You might also like
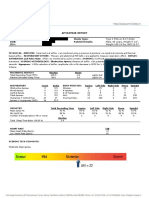
- Sample-Sleep Study Report PDFDocument2 pagesSample-Sleep Study Report PDFgopuNo ratings yet
- Sudhansu 2017 - Book - SleepDisordersMedicine PDFDocument1,258 pagesSudhansu 2017 - Book - SleepDisordersMedicine PDFVicko Suswidiantoro100% (1)
- Taylor Beck, "The Twitcing Eye: REM Sleep and The Emotional Brain"Document48 pagesTaylor Beck, "The Twitcing Eye: REM Sleep and The Emotional Brain"MIT Comparative Media Studies/WritingNo ratings yet
- Telepathy and The Technology of Mind ControlDocument18 pagesTelepathy and The Technology of Mind Controlbingwazzup100% (2)
- Interpreting Sleep Studies PrimerDocument23 pagesInterpreting Sleep Studies PrimerLaura MoiseNo ratings yet
- Clinician's Manual S8 AutoSet IIDocument70 pagesClinician's Manual S8 AutoSet IIsles22No ratings yet
- Sperry RogerDocument6 pagesSperry RogerDavid Alcantara MirandaNo ratings yet
- The Neurologyof Sleep 2012 Published FormDocument18 pagesThe Neurologyof Sleep 2012 Published FormNeurologie PediatricaNo ratings yet
- NeuroscienceDocument10 pagesNeurosciencea45624310% (1)
- The Scientific MovementDocument5 pagesThe Scientific MovementMosesNo ratings yet
- Neuroscience: For The Journal, See - "Brain Science" Redirects Here. For Other Aspects of Brain Science, See, ,, andDocument7 pagesNeuroscience: For The Journal, See - "Brain Science" Redirects Here. For Other Aspects of Brain Science, See, ,, andDexterNo ratings yet
- The Study of Human Sleep: A Historical Perspective: William C DementDocument6 pagesThe Study of Human Sleep: A Historical Perspective: William C DementKrisha ann MesanaNo ratings yet
- Normal Human Sleep, An OverviewDocument15 pagesNormal Human Sleep, An OverviewJulio César AcevedoNo ratings yet
- NeuroscienceDocument18 pagesNeuroscienceSukro WijoyoNo ratings yet
- Pol History gr10 2Document30 pagesPol History gr10 2api-321395685No ratings yet
- Human Brain & Cognition Assignmnet - KsdocxDocument14 pagesHuman Brain & Cognition Assignmnet - KsdocxYashpalNo ratings yet
- Neuroscience Is TheDocument8 pagesNeuroscience Is Thebezu76No ratings yet
- Reflex ArcDocument15 pagesReflex ArcFabio CampeottoNo ratings yet
- Lagerspetz, K. - JAKOB VON UEXKÜLL AND THE ORIGINS OF CYBERNETICSDocument9 pagesLagerspetz, K. - JAKOB VON UEXKÜLL AND THE ORIGINS OF CYBERNETICSBruno XavierNo ratings yet
- Neuroview: The 2014 Nobel Prize in Physiology or Medicine: A Spatial Model For Cognitive NeuroscienceDocument6 pagesNeuroview: The 2014 Nobel Prize in Physiology or Medicine: A Spatial Model For Cognitive NeuroscienceVictor CarrenoNo ratings yet
- Chapter 1 Textbook Notes - Introducing Biological PsychologyDocument7 pagesChapter 1 Textbook Notes - Introducing Biological PsychologyVanessa Eugine100% (1)
- Physiology PresentationDocument14 pagesPhysiology PresentationShivangi VermaNo ratings yet
- Artículo Generación y Propagación Del Potencial de AcciónDocument20 pagesArtículo Generación y Propagación Del Potencial de AcciónMISOL GALLEGUILLOS CALLEJASNo ratings yet
- Energetic MedicineDocument16 pagesEnergetic MedicineJAYAKUMAR85% (13)
- Sweden Human Brain Project Conference TranscriptDocument12 pagesSweden Human Brain Project Conference TranscriptHennot Do NorteNo ratings yet
- Tart 1967BDocument5 pagesTart 1967BIno MoxoNo ratings yet
- Zacharias Janssen: Van LeeuwenhoekDocument4 pagesZacharias Janssen: Van LeeuwenhoekCharl BaranganNo ratings yet
- Neuroscience: Jump To Navigation Jump To SearchDocument11 pagesNeuroscience: Jump To Navigation Jump To SearchDaniela BurceaNo ratings yet
- Lesson 123Document102 pagesLesson 123John Lerrie AdonayNo ratings yet
- Reporting Lesson 1 5Document29 pagesReporting Lesson 1 5Karen Angel AbaoNo ratings yet
- 2001 The First-Night Effect May Last More Than One NightDocument8 pages2001 The First-Night Effect May Last More Than One NightpsicosmosNo ratings yet
- 2003 E Fulcher Foundations of Cognitive PsychologyDocument26 pages2003 E Fulcher Foundations of Cognitive Psychologyrakum8No ratings yet
