You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- 9 AnsDocument25 pages9 AnsDrGasnasNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Peripheral NeuropathyDocument48 pagesPeripheral NeuropathyDrGasnasNo ratings yet
- Autonomic Nervous SystemDocument48 pagesAutonomic Nervous SystemDrGasnasNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- 12.4.09 Laudate Spinal LesionsDocument31 pages12.4.09 Laudate Spinal LesionsDrGasnasNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Lec. 2 - Autonomic Nervous SystemDocument26 pagesLec. 2 - Autonomic Nervous SystemDrGasnasNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- ch15 APR LectureDocument60 pagesch15 APR LectureDrGasnasNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Perspective of Synaptic Protection After Post-Infarction Treatment With StatinsDocument9 pagesPerspective of Synaptic Protection After Post-Infarction Treatment With StatinsDrGasnasNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- 4762376Document54 pages4762376DrGasnasNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Differentiating Upper From Lower Motor Neuron LesionsDocument4 pagesDifferentiating Upper From Lower Motor Neuron LesionsDrGasnasNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- What Imaging Teaches Us - КопияDocument62 pagesWhat Imaging Teaches Us - КопияDrGasnas100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Encephalitiscia3 151011085926 Lva1 App6892Document43 pagesEncephalitiscia3 151011085926 Lva1 App6892DrGasnasNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Nervous SystemDocument123 pagesNervous SystemDrGasnasNo ratings yet
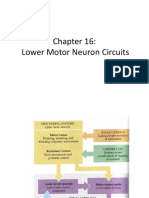
- Chapter 16 LizDocument58 pagesChapter 16 LizDrGasnasNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Alpha-Lipoic Acid Treatment Is Neurorestorative and Promotes Functional Recovery After Stroke in RatsDocument16 pagesAlpha-Lipoic Acid Treatment Is Neurorestorative and Promotes Functional Recovery After Stroke in RatsDrGasnasNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- WLK Chapter 006 NeurologicAssessDocument57 pagesWLK Chapter 006 NeurologicAssessDrGasnasNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- NIH Public Access: Author ManuscriptDocument18 pagesNIH Public Access: Author ManuscriptDrGasnasNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Role of GABA Plasticity in StrokeDocument3 pagesRole of GABA Plasticity in StrokeDrGasnasNo ratings yet
- Call For Papers: Neural Degeneration and Plasticity in Communication Disorders: Mechanism, Evaluation, and TreatmentDocument1 pageCall For Papers: Neural Degeneration and Plasticity in Communication Disorders: Mechanism, Evaluation, and TreatmentDrGasnasNo ratings yet
- Call For Papers: Plasticity of The Gabaergic System in Physiology and DiseaseDocument1 pageCall For Papers: Plasticity of The Gabaergic System in Physiology and DiseaseDrGasnasNo ratings yet
- Music Listening Enhances Cognitive Recovery and Mood After Middle Cerebral Artery StrokeDocument11 pagesMusic Listening Enhances Cognitive Recovery and Mood After Middle Cerebral Artery StrokeLAURIEJERIENo ratings yet
- Nervous SystemDocument123 pagesNervous SystemDrGasnasNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Fernandez-Torre ClinNeuroph12-Nonconvulsive SE Adults Electroclin DifferencesDocument8 pagesFernandez-Torre ClinNeuroph12-Nonconvulsive SE Adults Electroclin DifferencesDrGasnasNo ratings yet
- UnconsciousnessDocument91 pagesUnconsciousnessDrGasnasNo ratings yet
- In Ammatory Mechanisms in Ischemic Stroke PDFDocument11 pagesIn Ammatory Mechanisms in Ischemic Stroke PDFGustavo CabanasNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Call For Papers: Maladaptive Plasticity and Neuropathic PainDocument1 pageCall For Papers: Maladaptive Plasticity and Neuropathic PainDrGasnasNo ratings yet
