You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Hsdpa and Hspa DimensioningDocument106 pagesHsdpa and Hspa DimensioningTAOUACHINo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Adjacent Channel Interference Impact On The Capacity of Wcdma FDDDocument5 pagesAdjacent Channel Interference Impact On The Capacity of Wcdma FDDTAOUACHINo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- EUL OptimizationDocument41 pagesEUL OptimizationAlexander BabkinNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- (Huawei) WCDMA RAN AbbreviationDocument18 pages(Huawei) WCDMA RAN Abbreviationfofinho1No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- 002 WCDMA Radio Interface Physical LayerDocument60 pages002 WCDMA Radio Interface Physical LayerTAOUACHINo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Huawei Training & CertificationDocument24 pagesHuawei Training & CertificationMario Emiliano GordonNo ratings yet
- Post-Stroke Lower Limb Spasticity Alters The Interlimb Temporal Synchronisation of Centre of Pressure Displacements Across Multiple TimescalesDocument10 pagesPost-Stroke Lower Limb Spasticity Alters The Interlimb Temporal Synchronisation of Centre of Pressure Displacements Across Multiple TimescalesTAOUACHINo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- 00032106Document8 pages00032106TAOUACHINo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- 06776731Document6 pages06776731TAOUACHINo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Improved Biomedical Device For Spasticity QuantificationDocument4 pagesImproved Biomedical Device For Spasticity QuantificationTAOUACHINo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Haptic Simulation of Elbow Joint SpasticityDocument2 pagesHaptic Simulation of Elbow Joint SpasticityTAOUACHINo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Quick Start - SPU (V100R006C00 - 02)Document39 pagesQuick Start - SPU (V100R006C00 - 02)TAOUACHINo ratings yet
- 06168540Document6 pages06168540TAOUACHINo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Sample HF ArchitectureDocument1 pageSample HF ArchitectureTAOUACHINo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Radio Bearer Reconfiguration ExtractDocument1 pageRadio Bearer Reconfiguration ExtractTAOUACHINo ratings yet
- RANAP RAB Assignment Request For A CS Video CallDocument1 pageRANAP RAB Assignment Request For A CS Video CallTAOUACHINo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- RRC Messages ListDocument1 pageRRC Messages ListTAOUACHINo ratings yet
- RANAP RAB Assignment Response MessageDocument1 pageRANAP RAB Assignment Response MessageTAOUACHINo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- RRC Messages Associated With Each SRBDocument1 pageRRC Messages Associated With Each SRBTAOUACHINo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- RANAP RAB Assignment Response Message 2Document1 pageRANAP RAB Assignment Response Message 2TAOUACHINo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- RANAP Location Reporting Control MessageDocument1 pageRANAP Location Reporting Control MessageTAOUACHINo ratings yet
- RANAP RAB Assignment Request For PS Data CallDocument1 pageRANAP RAB Assignment Request For PS Data CallTAOUACHINo ratings yet
- RANAP Paging MessageDocument1 pageRANAP Paging MessageTAOUACHINo ratings yet
- RANAP RAB Assignment Request For A CS Speech CallDocument1 pageRANAP RAB Assignment Request For A CS Speech CallTAOUACHINo ratings yet
- RANAP Common Identity MessageDocument1 pageRANAP Common Identity MessageTAOUACHINo ratings yet
- Paging Type 1 MessageDocument1 pagePaging Type 1 MessageTAOUACHINo ratings yet
- Compressed Mode Using SFdiv2 - HLSDocument1 pageCompressed Mode Using SFdiv2 - HLSTAOUACHINo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- RANAP Messages ListDocument1 pageRANAP Messages ListTAOUACHINo ratings yet
