You might also like
- Medical Journals Year in Body Mods 2012 12-30-12Document24 pagesMedical Journals Year in Body Mods 2012 12-30-12Hadi FirmansyahNo ratings yet
- Lower Blepharoplasty: How To Avoid Complications: Dr. Vincent KH KWANDocument3 pagesLower Blepharoplasty: How To Avoid Complications: Dr. Vincent KH KWANHadi FirmansyahNo ratings yet
- Medical Journals Year in Body Mods 2012 12-30-12Document24 pagesMedical Journals Year in Body Mods 2012 12-30-12Hadi FirmansyahNo ratings yet
- Bleomycin and The SkinDocument8 pagesBleomycin and The SkinHadi FirmansyahNo ratings yet
- 10 5923 J Surgery 20140301 03 PDFDocument4 pages10 5923 J Surgery 20140301 03 PDFJacobMsangNo ratings yet
- White Piedra in A Mother and DaughterDocument3 pagesWhite Piedra in A Mother and DaughterHadi FirmansyahNo ratings yet
- Bleomycin in The Treatment of Keloids and Hypertrophic Scars by Multiple Needle PuncturesDocument10 pagesBleomycin in The Treatment of Keloids and Hypertrophic Scars by Multiple Needle PuncturesHadi FirmansyahNo ratings yet
- Chae Et Al-2015-Journal of Cosmetic DermatologyDocument7 pagesChae Et Al-2015-Journal of Cosmetic DermatologyHadi FirmansyahNo ratings yet
- Co-Isolation of Trichosporon Inkin and CandidaDocument8 pagesCo-Isolation of Trichosporon Inkin and CandidaHadi FirmansyahNo ratings yet
- Treatment of Keloids and Hypertrophic ScarsDocument9 pagesTreatment of Keloids and Hypertrophic ScarsHadi FirmansyahNo ratings yet
- Wilske B. Epidemiology and Diagnosis of Lyme Borreliosis 2005Document12 pagesWilske B. Epidemiology and Diagnosis of Lyme Borreliosis 2005Hadi FirmansyahNo ratings yet
- JorgenDocument5 pagesJorgenHadi FirmansyahNo ratings yet
- Verrucous Lepromatous Leprosy A Rare Form ofDocument4 pagesVerrucous Lepromatous Leprosy A Rare Form ofHadi FirmansyahNo ratings yet
- Fatal Metastatic Cutaneous Squamous Cell Carcinoma Evolving From A Localized Verrucous Epidermal NevusDocument11 pagesFatal Metastatic Cutaneous Squamous Cell Carcinoma Evolving From A Localized Verrucous Epidermal NevusHadi FirmansyahNo ratings yet
- A Case of Basal Cell Carcinoma Arising in Epidermal Nevus: CameoDocument3 pagesA Case of Basal Cell Carcinoma Arising in Epidermal Nevus: CameoHadi FirmansyahNo ratings yet
- Collodion Baby and Loricrin Keratoderma: A Case Report and Mutation AnalysisDocument5 pagesCollodion Baby and Loricrin Keratoderma: A Case Report and Mutation AnalysisHadi FirmansyahNo ratings yet
- Lepromatous Leprosy A Case Simulating VerrucousDocument5 pagesLepromatous Leprosy A Case Simulating VerrucousHadi FirmansyahNo ratings yet
- New Developments in Ochronosis: Review of The LiteratureDocument6 pagesNew Developments in Ochronosis: Review of The LiteratureHadi FirmansyahNo ratings yet
- Xerosis CutisDocument6 pagesXerosis CutisHadi FirmansyahNo ratings yet
- Cutaneous Annular Sarcoidosis Developing On A Background of Exogenous Ochronosis: A Report of Two Cases and Review of The LiteratureDocument5 pagesCutaneous Annular Sarcoidosis Developing On A Background of Exogenous Ochronosis: A Report of Two Cases and Review of The LiteratureHadi FirmansyahNo ratings yet
- Thayer Martin Agar Procedure 08Document1 pageThayer Martin Agar Procedure 08Hadi FirmansyahNo ratings yet
- Xerosis CutisDocument6 pagesXerosis CutisHadi FirmansyahNo ratings yet
- Dermatologica Sinica: Cheng-Han Lee, Yi-Chun Chen, Yung-Tsu Cho, Chia-Ying Chang, Chia-Yu ChuDocument5 pagesDermatologica Sinica: Cheng-Han Lee, Yi-Chun Chen, Yung-Tsu Cho, Chia-Ying Chang, Chia-Yu ChuHadi FirmansyahNo ratings yet
- 1999 1 1 29 36Document8 pages1999 1 1 29 36Hadi FirmansyahNo ratings yet
- JorgenDocument5 pagesJorgenHadi FirmansyahNo ratings yet
- New Developments in Ochronosis: Review of The LiteratureDocument6 pagesNew Developments in Ochronosis: Review of The LiteratureHadi FirmansyahNo ratings yet
