You might also like
- Human Brain & Cognition Assignmnet - KsdocxDocument14 pagesHuman Brain & Cognition Assignmnet - KsdocxYashpalNo ratings yet
- NEURO - Topic 1 - Additional SlidesDocument25 pagesNEURO - Topic 1 - Additional SlidesreaobokasegoeNo ratings yet
- History of BnsDocument24 pagesHistory of BnsHoorya HashmiNo ratings yet
- Summary of Chapter 1Document6 pagesSummary of Chapter 1Dicka ChenNo ratings yet
- Chapter 1 - History of NeuropsychologyDocument29 pagesChapter 1 - History of Neuropsychologymacue96No ratings yet
- 1.+fak Psikologi UMS Cognitive Kuliah+Tamu Biopsi1Document74 pages1.+fak Psikologi UMS Cognitive Kuliah+Tamu Biopsi1siti halida lubisNo ratings yet
- INTRODUCTIONDocument8 pagesINTRODUCTIONLaia CahorsNo ratings yet
- Biological Psychology: A Brief HistoryDocument29 pagesBiological Psychology: A Brief Historymarty_martinNo ratings yet
- Localization FunctionDocument5 pagesLocalization Functionapi-188978784100% (1)
- Brain LateralizationDocument46 pagesBrain LateralizationGabriel FrancisconiNo ratings yet
- Cognitive NeuroscienceDocument7 pagesCognitive NeuroscienceoptiuneNo ratings yet
- The Scientific MovementDocument5 pagesThe Scientific MovementMosesNo ratings yet
- Cognitive Neuroscience History PresentationDocument7 pagesCognitive Neuroscience History Presentationapi-365729288No ratings yet
- Procrsmed01407 0007Document22 pagesProcrsmed01407 0007ApostolisKambasNo ratings yet
- NeuroscienceDocument10 pagesNeurosciencea45624310% (1)
- Neuroscience: For The Journal, See - "Brain Science" Redirects Here. For Other Aspects of Brain Science, See, ,, andDocument7 pagesNeuroscience: For The Journal, See - "Brain Science" Redirects Here. For Other Aspects of Brain Science, See, ,, andDexterNo ratings yet
- Sperry RogerDocument6 pagesSperry RogerDavid Alcantara MirandaNo ratings yet
- Brain TheoryDocument41 pagesBrain TheoryNikhil NigamNo ratings yet
- Chapter 1 explores the history of cognitive neuroscienceDocument18 pagesChapter 1 explores the history of cognitive neurosciencedr_dicere_929212728No ratings yet
- Forty-Five Years of Split-Brain Research and Still Going StrongDocument7 pagesForty-Five Years of Split-Brain Research and Still Going StrongJuan Ignacio GelosNo ratings yet
- Prefrontal Lobotomy: January 2015Document7 pagesPrefrontal Lobotomy: January 2015duaNo ratings yet
- 12 The Advent of Modern NeuroscienceDocument3 pages12 The Advent of Modern Neurosciencezym1003No ratings yet
- OPTIONAL Gazzaniga 2005 PDFDocument7 pagesOPTIONAL Gazzaniga 2005 PDFSrikar VaradarajNo ratings yet
- The Functional Unity of The Cerebral Cortex and Sensory-Motor FunctionsDocument3 pagesThe Functional Unity of The Cerebral Cortex and Sensory-Motor FunctionsValentinus AlfrendoNo ratings yet
- The Split Brain in ManDocument6 pagesThe Split Brain in ManAKISNo ratings yet
- History of NeuroscienceDocument3 pagesHistory of Neurosciencemihaela irofteNo ratings yet
- Cognitive Neuroscience: The Brain Story' by Vaia LestouDocument53 pagesCognitive Neuroscience: The Brain Story' by Vaia LestouEdgardo100% (5)
- Introduction to Cognitive NeuroscienceDocument16 pagesIntroduction to Cognitive NeurosciencekhadijaNo ratings yet
- Two Hemispheres of The BrainDocument11 pagesTwo Hemispheres of The BrainAlexis RamirezNo ratings yet
- The Cerebral Sulci and Gyri: G C R, M.DDocument24 pagesThe Cerebral Sulci and Gyri: G C R, M.DJose Luis EspinosaNo ratings yet
- Brain Behavior 1Document8 pagesBrain Behavior 1sonika parikhNo ratings yet
- Neuropsychology Assignment 1Document9 pagesNeuropsychology Assignment 1Pranavi KhandekarNo ratings yet
