You might also like
- Intervention and Reflection Basic Issues in Medical EthicsDocument816 pagesIntervention and Reflection Basic Issues in Medical EthicsAndrea Jenkins89% (9)
- John Mordechai Gottman, Lynn Fainsilber Katz, Carole Hooven - Meta-Emotion - How Families Communicate Emotionally-Routledge (1997) PDFDocument375 pagesJohn Mordechai Gottman, Lynn Fainsilber Katz, Carole Hooven - Meta-Emotion - How Families Communicate Emotionally-Routledge (1997) PDFRoxana Malan100% (1)
- Fine Motor Skills of Children With Down SyndromeDocument260 pagesFine Motor Skills of Children With Down SyndromeYurita Kamil100% (3)
- Garantisadong PambataDocument3 pagesGarantisadong Pambataboss062212No ratings yet
- The Doh Nutrition ProgramDocument10 pagesThe Doh Nutrition ProgramDianne MaeNo ratings yet
- National Nutrition PolicyDocument18 pagesNational Nutrition PolicyhealthsutraNo ratings yet
- Priority Nutrition Indicators For The Post-2015 Sustainable Development FrameworkDocument1 pagePriority Nutrition Indicators For The Post-2015 Sustainable Development FrameworkthousanddaysNo ratings yet
- Legal and Ethical Issues in Pediatric NursingDocument18 pagesLegal and Ethical Issues in Pediatric NursingTanvi100% (4)
- CHN Group 4 Reporting 1Document44 pagesCHN Group 4 Reporting 1RIK HAROLD GATPANDANNo ratings yet
- Ii. Problems and Development Strategies: Problems of The Third World CountriesDocument21 pagesIi. Problems and Development Strategies: Problems of The Third World CountriesMicsjadeCastilloNo ratings yet
- Malnutrition and IndiaDocument3 pagesMalnutrition and IndiaPrashant AndhaleNo ratings yet
- Exposé Anglais La MalnutritionDocument9 pagesExposé Anglais La MalnutritionSeydou CisseNo ratings yet
- BMJ h4173 FullDocument5 pagesBMJ h4173 FullRabisha AshrafNo ratings yet
- Garantisadong PambataDocument3 pagesGarantisadong PambataJieann Crissel PilapilNo ratings yet
- Social and Economic Impact of MalnutritionDocument4 pagesSocial and Economic Impact of MalnutritionAmanNo ratings yet
- Malnutrition Morris Adams MDocument31 pagesMalnutrition Morris Adams Mokwadha simionNo ratings yet
- Muliika Stephen Chapter 1 and 2Document21 pagesMuliika Stephen Chapter 1 and 2LiikascypherNo ratings yet
- Expanded Doh Programs: List of TopicsDocument8 pagesExpanded Doh Programs: List of TopicsCyrusNo ratings yet
- Creating Mass Movement To Address MalnutritionDocument17 pagesCreating Mass Movement To Address MalnutritionCHAITI CHAKRABORTYNo ratings yet
- 1000 Days Brief 508Document7 pages1000 Days Brief 508Reham LasheenNo ratings yet
- Office of The SecretaryDocument19 pagesOffice of The Secretarykiteli mendozaNo ratings yet
- Dm2020-0092 Interim Nutritional Guidelines For Women of Reproductive Age WRADocument9 pagesDm2020-0092 Interim Nutritional Guidelines For Women of Reproductive Age WRARiza Joy DABALOSNo ratings yet
- Importance of Early Nutrition and Health OutcomesDocument4 pagesImportance of Early Nutrition and Health OutcomesRobby NurhariansyahNo ratings yet
- Self Directive LearningDocument18 pagesSelf Directive Learningcrystal fate valdezNo ratings yet
- Ppan ReflectionDocument3 pagesPpan Reflectionanecita calamohoy100% (1)
- M - S N S 2014-2025 Technical Guidance Brief: Ulti Ectoral Utrition TrategyDocument7 pagesM - S N S 2014-2025 Technical Guidance Brief: Ulti Ectoral Utrition TrategyIsaac MangulenjeNo ratings yet
- Ppan 2023Document3 pagesPpan 2023rogelio ramiroNo ratings yet
- BREASTFEEDINGDocument28 pagesBREASTFEEDINGFiona Xandra San JuanNo ratings yet
- Philippine Nutrition Plan Targets Reducing Stunting, WastingDocument7 pagesPhilippine Nutrition Plan Targets Reducing Stunting, WastingJerreca DasasNo ratings yet
- Child Health Strategic Plan 2001-2004Document5 pagesChild Health Strategic Plan 2001-2004Piao Liang JingNo ratings yet
