You might also like
- Fibrinolysis Laboratory TestDocument2 pagesFibrinolysis Laboratory TestMark Vincent SahagunNo ratings yet
- Evaluation Tests For Secondary Hemostasis (Lab Analysis) HematologyDocument5 pagesEvaluation Tests For Secondary Hemostasis (Lab Analysis) HematologyAudreySlitNo ratings yet
- Ordonez V CA GR No. 84046 July 30, 1990 by - YrreverreDocument1 pageOrdonez V CA GR No. 84046 July 30, 1990 by - YrreverreBrian DuffyNo ratings yet
- Bleeding Disorders: Hemorrhagic Diathesis: Frederick R. Llanera, MD, FPSP, Ascpi, Amt, RMTDocument29 pagesBleeding Disorders: Hemorrhagic Diathesis: Frederick R. Llanera, MD, FPSP, Ascpi, Amt, RMTRaymond MalubayNo ratings yet
- The Impossible Dream: A Reflection on Achieving EquityDocument3 pagesThe Impossible Dream: A Reflection on Achieving EquityFrancis LeaNo ratings yet
- VIRAL RESPIRATORY DISEASESDocument11 pagesVIRAL RESPIRATORY DISEASESmiguel gaquitNo ratings yet
- Hematology 2 Lecture Notes Platelet Qualitative DisordersDocument4 pagesHematology 2 Lecture Notes Platelet Qualitative DisorderscccomayogNo ratings yet
- Exfoliative CytologyDocument1 pageExfoliative CytologyNathaniel SimNo ratings yet
- 2ndquarter Lp1 Literal and Figurative BiaDocument6 pages2ndquarter Lp1 Literal and Figurative BiaBianca Nicole CesistaNo ratings yet
- Organic Halide Classification TestsDocument3 pagesOrganic Halide Classification TestsROSEMARIE ONGNo ratings yet
- Domestic Violence JennyDocument20 pagesDomestic Violence JennyjuliusdarianNo ratings yet
- 7 Developmental, Genetic, & Pediatric DiseaseDocument62 pages7 Developmental, Genetic, & Pediatric DiseasecamsfNo ratings yet
- Thyroid & Parathyroid GlandsDocument21 pagesThyroid & Parathyroid GlandsAzizan HannyNo ratings yet
- Therapeutic Drug MonitoringDocument5 pagesTherapeutic Drug MonitoringJanielle Medina FajardoNo ratings yet
- Hepatotoxicity, Vasculitis:: Pruritic Rash, Arthralgias-Joint Pain, AgranulocytosisDocument3 pagesHepatotoxicity, Vasculitis:: Pruritic Rash, Arthralgias-Joint Pain, AgranulocytosisThuan Tăng NguyenNo ratings yet
- Mixing StudiesDocument14 pagesMixing StudiesHery PriyantoNo ratings yet
- BloodDocument9 pagesBloodSheena PasionNo ratings yet
- HemopoiesisDocument22 pagesHemopoiesisSheena PasionNo ratings yet
- Inquiry (5E) Lesson Plan Template: Teachers: Ashley Moss Subject: Honors English Grade: 12Document2 pagesInquiry (5E) Lesson Plan Template: Teachers: Ashley Moss Subject: Honors English Grade: 12api-488398773No ratings yet
- Patho Unit 4.1Document20 pagesPatho Unit 4.1Lily ChouNo ratings yet
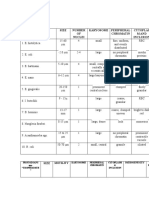
- Table 1: Protozoans Spp. "CYSTS" Size Number OF Nuclei Karyosome Peripheral Chromatin Cytoplas M and InclusionDocument3 pagesTable 1: Protozoans Spp. "CYSTS" Size Number OF Nuclei Karyosome Peripheral Chromatin Cytoplas M and InclusionJoshua TrinidadNo ratings yet
- Prothrombin Time (PT) PDFDocument3 pagesProthrombin Time (PT) PDFbongbongz8646100% (2)
- The Lymphatic System and Non-Immune ResponseDocument11 pagesThe Lymphatic System and Non-Immune ResponseSheena PasionNo ratings yet
- Nervous System - HistologyDocument8 pagesNervous System - HistologyambercrisologoNo ratings yet
- Qualitative Platelet DisordersDocument34 pagesQualitative Platelet Disordersalibayaty10% (1)
- Micro para OSCE For YL6 BacteriaDocument2 pagesMicro para OSCE For YL6 Bacteriagzldiwa100% (1)