- 2000-Aphasia and Wernickes ArcDocument1 page2000-Aphasia and Wernickes ArcMiguelNo ratings yet
- Splitbrain PDFDocument6 pagesSplitbrain PDFBrendz MarcialNo ratings yet
- Aphasia NoteDocument2 pagesAphasia NoteValentinus AlfrendoNo ratings yet
- Cognitive Neuroscience - WikipediaDocument10 pagesCognitive Neuroscience - WikipediaAlexandra Maria NeaguNo ratings yet
- Neuroscience of the nervous systemDocument8 pagesNeuroscience of the nervous systembezu76No ratings yet
- 1 - The Biological Approach To PsychologyDocument10 pages1 - The Biological Approach To PsychologyElmer SalazarNo ratings yet
- Sulci and GyriDocument24 pagesSulci and GyriravigoaNo ratings yet
- Historical Note: Marie Jean Pierre Flourens (1794-1867) : An Extraordinary Scientist of His TimeDocument1 pageHistorical Note: Marie Jean Pierre Flourens (1794-1867) : An Extraordinary Scientist of His TimeElelmoduNo ratings yet
- Script-Overview of Physiological PsychologyDocument5 pagesScript-Overview of Physiological Psychologysheen estemeraNo ratings yet
- The Neurologyof Sleep 2012 Published FormDocument18 pagesThe Neurologyof Sleep 2012 Published FormNeurologie PediatricaNo ratings yet
- Tart 1967BDocument5 pagesTart 1967BIno MoxoNo ratings yet
- NST1 - 2010 CreierulDocument10 pagesNST1 - 2010 Creierulcohal_adriana3397No ratings yet
- The Handbook of Clinical NeuropsychologyDocument1,439 pagesThe Handbook of Clinical NeuropsychologyFabiana AriasNo ratings yet
- Tutorial 4.2Document4 pagesTutorial 4.2Rosa FinizioNo ratings yet
- Cortex 2012 Catani-2Document26 pagesCortex 2012 Catani-2edgarNo ratings yet
- 1 s2.0 S0010945267800303 MainDocument15 pages1 s2.0 S0010945267800303 MainasdNo ratings yet
- NeuroscienceDocument18 pagesNeuroscienceSukro WijoyoNo ratings yet
- 2010 Article 9133 PDFDocument2 pages2010 Article 9133 PDFubunturiderNo ratings yet
- The Creation of Neuroscience: The Society For Neuroscience and The Quest For Disciplinary Unity 1969-1995Document80 pagesThe Creation of Neuroscience: The Society For Neuroscience and The Quest For Disciplinary Unity 1969-1995Sofia GomezNo ratings yet
- Lewis Amobi Ezie Neuropsychology Assignment-Split BrainDocument16 pagesLewis Amobi Ezie Neuropsychology Assignment-Split BrainEzie Lewis AmobiNo ratings yet
- Evolución Histórica de El Síndrome Del Lóbulo FrontalDocument8 pagesEvolución Histórica de El Síndrome Del Lóbulo FrontalFrancisca Cid BelmarNo ratings yet
- Haba Rubio2012Document13 pagesHaba Rubio2012Julian PintosNo ratings yet
- Psychology IB Biology Approach To BehaviorDocument25 pagesPsychology IB Biology Approach To Behaviorana kiranaNo ratings yet
- Cognitive NeuroscienceDocument64 pagesCognitive NeurosciencePedro M. BorgesNo ratings yet
- Module 2 PlasticityDocument42 pagesModule 2 PlasticityGUNJAN BHATIANo ratings yet
- Chapter 01Document45 pagesChapter 01scootysteeleNo ratings yet
- HSE Management Plan Rev. 08Document61 pagesHSE Management Plan Rev. 08rajaNo ratings yet
- The Northern Ireland Sport and Physical Activity Survey 2010 (SAPAS)Document178 pagesThe Northern Ireland Sport and Physical Activity Survey 2010 (SAPAS)sportniNo ratings yet
- HRM Case StudyDocument21 pagesHRM Case StudyNabil Eyg Iakini100% (1)
- Causes of Baby Dumping: Family Breakups, Lack of Education, and PovertyDocument2 pagesCauses of Baby Dumping: Family Breakups, Lack of Education, and Povertysirthana697547No ratings yet
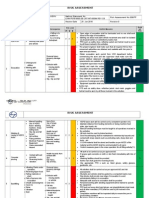
- Hse Risk Assessment - 006 Ra - Hdpe Duct LayingDocument7 pagesHse Risk Assessment - 006 Ra - Hdpe Duct Layingbinunalukandam83% (12)
