You might also like
- Drugs Used in Gastrointestinal Diseases FinalDocument30 pagesDrugs Used in Gastrointestinal Diseases FinalFaridah Yuwono 28No ratings yet
- Pharmacology ReviewDocument172 pagesPharmacology ReviewJan Patrick Arrieta100% (1)
- Emergency Contraception and Emergency Contraceptive Pills (ECPs)Document39 pagesEmergency Contraception and Emergency Contraceptive Pills (ECPs)cafemed100% (1)
- Anti Inflammatory DrugsDocument82 pagesAnti Inflammatory DrugsShardendu MishraNo ratings yet
- Pharmacology2 (Drug Receptors & Pharmacodynamics)Document58 pagesPharmacology2 (Drug Receptors & Pharmacodynamics)Durge Raj Ghalan100% (2)
- Pharmacology of The GIT System: CIC Ragasa, RN-MDDocument70 pagesPharmacology of The GIT System: CIC Ragasa, RN-MDCarmencita Ileen Ragasa - AhmedNo ratings yet
- Cardiovascular Agents ReviewerDocument18 pagesCardiovascular Agents ReviewerJoycel CeñidozaNo ratings yet
- Chapter 13 PharmacologyDocument35 pagesChapter 13 PharmacologyEdelrose LapitanNo ratings yet
- Pharma CNS DRUGS Part 1Document13 pagesPharma CNS DRUGS Part 1reference booksNo ratings yet
- NCM 107 1.2Document2 pagesNCM 107 1.2Clint Mikael EulatrizNo ratings yet
- Anti-Infectives and AntibioticsDocument38 pagesAnti-Infectives and AntibioticsKarel Lu0% (1)
- Cardiotonic Medications: Drugs Used To For Patients Experiencing Heart FailureDocument28 pagesCardiotonic Medications: Drugs Used To For Patients Experiencing Heart FailureMoxie MacadoNo ratings yet
- PHRM 246: MR Thabiso Tlaila Department of Pharmacology Discipline of Pharmaceutical Sciences University of Kwazulu-NatalDocument38 pagesPHRM 246: MR Thabiso Tlaila Department of Pharmacology Discipline of Pharmaceutical Sciences University of Kwazulu-NatalSindile MchunuNo ratings yet
- Drugs For Immune SystemDocument75 pagesDrugs For Immune SystemDhonat FlashNo ratings yet
- GIT DrugsDocument180 pagesGIT DrugsMaria Linevel Balderamos Dalida100% (1)
- Anti-Infective Pharmacology ReviewerDocument5 pagesAnti-Infective Pharmacology ReviewerArianne Pearl PrimeroNo ratings yet
- Pharmacology Mock Exam MCQDocument8 pagesPharmacology Mock Exam MCQanaeshklNo ratings yet
- Factors Affecting Drug ActionDocument3 pagesFactors Affecting Drug ActionHempriya Tomar0% (1)
- Introduction To CNS PharmacologyDocument9 pagesIntroduction To CNS PharmacologyAbraham Daniel Campo Cruz100% (1)
- Nutrition and Malnutrition Resource UnitDocument22 pagesNutrition and Malnutrition Resource UnitMitch GatdulaNo ratings yet
- Drugs acting on the Cardiovascular SystemDocument18 pagesDrugs acting on the Cardiovascular SystemIbrahem AlNo ratings yet
- GI Pharmacology OverviewDocument24 pagesGI Pharmacology OverviewjenniferluzonNo ratings yet
- Drugs For GI DisordersDocument5 pagesDrugs For GI DisordersAalap ShahNo ratings yet
- Pharmacology: By: Nerissa Cabañero Laiza PinedaDocument121 pagesPharmacology: By: Nerissa Cabañero Laiza PinedaJacq CalaycayNo ratings yet
- Module 1.1 Presentation (B2)Document15 pagesModule 1.1 Presentation (B2)Jan Lianne BernalesNo ratings yet
- Appendix A: National Unified Health Research Agenda A. DiagnosticsDocument10 pagesAppendix A: National Unified Health Research Agenda A. DiagnosticsKit ChampNo ratings yet
- Chapter 09 AntibioticsDocument77 pagesChapter 09 AntibioticsAngela Joy AmparadoNo ratings yet
- Pharmacotherapy of Diabetes MellitusDocument8 pagesPharmacotherapy of Diabetes MellitusSheryl Layne Lao-SebrioNo ratings yet
- Ursing Care of Client With CancerDocument51 pagesUrsing Care of Client With CancerJimmelyn PalosNo ratings yet
- Autonomic Nervous System: Parasympathetic and Sympathetic DivisionsDocument107 pagesAutonomic Nervous System: Parasympathetic and Sympathetic DivisionsMaria Mercedes LeivaNo ratings yet