- Soft HO Event 1a 1b 1cDocument1 pageSoft HO Event 1a 1b 1cTAOUACHINo ratings yet
- Gen. Zoo. Final ReviewerDocument34 pagesGen. Zoo. Final ReviewerAshley FranciscoNo ratings yet
- Human Genome Editing: Science, Ethics, and GovernanceDocument261 pagesHuman Genome Editing: Science, Ethics, and GovernanceAnonymous 6VKlaeigViNo ratings yet
- Pharyngeal ArchesDocument35 pagesPharyngeal ArchesconstantinilieNo ratings yet
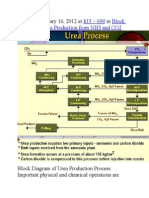
- Published January 16, 2012 at In: 813 × 699 Block Diagram of Urea Production From NH3 and CO2Document9 pagesPublished January 16, 2012 at In: 813 × 699 Block Diagram of Urea Production From NH3 and CO2himanshuchawla654No ratings yet
- LPL - Amit Sharma FPSC Loni Road-Gzb Shop No-4, Saharanpur Road, Loni Road, Main Tiraha, Loni, Ghaziabad, Loni S.ODocument3 pagesLPL - Amit Sharma FPSC Loni Road-Gzb Shop No-4, Saharanpur Road, Loni Road, Main Tiraha, Loni, Ghaziabad, Loni S.OKaran PrabhakarNo ratings yet
- Anatomy and PhysiologyPREFACEDocument3 pagesAnatomy and PhysiologyPREFACEtortenhumNo ratings yet
- Manage Your Personal Energy PDFDocument46 pagesManage Your Personal Energy PDFezhil manickamNo ratings yet
- Analisis AlantoinaDocument6 pagesAnalisis Alantoinarsevilla3No ratings yet
- ART - Spectrophotometric Method For Determining GA in ..Document4 pagesART - Spectrophotometric Method For Determining GA in ..Azahara Linares100% (2)
- OB Ultrasound Report Template 2Document1 pageOB Ultrasound Report Template 2PriyankaNo ratings yet
- 3 - Plasma Membrane and Transport MechanismsDocument67 pages3 - Plasma Membrane and Transport MechanismsThom PaglinawanNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Kleinman Culture and DepressionDocument3 pagesKleinman Culture and DepressionАлександра Курленкова100% (1)
- Skin and Body Membranes: EssentialsDocument43 pagesSkin and Body Membranes: EssentialsJohn Rex Lloyd TunaNo ratings yet
- Study Guide Cardio Tayang by Gextha 30 Maret 2015Document82 pagesStudy Guide Cardio Tayang by Gextha 30 Maret 2015Adi ParamarthaNo ratings yet
- 1st Summative Exam in General Biology 2Document1 page1st Summative Exam in General Biology 2Eula Pacifico100% (1)
- 300 One Word Substitutions Asked in SSC IBPS UPSC ExamDocument12 pages300 One Word Substitutions Asked in SSC IBPS UPSC ExamRashid AliNo ratings yet
- Email To Professor SampleDocument6 pagesEmail To Professor SamplesimplecobraNo ratings yet
- Duels and DuetsDocument253 pagesDuels and DuetsM Xenia0% (1)
- 19 - Lipid MetabolismDocument35 pages19 - Lipid MetabolismcheckmateNo ratings yet
- Nominalization (Exercise)Document2 pagesNominalization (Exercise)KryzQuinonesNo ratings yet
- CLS Aipmt 15 16 XIII Zoo Study Package 2 Set 1 Chapter 3Document30 pagesCLS Aipmt 15 16 XIII Zoo Study Package 2 Set 1 Chapter 3Santu Karmakar100% (1)
- Recent DevelopmentsDocument295 pagesRecent DevelopmentsGabriel PinheiroNo ratings yet
- Muscle Biopsy A Diagnostic Tool in Muscle DiseasesDocument9 pagesMuscle Biopsy A Diagnostic Tool in Muscle DiseasesRosa AquinoNo ratings yet
- Meriem Chatti - RéférencesDocument22 pagesMeriem Chatti - RéférencesOussama SghaïerNo ratings yet
- Sri Roth 2000Document11 pagesSri Roth 2000ottoojuniiorNo ratings yet
- Alvin MDocument2 pagesAlvin MRunmel Emmanuel Ramal DampiosNo ratings yet
- Weekly Home Learning Plan: Day/Time Learning Competency Learning Tasks Mode of DeliveryDocument4 pagesWeekly Home Learning Plan: Day/Time Learning Competency Learning Tasks Mode of DeliveryEricha SolomonNo ratings yet
- Fundamental Aspects of Sitting and StandingDocument2 pagesFundamental Aspects of Sitting and StandingMeenakshi SinghNo ratings yet
- Artikel SkripsiDocument12 pagesArtikel SkripsiSari RofiqohNo ratings yet
- CAPE Bio Mark SchemeDocument4 pagesCAPE Bio Mark Schemeron97150% (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (24)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)