You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Mass General Cover LetterDocument1 pageMass General Cover Letterapi-404285262No ratings yet
- Duties of Medical Officer of Health (MOHDocument11 pagesDuties of Medical Officer of Health (MOHanojan100% (1)
- Activity 1Document4 pagesActivity 1KyleRepolidon MoralesNo ratings yet
- 60 Revision MCQs For ProsDocument9 pages60 Revision MCQs For ProsUsman Ali AkbarNo ratings yet
- Hypertension Pamphlet.Document5 pagesHypertension Pamphlet.Adelerin David OluwatosinNo ratings yet
- Health and Physical Education Mod 1-2Document20 pagesHealth and Physical Education Mod 1-2Ethel Jane RemoNo ratings yet
- Unity 3Document3 pagesUnity 3Gabigames CarottiNo ratings yet
- Health Insurance Presentation. (Fn-26)Document19 pagesHealth Insurance Presentation. (Fn-26)m_dattaiasNo ratings yet
- Facts About Eating Disorders: What The Research ShowsDocument3 pagesFacts About Eating Disorders: What The Research ShowsLauro Espiritu Jr.No ratings yet
- Aromatherapy Patient Intake Form-BlankDocument8 pagesAromatherapy Patient Intake Form-Blankapi-282993701100% (2)
- Artigon Gold CapsuleDocument3 pagesArtigon Gold Capsulehk_scribdNo ratings yet
- The Sense of Stopping Migraine ProphylaxisDocument20 pagesThe Sense of Stopping Migraine ProphylaxisdedeadamNo ratings yet
- A Manual of Practical Exercises in PharmacologyDocument79 pagesA Manual of Practical Exercises in Pharmacologyrajender67% (3)
- British Association of Dermatologists and British Photodermatology Group Guidelines For Narrowband Ultraviolet B Phototherapy 2022Document14 pagesBritish Association of Dermatologists and British Photodermatology Group Guidelines For Narrowband Ultraviolet B Phototherapy 2022Pietro PensoNo ratings yet
- Teacher In-Charge Dr. A. PRAKASH, M.Pharm (Pharmacology), PHD (Nitc)Document34 pagesTeacher In-Charge Dr. A. PRAKASH, M.Pharm (Pharmacology), PHD (Nitc)Prakash AppaNo ratings yet
- Editorial: The Annual Physical Examination: Needless Ritual or Necessary Routine?Document3 pagesEditorial: The Annual Physical Examination: Needless Ritual or Necessary Routine?ddyendNo ratings yet
- Drug Resistant TuberculosisDocument42 pagesDrug Resistant Tuberculosiszee1305No ratings yet
- Simulating Irregular Enamel Surface Texture in Composite Resin RestorationsDocument3 pagesSimulating Irregular Enamel Surface Texture in Composite Resin RestorationsIlseNo ratings yet
- Pediatric Infectious Diseases. Vaccination ProgramsDocument44 pagesPediatric Infectious Diseases. Vaccination ProgramsShubhra PaulNo ratings yet
- Vas BerryDocument1 pageVas BerryNabaa AlhammadiNo ratings yet
- Psoriatic ArthritisDocument6 pagesPsoriatic ArthritisAndu1991No ratings yet
- Program Terminal Report Sy 2022 (St. John Es February)Document4 pagesProgram Terminal Report Sy 2022 (St. John Es February)Amorelle Sharon AlemanNo ratings yet
- John Hopkins Specimen Collection Guidelines Updated 06-2019Document28 pagesJohn Hopkins Specimen Collection Guidelines Updated 06-2019Vincent ReyesNo ratings yet
- Sherese M Brooks News Release E-Portfolio 5Document3 pagesSherese M Brooks News Release E-Portfolio 5api-300678072No ratings yet
- Jktlfkku Yksd Lsok VK KSX) VtesjDocument2 pagesJktlfkku Yksd Lsok VK KSX) VtesjJeshiNo ratings yet
- Renewalcnaar : Arkansas Nursing Assistant Registry Renewal FormDocument3 pagesRenewalcnaar : Arkansas Nursing Assistant Registry Renewal FormKarrietta FrazierNo ratings yet
- KieyunabradleyweeblyDocument1 pageKieyunabradleyweeblyapi-383992037No ratings yet
- Community Mental HealthDocument40 pagesCommunity Mental Healthsameena vNo ratings yet
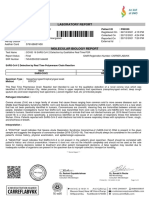
- Laboratory Report: Name: MR .Sandeep Mane Patient ID: P80359Document1 pageLaboratory Report: Name: MR .Sandeep Mane Patient ID: P80359akash srivastavaNo ratings yet
- Meiko 1Document6 pagesMeiko 1Meiko Ito-VillanuevaNo ratings yet