- Patch Test FDEDocument8 pagesPatch Test FDEHadi FirmansyahNo ratings yet
- Can P Rio Biotics Prevent VaginitisDocument2 pagesCan P Rio Biotics Prevent VaginitisHadi FirmansyahNo ratings yet
- 1486 - Vitamin D PaperDocument9 pages1486 - Vitamin D PaperHadi FirmansyahNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Webrep - Cgi 4Document1 pageWebrep - Cgi 4viridiana bonillaNo ratings yet
- HS - I Don't Feel Weel TodayDocument10 pagesHS - I Don't Feel Weel Todaychie NbaNo ratings yet
- Artesunato MefloquinaDocument11 pagesArtesunato MefloquinaDavid CerrónNo ratings yet
- Resbakuna - Comirnaty PoU Deck For Site Training and Education-FINAL-013122Document53 pagesResbakuna - Comirnaty PoU Deck For Site Training and Education-FINAL-013122toledanagerald516No ratings yet
- Community Project Proposal (Rabbi Petallar)Document2 pagesCommunity Project Proposal (Rabbi Petallar)Gerald Riate100% (1)
- Antibiotic Prophylaxis in Pediatric Odontology. An UpdateDocument6 pagesAntibiotic Prophylaxis in Pediatric Odontology. An UpdateJavier Farias VeraNo ratings yet
- SCREENING FOR DISEASEDocument15 pagesSCREENING FOR DISEASEDr. Radhay ShyamNo ratings yet
- Vaccine Guide - Randall NeustaedterDocument6 pagesVaccine Guide - Randall NeustaedterttreksNo ratings yet
- Awareness of Mother With Baby PacifierDocument10 pagesAwareness of Mother With Baby PacifierIJAR JOURNALNo ratings yet
- COA OB WardDocument17 pagesCOA OB WardChristian PasiliaoNo ratings yet
- Pamphlet TemplateDocument2 pagesPamphlet TemplateZoe ColemanNo ratings yet
- Fluids and Electrolytes in ElderlyDocument7 pagesFluids and Electrolytes in ElderlyDithaNo ratings yet
- Patient Care StudyDocument49 pagesPatient Care StudyKwabena AmankwaNo ratings yet
- Cabizares Handle CaseDocument8 pagesCabizares Handle CaseMae AbabonNo ratings yet
- Basic Principles of Nursing EthicsDocument2 pagesBasic Principles of Nursing Ethicsalena volinaNo ratings yet
- Asante Teaching Hospital Activity Based CostingDocument3 pagesAsante Teaching Hospital Activity Based CostingMuskanNo ratings yet
- Revised SNCU Mentoring ChecklistDocument6 pagesRevised SNCU Mentoring Checklistrani26octNo ratings yet
- 248-Article Text-614-1-10-20210714Document7 pages248-Article Text-614-1-10-20210714Abl ApriliaaNo ratings yet
- ASTHMADocument16 pagesASTHMAAyesigwa Gerald96100% (1)
- USMLE Images For The BoardsDocument297 pagesUSMLE Images For The BoardsMulham Etki100% (3)
- CDI Module 19: Behavior Change Communication: ©jhpiego Corporation The Johns Hopkins UniversityDocument34 pagesCDI Module 19: Behavior Change Communication: ©jhpiego Corporation The Johns Hopkins University420192420192No ratings yet
- History Patient - Co.ukDocument14 pagesHistory Patient - Co.ukiuytrerNo ratings yet
- Ncma217 Performancetask#5 TinioDocument7 pagesNcma217 Performancetask#5 TinioAndhee Mae TinioNo ratings yet
- World Health OrganizationDocument18 pagesWorld Health OrganizationsulyNo ratings yet
- MSEB - Claim - Form 2016 MahaGencoDocument2 pagesMSEB - Claim - Form 2016 MahaGencoAnonymous pKsr5vNo ratings yet
- Medical Act outlines requirements for medical practiceDocument13 pagesMedical Act outlines requirements for medical practiceCornelio AlfonsoNo ratings yet
- Global Epidemiology of Hepatitis B Virus (HBV) Infection: Elizabeth W. Hwang, MD, Ramsey Cheung, MDDocument7 pagesGlobal Epidemiology of Hepatitis B Virus (HBV) Infection: Elizabeth W. Hwang, MD, Ramsey Cheung, MDivan gartikaNo ratings yet
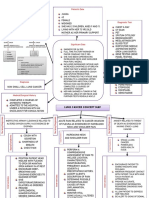
- Lung Cancer Concept Map-Group 2Document2 pagesLung Cancer Concept Map-Group 2Maria Cristina100% (2)
- The Hospital Formulary: Bilal Hassan M.Phil PharmaceuticsDocument11 pagesThe Hospital Formulary: Bilal Hassan M.Phil PharmaceuticsShafaqat Ghani Shafaqat GhaniNo ratings yet
- MT 1 NurseDocument36 pagesMT 1 NurseShipra dhingraNo ratings yet