- Biology 1 - Cell-Basic Unit of LifeDocument22 pagesBiology 1 - Cell-Basic Unit of LifeAryan MendozaNo ratings yet
- Activity 2: Timeline: Sleep Medicine Throughout HistoryDocument5 pagesActivity 2: Timeline: Sleep Medicine Throughout HistoryDNAANo ratings yet
- Module 3 Lesson 3.1 For ResearchDocument18 pagesModule 3 Lesson 3.1 For ResearchJohn Clieford AdarayanNo ratings yet
- James L. OschmanDocument120 pagesJames L. Oschmannamkay_tenzyn100% (7)
- Isaac NewtonDocument3 pagesIsaac NewtonBlue Heavens100% (1)
- Biofeedback Human Energy FieldDocument60 pagesBiofeedback Human Energy FieldElianKitha100% (2)
- Cognitive NeuroscienceDocument7 pagesCognitive NeuroscienceoptiuneNo ratings yet
- Alexander Graham BellDocument3 pagesAlexander Graham BellMark Joseph Nepomuceno CometaNo ratings yet
- History of NeuroscienceDocument3 pagesHistory of Neurosciencemihaela irofteNo ratings yet
- Histology HistoryDocument5 pagesHistology HistoryEzekiel Morena RiveraNo ratings yet
- Timeline MineDocument1 pageTimeline MineJane Angela FerrerNo ratings yet
- An Appreciation of Sherrington's "The Integrative Action of The Nervous System"Document8 pagesAn Appreciation of Sherrington's "The Integrative Action of The Nervous System"saswepakNo ratings yet
- ParapsychologyDocument17 pagesParapsychologymamulasioan9675No ratings yet
- Stephen William HawkingDocument7 pagesStephen William HawkingJoshua DiazNo ratings yet
- Laboratory Activity No. 1 - PagtalunanDocument6 pagesLaboratory Activity No. 1 - PagtalunanRosette PagtalunanNo ratings yet
- Activity 1 PDFDocument7 pagesActivity 1 PDFRoland AbelaNo ratings yet
- 12 The Advent of Modern NeuroscienceDocument3 pages12 The Advent of Modern Neurosciencezym1003No ratings yet
- Calla, Lorelie L. 4 CR - 3E Contributions in PolygraphyDocument3 pagesCalla, Lorelie L. 4 CR - 3E Contributions in PolygraphyApple Santos Mabagos100% (1)
- Natur Philosophie 21Document33 pagesNatur Philosophie 21Ivan TalonNo ratings yet
- Tarea 2 Teoríacelular López Marmolejo Clere MishellDocument3 pagesTarea 2 Teoríacelular López Marmolejo Clere Mishellclere02marmolejoNo ratings yet
- Presvee Lara ADocument1 pagePresvee Lara AHazel MedranoNo ratings yet
- Brown Doodle Company Profile PresentationDocument13 pagesBrown Doodle Company Profile PresentationHAYDEE SUSTENTONo ratings yet
- Aphasia NoteDocument2 pagesAphasia NoteValentinus AlfrendoNo ratings yet
- A History of Sleep and DreamingDocument8 pagesA History of Sleep and DreamingtaniasuhinaNo ratings yet
- The Visual Scoring of Sleep in AdultsDocument11 pagesThe Visual Scoring of Sleep in AdultsMasyfuk Zuhdi JamhurNo ratings yet
- Brief History of Cell DiscoveryDocument3 pagesBrief History of Cell DiscoveryRobert Ford100% (1)
- Cell TheoryDocument3 pagesCell TheoryNovie Dave EstremaduraNo ratings yet
- Waking Up To The Problem of Sleep: Can Mindfulness Help? A Review of Theory and Evidence For The Effects of Mindfulness For SleepDocument5 pagesWaking Up To The Problem of Sleep: Can Mindfulness Help? A Review of Theory and Evidence For The Effects of Mindfulness For SleepJulian PintosNo ratings yet
- Ong 2017Document9 pagesOng 2017Lukas TmsNo ratings yet
- Blake 2017Document13 pagesBlake 2017Julian PintosNo ratings yet
- Update On Non-Pharmacological Interventions in Parasomnias: Postgraduate MedicineDocument23 pagesUpdate On Non-Pharmacological Interventions in Parasomnias: Postgraduate MedicineJulian PintosNo ratings yet
- Cognitive BehavioralTherapyDocument12 pagesCognitive BehavioralTherapyJulian PintosNo ratings yet
- Waking Up To The Problem of Sleep: Can Mindfulness Help? A Review of Theory and Evidence For The Effects of Mindfulness For SleepDocument5 pagesWaking Up To The Problem of Sleep: Can Mindfulness Help? A Review of Theory and Evidence For The Effects of Mindfulness For SleepJulian PintosNo ratings yet
- Blake 2017Document13 pagesBlake 2017Julian PintosNo ratings yet