- Hypersensitivity Reaction/ AllergyDocument23 pagesHypersensitivity Reaction/ AllergyCharity Grace MagnoNo ratings yet
- Therapeutic Drug Monitoring in The ElderlyDocument3 pagesTherapeutic Drug Monitoring in The ElderlyKristine BaringNo ratings yet
- Enzyme Histochemistry Techniques for Tissue Preservation and AnalysisDocument4 pagesEnzyme Histochemistry Techniques for Tissue Preservation and AnalysisKristine Baring50% (2)
- Microbiology Course SyllabusDocument3 pagesMicrobiology Course SyllabusTommy Ngo0% (1)
- 08.30 2021 IA Histology S1T4 Cartilage and BoneDocument11 pages08.30 2021 IA Histology S1T4 Cartilage and BoneAman SinghNo ratings yet
- Salivary Gland Carcinoma PresentationDocument34 pagesSalivary Gland Carcinoma PresentationIAMSANWAR019170No ratings yet
- RRLDocument96 pagesRRLKristiene Kyle AquinoNo ratings yet
- Evangelium VitaeDocument28 pagesEvangelium VitaeTobiasNo ratings yet
- AnaPhy Lab Exercise 24-41Document6 pagesAnaPhy Lab Exercise 24-41Angelyka Cabalo50% (2)
- Muscle Tissue OutlineDocument4 pagesMuscle Tissue OutlinePeachy PieNo ratings yet
- Microbiology ReviewerDocument21 pagesMicrobiology ReviewerJulianne BalquinNo ratings yet
- Tissue TableDocument4 pagesTissue TableMarcie BooneNo ratings yet
- Amniotic Fluid AubfDocument5 pagesAmniotic Fluid AubfVicky ChanNo ratings yet
- Cardiovascular Disorders StudentsDocument46 pagesCardiovascular Disorders StudentsPye Antwan DelvaNo ratings yet
- Immediate Hemolytic Transfusion ReactionDocument2 pagesImmediate Hemolytic Transfusion ReactionleoNo ratings yet
- Exercise 1 Gametogenesis ReviewerDocument4 pagesExercise 1 Gametogenesis ReviewerJasper AdonisNo ratings yet
- Case Study AsthmaDocument11 pagesCase Study AsthmaJaya ShriNo ratings yet
- Objectives: at The End of This Activity, You Should Be Able ToDocument3 pagesObjectives: at The End of This Activity, You Should Be Able ToArriane AndayaNo ratings yet
- Nose and Paranasal SinusesDocument4 pagesNose and Paranasal SinusesAlloiBialbaNo ratings yet
- Org Chem Ost LabDocument21 pagesOrg Chem Ost Labjullian marasiganNo ratings yet
- Cerebrovascular DiseasesDocument16 pagesCerebrovascular DiseasesSopna ZenithNo ratings yet
- Gram Staining 01Document11 pagesGram Staining 01MARICAR RAFAELNo ratings yet
- Experiment-4 (Clotting Time)Document4 pagesExperiment-4 (Clotting Time)Eva Luviriani75% (4)
- Fluorescent Treponemal Antibody Absorption FTA ABS TestDocument22 pagesFluorescent Treponemal Antibody Absorption FTA ABS TestMekar PalupiNo ratings yet
- Atopic DermatitisDocument9 pagesAtopic DermatitisJorge De VeraNo ratings yet
- Introduction To PathophysiologyDocument29 pagesIntroduction To PathophysiologystevencongressNo ratings yet
- Lesson Plan English 7 Parts of SpeechDocument7 pagesLesson Plan English 7 Parts of SpeechBianca Nicole CesistaNo ratings yet
- Mechanisms of Antimicrobial Resistance and ActionDocument5 pagesMechanisms of Antimicrobial Resistance and ActionJJ AngNo ratings yet
- Nematodes-Reviewer (Revised)Document4 pagesNematodes-Reviewer (Revised)Primo GeorgeNo ratings yet
- The Immune System: Department of Histology & EmbryologyDocument68 pagesThe Immune System: Department of Histology & EmbryologymookandpoppyNo ratings yet
- Platelet Counting Fordirect Indirect MethodDocument30 pagesPlatelet Counting Fordirect Indirect MethodShana Flame Haze100% (2)
- Baldomero Roxas Memorial Lecture 2017 The Triumph of Science Over Death PDFDocument7 pagesBaldomero Roxas Memorial Lecture 2017 The Triumph of Science Over Death PDFAngel PasaholNo ratings yet
