You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Change4Life Marketing Strategy April09Document65 pagesChange4Life Marketing Strategy April09Leyla MajundaNo ratings yet
- Howard Marks - Mastering The Market CyclesDocument40 pagesHoward Marks - Mastering The Market Cyclessidbaba60% (5)
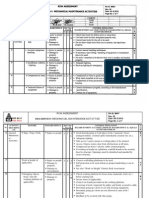
- Mechanical Maintenance ActivitesDocument7 pagesMechanical Maintenance ActivitesJhun Aquino50% (2)
- Organizational Change in Vale - EditedDocument13 pagesOrganizational Change in Vale - EditedBaisakhi ChatterjeeNo ratings yet
- 2 TACCP Doc 5.4.2 Vulnerability Assessment MatrixDocument10 pages2 TACCP Doc 5.4.2 Vulnerability Assessment MatrixNewhame Dagne100% (1)
- L3 24.6 Reading+writing You Can Be An EntrepreneurDocument20 pagesL3 24.6 Reading+writing You Can Be An EntrepreneurKuan LoongNo ratings yet
- A Noun Is A Name of A Person, Place or Thing.: Shoe Leaf BallDocument12 pagesA Noun Is A Name of A Person, Place or Thing.: Shoe Leaf BallKuan LoongNo ratings yet
- L2 21.6 Reading You Can Be An EntrepreneurDocument16 pagesL2 21.6 Reading You Can Be An EntrepreneurKuan LoongNo ratings yet
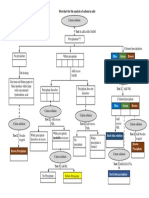
- Flowchart For The Analysis of Cations in Salts: Blue Green BrownDocument1 pageFlowchart For The Analysis of Cations in Salts: Blue Green BrownKuan LoongNo ratings yet
- Unknown Solid Anion: Test 1: Heating The SolidDocument1 pageUnknown Solid Anion: Test 1: Heating The SolidKuan LoongNo ratings yet
- Jadikan M Sebagai Perkara Rumus Bagi Setiap Berikut. 1. 2Document3 pagesJadikan M Sebagai Perkara Rumus Bagi Setiap Berikut. 1. 2Kuan Loong100% (1)
- Period 3 in The Periodic Table of ElementsDocument1 pagePeriod 3 in The Periodic Table of ElementsKuan LoongNo ratings yet
- Example: +2 or 2, +7 or 7, 8, 12Document6 pagesExample: +2 or 2, +7 or 7, 8, 12Kuan LoongNo ratings yet
- Exe Melting and BoilingDocument3 pagesExe Melting and BoilingKuan LoongNo ratings yet
- Biology Chapter 1Document7 pagesBiology Chapter 1Kuan LoongNo ratings yet
- Square Square RootDocument2 pagesSquare Square RootKuan LoongNo ratings yet
- Multiple of A Number The Product of That Number and Another Non-Zero Whole NumberDocument6 pagesMultiple of A Number The Product of That Number and Another Non-Zero Whole NumberKuan LoongNo ratings yet
- Exercise MicroorganismDocument2 pagesExercise MicroorganismKuan Loong0% (1)
- TaskDocument1 pageTaskKuan LoongNo ratings yet
- Ppgs 6141 Pentaksiran Dalam Kaunseling PerkhidmatanDocument2 pagesPpgs 6141 Pentaksiran Dalam Kaunseling PerkhidmatanKuan LoongNo ratings yet
- The Role of Career Counselling Influencing UM Students in Their Career ChoiceDocument3 pagesThe Role of Career Counselling Influencing UM Students in Their Career ChoiceKuan LoongNo ratings yet
- Sayangi MasyarakatDocument12 pagesSayangi MasyarakatKuan LoongNo ratings yet
- Corporate GovernanceDocument46 pagesCorporate GovernancevirajNo ratings yet
- Safety and Risk Ping PongDocument2 pagesSafety and Risk Ping PongIsenn INo ratings yet
- Umbrio Concept Note For Jaura Infratech - Building A Strong Workplace Through Creating Engaged WorkforceDocument42 pagesUmbrio Concept Note For Jaura Infratech - Building A Strong Workplace Through Creating Engaged WorkforceAyesha ShroffNo ratings yet
- Retail Banking and Wealth ManagementDocument36 pagesRetail Banking and Wealth ManagementSAMBITPRIYADARSHINo ratings yet
- Whistleblowing in A Changing Legal Climate Is It Time To Revisit Our Approach To Trust and Loyalty at The WorkplaceDocument17 pagesWhistleblowing in A Changing Legal Climate Is It Time To Revisit Our Approach To Trust and Loyalty at The WorkplacecshadowsmeNo ratings yet
- UR3 User Manual en USDocument205 pagesUR3 User Manual en USTADEOULISESNo ratings yet
- EMA Guideline On Computerised Systems and Electronic Data in Clinical TrialsDocument52 pagesEMA Guideline On Computerised Systems and Electronic Data in Clinical TrialsHoàng Ngọc AnhNo ratings yet
- Political Risk Factors and TheirDocument21 pagesPolitical Risk Factors and TheircrsalinasNo ratings yet
- Risk and ReturnsDocument17 pagesRisk and ReturnsLeica Jayme100% (1)
- A Report On Three Different Cases of Company Investments Happening NowDocument5 pagesA Report On Three Different Cases of Company Investments Happening NowNadia RiazNo ratings yet
- Invitational 2020 2ndDocument36 pagesInvitational 2020 2ndÁnh Thiện TriệuNo ratings yet
- Chandelier Hoist SystemDocument10 pagesChandelier Hoist SystemNishadh 83No ratings yet
- ProposalDocument12 pagesProposalJon Rexor GomezNo ratings yet
- On Site Emergency Plan - Sep 2020Document115 pagesOn Site Emergency Plan - Sep 2020Raj Goswami100% (3)
- SWMS-HYD-VAYUCON-03 - Unloading and Shifting Material Through ForkliftDocument7 pagesSWMS-HYD-VAYUCON-03 - Unloading and Shifting Material Through ForkliftBodakunta Ajay VarmaNo ratings yet
- EPM-KSH-PR-000007 - 02 Project Control of Hazardous Materials ProcedureDocument12 pagesEPM-KSH-PR-000007 - 02 Project Control of Hazardous Materials Procedureamr AboelnagaNo ratings yet
- CommRev CasesDocument30 pagesCommRev CasesanjisyNo ratings yet
- ITAF-Companion-Performance-Guidelines-2208 wpg2208 Res Eng 1020Document20 pagesITAF-Companion-Performance-Guidelines-2208 wpg2208 Res Eng 1020Florencio CossaNo ratings yet
- TR - Aquaculture NC IIDocument64 pagesTR - Aquaculture NC IIherbert rebloraNo ratings yet
- Module 3 Lesson 6Document4 pagesModule 3 Lesson 6John Benz SamsonNo ratings yet
- Trading Plan TemplateDocument13 pagesTrading Plan TemplateKrishnamurthy HegdeNo ratings yet
- Mgh-Jun-02072022-1233pm-Krm Thesis-Ch2 - 1500Document35 pagesMgh-Jun-02072022-1233pm-Krm Thesis-Ch2 - 1500Dababrata SahaNo ratings yet
- A Report On Strategic Management of National Bank LimitedDocument36 pagesA Report On Strategic Management of National Bank LimitedNabila AhmadNo ratings yet
- Audit KYC AND CDDDocument16 pagesAudit KYC AND CDDHemant MishraNo ratings yet