- Cognitivebehavioral Therapyforsleep Disorders: Kimberly A. Babson,, Matthew T. Feldner,, Christal L. BadourDocument12 pagesCognitivebehavioral Therapyforsleep Disorders: Kimberly A. Babson,, Matthew T. Feldner,, Christal L. BadourJulian PintosNo ratings yet
- Practice Essentials: Ralph Downey, Iii, PHD Staff Sleep Specialist, Cleveland Clinic Foundation AssociateDocument18 pagesPractice Essentials: Ralph Downey, Iii, PHD Staff Sleep Specialist, Cleveland Clinic Foundation AssociateMaulana 'Sugat' Iskandar DinataNo ratings yet
- Icon Cpap Fisherpaykel Infosmart BrochureDocument2 pagesIcon Cpap Fisherpaykel Infosmart BrochureRob BriceNo ratings yet
- Night Sweats: A Systematic Review of The LiteratureDocument16 pagesNight Sweats: A Systematic Review of The LiteraturesyafahalimNo ratings yet
- Philips Titration Protocol 2017Document12 pagesPhilips Titration Protocol 2017Sam WhiteNo ratings yet
- Myofunctional TherapyDocument19 pagesMyofunctional Therapy許越隆No ratings yet
- Yel Cpap Yel Cpap 1587377064Document33 pagesYel Cpap Yel Cpap 1587377064Haitham yousifNo ratings yet
- Mandibular Movement Analysis To Assess Ef Ficacy of Oral Appliance Therapy in OSADocument8 pagesMandibular Movement Analysis To Assess Ef Ficacy of Oral Appliance Therapy in OSAZUNENo ratings yet
- 2003, Vol.24. Issues 2, Sleep DisordersDocument189 pages2003, Vol.24. Issues 2, Sleep Disorderssantiago_auteriNo ratings yet
- Sleep Apnea PDFDocument257 pagesSleep Apnea PDFdantevermillion100% (6)
- Obstructive Sleep Apnea and Orthodontics: An American Association of Orthodontists White PaperDocument17 pagesObstructive Sleep Apnea and Orthodontics: An American Association of Orthodontists White PaperIsa TorresNo ratings yet
- Mode Selection For Positive Airway Pressure Titration in Adult Patients With Central Sleep Apnea Syndromes - UpToDateDocument16 pagesMode Selection For Positive Airway Pressure Titration in Adult Patients With Central Sleep Apnea Syndromes - UpToDatedavimemNo ratings yet
- Classification of Sleep DisordersDocument15 pagesClassification of Sleep Disorderselvinegunawan100% (1)
- Treatment of Obstructive Sleep Apnea With Oral Appliances: Research Open AccessDocument9 pagesTreatment of Obstructive Sleep Apnea With Oral Appliances: Research Open AccessVinay MuppanaNo ratings yet
- MALLAMPATI Sleep-29-7-903Document6 pagesMALLAMPATI Sleep-29-7-903Jeisson Auqui GutierrezNo ratings yet
- 2010 Philips Respironics CatalogDocument148 pages2010 Philips Respironics CatalogAcilegna BNo ratings yet
- FND Sleep DisordersDocument10 pagesFND Sleep DisordersQuang VuNo ratings yet
- Respironics Dreamstation CpapDocument12 pagesRespironics Dreamstation CpapLowtech23No ratings yet
- Facts and Figures: Sleep ApneaDocument2 pagesFacts and Figures: Sleep ApneaNazir AhmadNo ratings yet
- Application of A Wireless Apnea Monitoring Device For Crisis Alertness and Sleep DiagnosisDocument8 pagesApplication of A Wireless Apnea Monitoring Device For Crisis Alertness and Sleep DiagnosisTELKOMNIKA100% (1)
- BMC RESmart ICode-Software User-ManualDocument13 pagesBMC RESmart ICode-Software User-ManualDamian GriffoNo ratings yet
- RespironicsDocument6 pagesRespironicsHuzur MezarNo ratings yet
- Sleep Apnea White Paper 2019Document53 pagesSleep Apnea White Paper 2019Majai Erzsebet Emoke EmyNo ratings yet
- Pediatric Sleep Questionnaire (PSQ) - Validity and ReliabilityDocument12 pagesPediatric Sleep Questionnaire (PSQ) - Validity and ReliabilitySabrina GurksnisNo ratings yet
- Philips Respironics Bipap ST Niv Noninvasive VentilatorDocument2 pagesPhilips Respironics Bipap ST Niv Noninvasive Ventilatorsonia87No ratings yet
- Pgi May 2012 Ebook PDFDocument50 pagesPgi May 2012 Ebook PDFloviNo ratings yet
- Signs and Symptoms of Obstructive Sleep Apnea and Upper Airway Resistance SyndromeDocument7 pagesSigns and Symptoms of Obstructive Sleep Apnea and Upper Airway Resistance SyndromeLuis De jesus SolanoNo ratings yet
- Sleep Apnea Syndrome &Document28 pagesSleep Apnea Syndrome &Sumit PuloriaNo ratings yet