- Impetigo2Document4 pagesImpetigo2Coral Srinivasa RamaluNo ratings yet
- 14 PapsDocument8 pages14 PapsReg LagartejaNo ratings yet
- Item IDocument123 pagesItem IFait HeeNo ratings yet
- EXECUTIVE ORDER NO. 200 June 18, 1987 (Links To An External Site.)Document5 pagesEXECUTIVE ORDER NO. 200 June 18, 1987 (Links To An External Site.)Fait HeeNo ratings yet
- 31Document2 pages31Fait HeeNo ratings yet
- Digests TST StsDocument18 pagesDigests TST StsFait HeeNo ratings yet
- ContinuationDocument2 pagesContinuationFait HeeNo ratings yet
- NationalityDocument85 pagesNationalityFait HeeNo ratings yet
- NationalityDocument85 pagesNationalityFait HeeNo ratings yet
- 2020 PALE OutlineDocument10 pages2020 PALE OutlineRyoNo ratings yet
- Transpo Digests 11 20Document11 pagesTranspo Digests 11 20Phoebe BalubarNo ratings yet
- Cir V. Ca G.R. No. 119322 FactsDocument2 pagesCir V. Ca G.R. No. 119322 FactsFait HeeNo ratings yet
- LTD HomeworkDocument52 pagesLTD HomeworkFait HeeNo ratings yet
- Mactan Cebu Airport Authority Tax Exemption RepealDocument34 pagesMactan Cebu Airport Authority Tax Exemption RepealFait Hee100% (1)
- 31Document2 pages31Fait HeeNo ratings yet
- PALE Pre NoteDocument22 pagesPALE Pre NoteFait HeeNo ratings yet
- Adr ReportDocument2 pagesAdr ReportFait HeeNo ratings yet
- HLI Full TextDocument224 pagesHLI Full TextFait HeeNo ratings yet
- Lutz vs. Araneta, 98 Phil 148, G.R. No. L-7859, 22 December 1955Document7 pagesLutz vs. Araneta, 98 Phil 148, G.R. No. L-7859, 22 December 1955Fait HeeNo ratings yet
- Court Rules on Validity of Contracts of Sale and Homestead PatentsDocument3 pagesCourt Rules on Validity of Contracts of Sale and Homestead PatentsFait HeeNo ratings yet
- Complement SystemDocument4 pagesComplement SystemFait HeeNo ratings yet
- Cred CasesDocument22 pagesCred CasesFait HeeNo ratings yet
- Virology FinalsDocument8 pagesVirology FinalsFait HeeNo ratings yet
- Cases - Consti 2 022417 Priority Cases 2Document75 pagesCases - Consti 2 022417 Priority Cases 2Fait HeeNo ratings yet
- Registered Land Sale DeedDocument2 pagesRegistered Land Sale DeedFait Hee100% (1)
- Case Digest - Legal Ethics 020417Document16 pagesCase Digest - Legal Ethics 020417Fait HeeNo ratings yet
- Case Digest - Consti 2 Ang Tibay - PurugananDocument67 pagesCase Digest - Consti 2 Ang Tibay - PurugananFait HeeNo ratings yet
- Rule 126Document3 pagesRule 126Carlie MaeNo ratings yet
- Ra 7719 Blood Bank MT-B & C 8Document7 pagesRa 7719 Blood Bank MT-B & C 8Fait Hee100% (1)
- PFR Digests 2Document8 pagesPFR Digests 2Fait HeeNo ratings yet
- Case - Crim 2 People Vs Garcia 021517Document7 pagesCase - Crim 2 People Vs Garcia 021517Fait HeeNo ratings yet
- Cred CasesDocument22 pagesCred CasesFait HeeNo ratings yet
- S. G. Silverberg (Ed) : Principles and Practice of Surgical Pathology and Cytopathology. Churchill LivingstoneDocument1 pageS. G. Silverberg (Ed) : Principles and Practice of Surgical Pathology and Cytopathology. Churchill LivingstoneasadsNo ratings yet
- T.Y.B.Sc. - Medical Tech. - 2019Document26 pagesT.Y.B.Sc. - Medical Tech. - 2019PareshNo ratings yet
- Principles of Medical Laboratory Science PracticeDocument14 pagesPrinciples of Medical Laboratory Science PracticeJanna EchavezNo ratings yet
- Advantage and Disadvantage of FNACDocument13 pagesAdvantage and Disadvantage of FNACDebayan KarmakarNo ratings yet