- Strategy: Roadmap For Nutrition in South Africa 2013-2017Document50 pagesStrategy: Roadmap For Nutrition in South Africa 2013-2017Laura Lopez GonzalezNo ratings yet
- Literature ReviewDocument3 pagesLiterature ReviewImbroglio ProductionsNo ratings yet
- Overview & Community Pediatrics: DefinitionDocument3 pagesOverview & Community Pediatrics: DefinitionJessica Febrina WuisanNo ratings yet
- NUTRITION ESSENTIALS A Guide For Health ManagersDocument148 pagesNUTRITION ESSENTIALS A Guide For Health ManagersMatias CANo ratings yet
- Bangladesh PDFDocument10 pagesBangladesh PDFDamesa MiesaNo ratings yet
- Public Health Nutrition InterventionDocument9 pagesPublic Health Nutrition Interventionpdsth7mtsjNo ratings yet
- ORDINANCE TEMPLATE - First 1000 DaysDocument15 pagesORDINANCE TEMPLATE - First 1000 DaysGiezlRamos-PolcaNo ratings yet
- Infant and Young Child FeedingDocument5 pagesInfant and Young Child FeedingRinjaya TeguhNo ratings yet
- Why Does Malnutrition Increases in Sri LankaDocument6 pagesWhy Does Malnutrition Increases in Sri Lankarovel shelieNo ratings yet
- Rajiv Gandhi University of Health Sciences Bangalore, KarnatakaDocument27 pagesRajiv Gandhi University of Health Sciences Bangalore, Karnatakasathyasai999No ratings yet
- Review On CHNDocument8 pagesReview On CHNAnnalisa TellesNo ratings yet
- تغذية الاطفالDocument20 pagesتغذية الاطفالJamal JunaidNo ratings yet
- Book Chapter National Nutritional PolicyDocument15 pagesBook Chapter National Nutritional Policyscience worldNo ratings yet
- Nutrition and India GS1Document2 pagesNutrition and India GS1Mat MohanNo ratings yet
- Linking Nutrition and HealthDocument24 pagesLinking Nutrition and HealththousanddaysNo ratings yet
- Save The Children Child Survival - Position Paper 2009Document7 pagesSave The Children Child Survival - Position Paper 2009nileshsingh29062092No ratings yet
- Hunger Alleviation & Nutrition Landscape AnalysisDocument82 pagesHunger Alleviation & Nutrition Landscape AnalysisthousanddaysNo ratings yet
- RMNCH+A: Improving Maternal and Child Health in IndiaDocument42 pagesRMNCH+A: Improving Maternal and Child Health in Indiashivangi sharma100% (1)
- New Hope For Malnourished Mothers and ChildrenDocument12 pagesNew Hope For Malnourished Mothers and ChildrenthousanddaysNo ratings yet
- Maternal AbhaDocument13 pagesMaternal AbhaAnju RaniNo ratings yet
- Reflection Paper: Community Strategies/Interventions On Health and NutritionDocument1 pageReflection Paper: Community Strategies/Interventions On Health and NutritionChristina CorcinoNo ratings yet
- Provision of Child Health Care 2010Document50 pagesProvision of Child Health Care 2010Nour AhmededNo ratings yet
- Programmes Related To Child Health and WelfareDocument40 pagesProgrammes Related To Child Health and WelfareAleena ShibuNo ratings yet
- Untitled DocumentDocument3 pagesUntitled DocumentKhenyuza Angel ClementeNo ratings yet
- Nutrition Problems & Solutions in IndiaDocument39 pagesNutrition Problems & Solutions in IndiaBeulah DasariNo ratings yet
- Epidemiological Aspects of Maternal and Child Health and Its Issues Word ContentDocument40 pagesEpidemiological Aspects of Maternal and Child Health and Its Issues Word ContentNimi Simon100% (2)
- Primary SourcesDocument2 pagesPrimary SourcesRenaiah Kamaong QuitorianoNo ratings yet
- IPNAP Position Paper Updated 01 Mar 2011Document18 pagesIPNAP Position Paper Updated 01 Mar 2011Stephanie PeNo ratings yet
- Health System in LDCsDocument19 pagesHealth System in LDCsAyneh MaqpoonNo ratings yet
- The epidemiological transition: incorporating obesity prevention into nutrition programmesDocument8 pagesThe epidemiological transition: incorporating obesity prevention into nutrition programmesrc513No ratings yet