- 1.introduction To PharmacologyDocument127 pages1.introduction To PharmacologyblacknurseNo ratings yet
- Anti InfectivesDocument126 pagesAnti Infectiveseunice lachicaNo ratings yet
- Introduction to Key Concepts in PharmacologyDocument30 pagesIntroduction to Key Concepts in PharmacologyCandy crush100% (1)
- Sexually Transmitted InfectionsDocument34 pagesSexually Transmitted InfectionsMariana Creciun100% (1)
- Pharmacology of Gastrointestinal SystemDocument4 pagesPharmacology of Gastrointestinal SystemZaira KimNo ratings yet
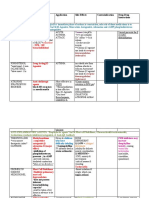
- Drug Name Mechanism Application Side Effects Contraindication Drug-Drug InteractionsDocument3 pagesDrug Name Mechanism Application Side Effects Contraindication Drug-Drug Interactionsazhar hussinNo ratings yet
- Gastrointestinal DrugsDocument2 pagesGastrointestinal DrugsJannah Mikhaela Alibay VillarinNo ratings yet
- NCM 106.2 3Document3 pagesNCM 106.2 3Marielle ChuaNo ratings yet
- Drug Study: Name Mechanism of Action Indication/Contraindication Side Effects Nursing ResponsibilityDocument2 pagesDrug Study: Name Mechanism of Action Indication/Contraindication Side Effects Nursing ResponsibilityJoshua DavantesNo ratings yet
- Huntington DiseaseDocument10 pagesHuntington Diseaseapi-498055661No ratings yet
- Albacio Eddiva Dapli-An Magwilang MaspilDocument138 pagesAlbacio Eddiva Dapli-An Magwilang MaspilJustineNo ratings yet
- Mental Health Nursing II NURS 2310: Unit 1 Basic Concepts of Mental Health and Mental IllnessDocument41 pagesMental Health Nursing II NURS 2310: Unit 1 Basic Concepts of Mental Health and Mental IllnessRocky Domingo LazaroNo ratings yet
- NotesDocument14 pagesNotesJan Rey L. TejereroNo ratings yet
- Autonomic Nervous System DrugsDocument111 pagesAutonomic Nervous System DrugsCres Padua QuinzonNo ratings yet
- Pharma ExamDocument7 pagesPharma ExamGeno Adrian T PampangaNo ratings yet
- Case HistoryDocument8 pagesCase HistoryjabeensarwarNo ratings yet
- Antiviral AgentsDocument14 pagesAntiviral AgentsKate MendozaNo ratings yet
- Pharmacology Section on Antibiotics, Antivirals and AntifungalsDocument5 pagesPharmacology Section on Antibiotics, Antivirals and AntifungalsPathalee ThalpavilaNo ratings yet
- Drugs Acting On Cardiovascular SystemDocument7 pagesDrugs Acting On Cardiovascular SystemAnwar Ul HaqueNo ratings yet
- TB in ChildrenDocument26 pagesTB in ChildrenReagan PatriarcaNo ratings yet
- Anti InflammatoryDocument41 pagesAnti InflammatoryKakai Ablanque LopozNo ratings yet
- Anti-TB Drugs: Mechanisms & Treatment PhasesDocument35 pagesAnti-TB Drugs: Mechanisms & Treatment PhasesZijieNo ratings yet
- Health Education PlanDocument10 pagesHealth Education PlanJulienne Sanchez-SalazarNo ratings yet
- Medical AbbreviationsDocument5 pagesMedical AbbreviationsReuelHengNo ratings yet
- Adult Nursing Immune FunctionDocument103 pagesAdult Nursing Immune FunctionEstherThompsonNo ratings yet
- Drugs Affecting The Gastrointestinal SystemDocument4 pagesDrugs Affecting The Gastrointestinal SystemJerica Jaz F. Vergara100% (1)
- TB TreatmentDocument58 pagesTB TreatmentNdayisaba CorneilleNo ratings yet
- Central Nervous System Pharmacology: Elly Nurus SakinahDocument64 pagesCentral Nervous System Pharmacology: Elly Nurus Sakinahkareem92No ratings yet
- Anti Emetics 141109072529 Conversion Gate02Document23 pagesAnti Emetics 141109072529 Conversion Gate02sanoozarmNo ratings yet
- Autonomic Nervous System: Skin / Gut Skeletal MuscleDocument7 pagesAutonomic Nervous System: Skin / Gut Skeletal MuscleAbby MataNo ratings yet