- The Role of the Forensic Pathologist ExplainedDocument26 pagesThe Role of the Forensic Pathologist Explainedzahari0% (1)
- HPV Testing in The Follow-Up of Women Post Colposcopy Treatment - Final VersionDocument16 pagesHPV Testing in The Follow-Up of Women Post Colposcopy Treatment - Final VersionPaulo César López BarrientosNo ratings yet
- Dr. Rajasekhar A. National Pathology Laboratory HyderabadDocument26 pagesDr. Rajasekhar A. National Pathology Laboratory HyderabadAmit KumarNo ratings yet
- Guide For SmeartakersDocument168 pagesGuide For SmeartakersMc CoralNo ratings yet
- 2s2022 Ncm109 Rle Learn Mat 1Document18 pages2s2022 Ncm109 Rle Learn Mat 1Guia SalandananNo ratings yet
- Cytology - Clinical Pathology and Procedures - Merck Veterinary Manual PDFDocument14 pagesCytology - Clinical Pathology and Procedures - Merck Veterinary Manual PDFJD46No ratings yet
- Histology StainsDocument7 pagesHistology StainsFrozenMan100% (2)
- Download Canine And Feline Cytology A Color Atlas And Interpretation Guide 3E 3Rd Edition Rose E Raskin full chapterDocument67 pagesDownload Canine And Feline Cytology A Color Atlas And Interpretation Guide 3E 3Rd Edition Rose E Raskin full chapterrosanne.hahn846100% (2)
- Histology Stain GuideDocument9 pagesHistology Stain GuideSheba Dan de WiseNo ratings yet
- Breast Fine Needle Aspiration Cytology Reporting Icet13i2p54Document6 pagesBreast Fine Needle Aspiration Cytology Reporting Icet13i2p54salijanstarNo ratings yet
- Principles and Practice of Veterinary Technology e Book 4th Edition Ebook PDFDocument62 pagesPrinciples and Practice of Veterinary Technology e Book 4th Edition Ebook PDFhelen.fico427100% (35)
- Cervical Pap Smear Study in a Tertiary HospitalDocument4 pagesCervical Pap Smear Study in a Tertiary HospitalkushalNo ratings yet
- Case-Cancer Diagnostics and Therapeutics Exercise - TaggedDocument4 pagesCase-Cancer Diagnostics and Therapeutics Exercise - TaggedAhmed SahilNo ratings yet
- AIMS Professional Examination PackDocument13 pagesAIMS Professional Examination PackKaung Zaw SheinNo ratings yet
- Laboratory Diagnosis of InfectionDocument4 pagesLaboratory Diagnosis of InfectionHairul Anuar100% (1)
- Hematology ManualDocument233 pagesHematology ManualharpreetNo ratings yet
- J Janardhan, P Venkateshwar, K Sreedhar Rao, K Sreedhar RaoDocument5 pagesJ Janardhan, P Venkateshwar, K Sreedhar Rao, K Sreedhar RaoNatalindah Jokiem Woecandra T. D.No ratings yet
- Gram StainingDocument37 pagesGram StainingdhanyaNo ratings yet
- Specifications: (Endobronchial Ultrasound Application)Document4 pagesSpecifications: (Endobronchial Ultrasound Application)Ingrid SanchezNo ratings yet
- UntitledDocument264 pagesUntitledFed Espiritu Santo GNo ratings yet
- Loresca - Ratio Mtle - HistopathDocument10 pagesLoresca - Ratio Mtle - HistopathKaycee Gretz LorescaNo ratings yet
- Clinical Effects of NeoplasiaDocument12 pagesClinical Effects of NeoplasiaGhazi Uddin AhmedNo ratings yet
- SOP CYTO UpdatedDocument39 pagesSOP CYTO UpdatedDEEPAK SINGH SANGWANNo ratings yet
- Liquid-Based Cytology (LBC) Method For Gynecologic CytologyDocument79 pagesLiquid-Based Cytology (LBC) Method For Gynecologic CytologyIndonesian Journal of CancerNo ratings yet
- Clsi GP20 A2Document44 pagesClsi GP20 A2Cristian Gutiérrez VeraNo ratings yet
- Respiratory Cytology I PDFDocument13 pagesRespiratory Cytology I PDFafdsdgsd100% (1)