- Central Nervous SystemDocument25 pagesCentral Nervous SystemDrGasnasNo ratings yet
- ReflexesDocument35 pagesReflexesBaleli Zagala100% (1)
- Nervous SystemDocument58 pagesNervous SystemDrGasnasNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Nervous System Powerpoint2007 - 1Document98 pagesNervous System Powerpoint2007 - 1DrGasnasNo ratings yet
- CNS PNSDocument163 pagesCNS PNSDrGasnasNo ratings yet
- Group 5Document19 pagesGroup 5Jazrine Dyllah Flores100% (2)
- Lotf Argument EssayDocument4 pagesLotf Argument Essayapi-332982124No ratings yet
- Introduction To Algorithm & Flowchart - L1Document20 pagesIntroduction To Algorithm & Flowchart - L1April VasquezNo ratings yet
- Managing ConflictDocument16 pagesManaging ConflictGwenNo ratings yet
- Looking at Aspects of A NovelDocument17 pagesLooking at Aspects of A NovelGus LionsNo ratings yet
- Lesson Plan PDFDocument7 pagesLesson Plan PDFtaneastefanita100% (1)
- Emotions LectureDocument12 pagesEmotions LecturePalwasha SheikhNo ratings yet
- Describe With Examples, The Three Inference Rules Involving QuantifiersDocument10 pagesDescribe With Examples, The Three Inference Rules Involving QuantifiersalbertspadeNo ratings yet
- Actual Freedom - Made EasyDocument186 pagesActual Freedom - Made EasyJustine100% (1)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- How Does Nature Nurture Creativity?Document20 pagesHow Does Nature Nurture Creativity?Anonymous vWJ2rNvPNo ratings yet
- Organizational SocializationDocument19 pagesOrganizational SocializationAhsan Khan NiaziNo ratings yet
- Chapter 2 MultigradeDocument3 pagesChapter 2 MultigradeLovely Mahinay CapulNo ratings yet
- Authentic LearningDocument52 pagesAuthentic Learningsmvuksie100% (1)
- RCOT Informed View - Sensory Integration Feb 2021Document2 pagesRCOT Informed View - Sensory Integration Feb 2021David NkwabiNo ratings yet
- William Labov and The Social Stratification of RDocument3 pagesWilliam Labov and The Social Stratification of RSamaraNo ratings yet
- Rynna's Week 13 TSL1044 Online Learning 2 Part 1Document2 pagesRynna's Week 13 TSL1044 Online Learning 2 Part 1Rynna NaaNo ratings yet
- ch3Document43 pagesch3Sudheer AyazNo ratings yet
- 2 Document Reality PDFDocument3 pages2 Document Reality PDFNicole TapiaNo ratings yet
- Lesson Plan 7 - Adverbs of FrequencyDocument4 pagesLesson Plan 7 - Adverbs of FrequencyMaribel Carvajal RiosNo ratings yet
- 9903463892NMHP Detail - 0 - 2Document19 pages9903463892NMHP Detail - 0 - 2Pratibha LoarNo ratings yet
- The Ultimate Texting GuideDocument86 pagesThe Ultimate Texting Guidewebotpad50% (2)
- Table of Score EquivalentDocument3 pagesTable of Score EquivalentCaroline Paratcha67% (3)
- The Forced-Choice Paradigm and The Perception of Facial Expressions of EmotionDocument11 pagesThe Forced-Choice Paradigm and The Perception of Facial Expressions of EmotionjnkjnNo ratings yet
- Why People Shouldn't Watch Too Much TelevisionDocument2 pagesWhy People Shouldn't Watch Too Much TelevisionDhriti Chowdary GallaNo ratings yet
- Horney, Karen - Self Analysis PDFDocument154 pagesHorney, Karen - Self Analysis PDFdamari67No ratings yet
- 2012 Kim Y. Development and Application of STEAM Teaching Model Based On The Rube Goldberg S InventionDocument6 pages2012 Kim Y. Development and Application of STEAM Teaching Model Based On The Rube Goldberg S InventionJose Gallardo ANo ratings yet
- Brown Et Al., 2020Document5 pagesBrown Et Al., 2020LauraNo ratings yet
- Oxford Happiness QuestionnaireDocument2 pagesOxford Happiness QuestionnaireSyed Wasi ShahNo ratings yet
- Case StudyDocument1 pageCase StudyKhyati MehtaNo ratings yet
- Unit 1Document152 pagesUnit 1Crazy DPS YTNo ratings yet
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (24)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)