- W6 - Nutrition Program, Oral Health Program, Essential Health Packages For The Adolescent, and Older PersonsDocument4 pagesW6 - Nutrition Program, Oral Health Program, Essential Health Packages For The Adolescent, and Older PersonsApostol DyNo ratings yet
- Global Commitments Address Nutrition TransitionDocument11 pagesGlobal Commitments Address Nutrition Transitionmaurisio viemmoNo ratings yet
- Childhood Obesity: Causes and Consequences, Prevention and Management.From EverandChildhood Obesity: Causes and Consequences, Prevention and Management.No ratings yet
- Healthy Schools, Healthy Lives: A Teacher's Guide to Tackling Childhood ObesityFrom EverandHealthy Schools, Healthy Lives: A Teacher's Guide to Tackling Childhood ObesityNo ratings yet
- RA 11222 - Administrative Adoption - Group 17 PDFDocument24 pagesRA 11222 - Administrative Adoption - Group 17 PDFPatricia Nicole BalgoaNo ratings yet
- 5,6,7 CmcaDocument224 pages5,6,7 CmcaErika CadawanNo ratings yet
- REVIEW OF RELATED LITERATURE (Grade 12 English Thesis)Document3 pagesREVIEW OF RELATED LITERATURE (Grade 12 English Thesis)Dae Young SeoNo ratings yet
- Expanded Programme For Free Maternity: Package BenefitsDocument2 pagesExpanded Programme For Free Maternity: Package BenefitsQuentene odongoNo ratings yet
- Causes and Effects of Teen PregnancyDocument5 pagesCauses and Effects of Teen PregnancyRae Simone SampangNo ratings yet
- Midterm Exam Review: Gender Roles and StereotypesDocument5 pagesMidterm Exam Review: Gender Roles and StereotypesMickaella Amor De VeraNo ratings yet
- Millennials Can't Handle Critical FeedbackDocument12 pagesMillennials Can't Handle Critical FeedbackLhea Joy T. CiprianoNo ratings yet
- PSY201 Study Guide S3 2020Document177 pagesPSY201 Study Guide S3 2020fazila.hares90No ratings yet
- EDUC50 Part 3Document4 pagesEDUC50 Part 3Cas LoydeNo ratings yet
- Mother's Day Gift Tags - TomKat StudioDocument1 pageMother's Day Gift Tags - TomKat StudioThe TomKat Studio100% (1)
- Moderate Anemia in Pregnant WomenDocument4 pagesModerate Anemia in Pregnant Womensiti rahayuNo ratings yet
- Uncertainties of LifeDocument1 pageUncertainties of LifeeaglefrgNo ratings yet
- Task2 Educ.2Document5 pagesTask2 Educ.2HONEYLYN CASINGNo ratings yet
- Pradhan Mantri Yojna Review - Dr. Sasmita BeheraDocument5 pagesPradhan Mantri Yojna Review - Dr. Sasmita BeheraSasmita BeheraNo ratings yet
- WVM Walkthrough V9.4Document15 pagesWVM Walkthrough V9.4Ryller X-XNo ratings yet
- My Family Is Very Inspiring To MeDocument2 pagesMy Family Is Very Inspiring To MeMidz Santayana100% (1)
- AnthropometricDocument11 pagesAnthropometricDots DyNo ratings yet
- Emergency DeliveryDocument61 pagesEmergency DeliveryRam Kirubakar ThangarajNo ratings yet
- The Effects of Different Parenting Styles of Students' Academic Performance in Online Class SettingDocument29 pagesThe Effects of Different Parenting Styles of Students' Academic Performance in Online Class SettingSnowNo ratings yet
- AssignmentDocument3 pagesAssignmentStephanie EspiridionNo ratings yet
- Men's Conference Speech FINALDocument11 pagesMen's Conference Speech FINALPaul ApredaNo ratings yet
- VocabularyDocument1 pageVocabularyGaluh SadhanaNo ratings yet
- Personal Responsibility Agreement: What Is TANF?Document1 pagePersonal Responsibility Agreement: What Is TANF?Shana LeighlaNo ratings yet
- Importance of FamilyDocument1 pageImportance of FamilyMOLLEY VARUGHESE A/P P.E. VARUGHESE MoeNo ratings yet
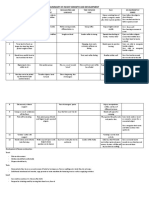
- SUMMARY OF INFANT GROWTH AND DEVELOPMENTDocument10 pagesSUMMARY OF INFANT GROWTH AND DEVELOPMENTDARLENE ROSE BONGCAWILNo ratings yet
- ABA Books Master ListDocument15 pagesABA Books Master Listعلم ينتفع بهNo ratings yet