr-Hassan JunaidNo ratings yet
- Tally Trading and Profit Loss Acc Balance SheetDocument14 pagesTally Trading and Profit Loss Acc Balance Sheetsuresh kumar10No ratings yet
- Vayigash BookletDocument35 pagesVayigash BookletSalvador Orihuela ReyesNo ratings yet
- Final WorksheetDocument13 pagesFinal WorksheetAgung Prasetyo WibowoNo ratings yet