- USP Limit Test For LeadDocument2 pagesUSP Limit Test For LeadAbby MataNo ratings yet
- Sensations and Sensory Pathways General Senses Test Procedure Normal Result Abnormal Result Clinical InterpretationDocument5 pagesSensations and Sensory Pathways General Senses Test Procedure Normal Result Abnormal Result Clinical InterpretationAbby MataNo ratings yet
- Hypertension and Anti-Hypertensive DrugsDocument12 pagesHypertension and Anti-Hypertensive DrugsAbby Mata100% (1)
- Cholelithiasis AnaphysioDocument12 pagesCholelithiasis AnaphysioAbby MataNo ratings yet
- REDOXDocument27 pagesREDOXAbby MataNo ratings yet
- Carbohydrate identification testsDocument3 pagesCarbohydrate identification testsAbby Mata100% (1)
- Xanax Information-Sheet 2018-002Document2 pagesXanax Information-Sheet 2018-002Alexa HuffmanNo ratings yet
- Administering Subcutaneous InjectionDocument6 pagesAdministering Subcutaneous InjectionAnggrian Clara DewiNo ratings yet
- Analysis of NATCO Vs BAYER Pharma Case by Ankit SinghDocument18 pagesAnalysis of NATCO Vs BAYER Pharma Case by Ankit SinghAnkit Singh50% (4)
- Swcavilt 11103Document3 pagesSwcavilt 11103Sadik AmbaniNo ratings yet
- National Drug Policy 1995Document13 pagesNational Drug Policy 1995Madhu Sudhan PandeyaNo ratings yet
- Tylenol for mild to moderate painDocument2 pagesTylenol for mild to moderate painKristi WrayNo ratings yet
- Ch1 Intro To DrugsDocument23 pagesCh1 Intro To DrugsLalita SutcharitkulNo ratings yet
- Pharmaceutical Formulations III Pharm DQuestion BankDocument7 pagesPharmaceutical Formulations III Pharm DQuestion BankAnanda VijayasarathyNo ratings yet
- Formularium OBAT KlinikDocument13 pagesFormularium OBAT KlinikSathyani ParmitaNo ratings yet
- Abott LaboratoriesDocument41 pagesAbott Laboratoriesnishant_gupta_22No ratings yet
- Usp 2008 P 2 Supplement 3Document166 pagesUsp 2008 P 2 Supplement 3EstiPramestiningtyas100% (1)
- Asthma MedicationDocument6 pagesAsthma Medicationmomina arshidNo ratings yet
- Acyclovir antiviral drug overviewDocument3 pagesAcyclovir antiviral drug overviewLisaNo ratings yet
- LEAM ProtocolDocument6 pagesLEAM ProtocolShaza ElkourashyNo ratings yet
- Acetaminophen ToxicityDocument14 pagesAcetaminophen ToxicityEdel CarlosNo ratings yet
- Do Not CrushDocument16 pagesDo Not CrushDouglas Greg CookNo ratings yet
- Entire Pharm ClassDocument173 pagesEntire Pharm ClassnancyNo ratings yet
- Format Inject Stock Obat FOI 2017Document32 pagesFormat Inject Stock Obat FOI 2017Rani HadinataNo ratings yet
- 07 26 17Document24 pages07 26 17WoodsNo ratings yet
- Clinical PharmacyDocument38 pagesClinical PharmacyBalakrishna Thalamanchi100% (1)
- Omeprazole (Losec, Prilosec)Document1 pageOmeprazole (Losec, Prilosec)Jocelyn RiveraNo ratings yet
- PONV 30 Mar 2010 AmitDocument46 pagesPONV 30 Mar 2010 AmitAmit KochetaNo ratings yet
- What Are Drug Utilization Reviews (Dur) : Why Durs Are ImportantDocument3 pagesWhat Are Drug Utilization Reviews (Dur) : Why Durs Are ImportantthegroovyNo ratings yet
- Vesicular Palmoplantar EczemaDocument16 pagesVesicular Palmoplantar EczemakcipitNo ratings yet
- Normal Values HR RR BPDocument28 pagesNormal Values HR RR BPKthrine CrronNo ratings yet
- Report Regarding DepressionDocument18 pagesReport Regarding Depressiontech masterNo ratings yet
- Caffeine Piece in WiredDocument4 pagesCaffeine Piece in Wiredthird3planetNo ratings yet
- Drugs Acting On The Endocrine SystemDocument90 pagesDrugs Acting On The Endocrine SystemKATHERINE GRACE JOSENo ratings yet
- Antiepileptic DrugsDocument39 pagesAntiepileptic Drugsking_goldNo ratings yet
- Package InsertDocument2 pagesPackage InsertcherokeeNo ratings yet