- Introduction of Online Basic First Aid Course - For Circulation April 2021Document39 pagesIntroduction of Online Basic First Aid Course - For Circulation April 2021Yuwaraj NaiduNo ratings yet
- MSDSDocument3 pagesMSDSSiti Nurjanah SeptianiNo ratings yet
- TC Elastomeric Tapes SDS Rev 3, 2-19 - 1 PDFDocument6 pagesTC Elastomeric Tapes SDS Rev 3, 2-19 - 1 PDFEbondNo ratings yet
- Trays PDFDocument18 pagesTrays PDFBilal Hasan100% (1)
- Grand Unification For World Peace Music THerapy For Integrating Healthcare PDFDocument339 pagesGrand Unification For World Peace Music THerapy For Integrating Healthcare PDFDr Suvarna NalapatNo ratings yet
- Global Urology Devices MarketDocument14 pagesGlobal Urology Devices MarketNamrataNo ratings yet
- 2020 Corportate Sustainability ReportDocument22 pages2020 Corportate Sustainability ReportMohamed KannouNo ratings yet
- Preface: Color Profile: Disabled Composite Default ScreenDocument2 pagesPreface: Color Profile: Disabled Composite Default ScreenCláudio CastroNo ratings yet
- Top 5 Consumer Court CasesDocument7 pagesTop 5 Consumer Court CasesTanishka SoniNo ratings yet
- Maynilad Valenzuela Sewerage Project Environmental ReportDocument297 pagesMaynilad Valenzuela Sewerage Project Environmental ReportmarvilouNo ratings yet
- Quality Improvement: The Model For Improvement, PDSA Cycles, and Accelerating ImprovementDocument37 pagesQuality Improvement: The Model For Improvement, PDSA Cycles, and Accelerating ImprovementDewi ListyoriniNo ratings yet
- Evaluation and Treatment of Aphasia Among The Elderly With StrokeDocument11 pagesEvaluation and Treatment of Aphasia Among The Elderly With StrokemgpastorNo ratings yet
- Power of The Pinch Pinch Lower Lid BlepharoplastyDocument6 pagesPower of The Pinch Pinch Lower Lid BlepharoplastyBFF BotoxNo ratings yet
- Unilag MSC Environmenatl Toxicology SampleDocument4 pagesUnilag MSC Environmenatl Toxicology SamplebdianNo ratings yet
- Effectiveness of A Functional Rehabilitation Program For Upper Limb Apraxia in Poststroke Patients: A Randomized Controlled TrialDocument11 pagesEffectiveness of A Functional Rehabilitation Program For Upper Limb Apraxia in Poststroke Patients: A Randomized Controlled Trialguohong huNo ratings yet
- Organon of Medicine All Years 2marks Question Viva Questions AnswersDocument12 pagesOrganon of Medicine All Years 2marks Question Viva Questions Answersabcxyz15021999No ratings yet
- Nurs 5019 - Soap Note 41-60 Year OldDocument7 pagesNurs 5019 - Soap Note 41-60 Year Oldapi-308904543100% (1)
- Chapter 1 2 3Document77 pagesChapter 1 2 3Ferissa MohammadNo ratings yet
- West Fertilizer FINAL Report For Website 0223161 PDFDocument267 pagesWest Fertilizer FINAL Report For Website 0223161 PDFJawahar KhetanNo ratings yet
- DMLC Part I & II Cyprus (Hyundai Busan)Document17 pagesDMLC Part I & II Cyprus (Hyundai Busan)Shankar Singh0% (1)
- Hazards of Nitrogen AsphyxiationDocument10 pagesHazards of Nitrogen AsphyxiationRaja Senthil NathanNo ratings yet
- Nursing assessment diagnosis interventions rationale evaluationDocument3 pagesNursing assessment diagnosis interventions rationale evaluationanimesh pandaNo ratings yet
- Managing Painful Diabetic NeuropathyDocument26 pagesManaging Painful Diabetic NeuropathyAthalia TalawayNo ratings yet
- Lifting Vs Volumizing-The Difference in Facial Minimally Invasive Procedures When Respecting The Line of LigamentsDocument7 pagesLifting Vs Volumizing-The Difference in Facial Minimally Invasive Procedures When Respecting The Line of LigamentsArcelino Farias100% (1)
- Pathological Urine ConstituentsDocument22 pagesPathological Urine Constituentsmanni1001100% (3)