You might also like
- The Peat WhispererDocument85 pagesThe Peat Whispererzarrin77100% (6)
- Lung Cancer Report Sample High enDocument1 pageLung Cancer Report Sample High enSiddhesh PawarNo ratings yet
- Internal Audit Ratings GuideDocument19 pagesInternal Audit Ratings Guidesanranist2100% (3)
- Smith Slides CH 4Document26 pagesSmith Slides CH 4USHA RANI SONOWALNo ratings yet
- AAFP Board Review ClinchersDocument53 pagesAAFP Board Review ClinchersJessica E Isom100% (2)
- 1cambrigton Dave Ielts Reading 100 9 PointsDocument43 pages1cambrigton Dave Ielts Reading 100 9 PointsWit FksunNo ratings yet
- Winter Safety Toolbox TalkDocument18 pagesWinter Safety Toolbox TalkKristina100% (1)
- PriceNEJMrev PrimaryDocument10 pagesPriceNEJMrev PrimarySunilSainiNo ratings yet
- What To Know About Eyebrow TransplantsDocument5 pagesWhat To Know About Eyebrow TransplantsOliver Carrasco VilladomaNo ratings yet
- Hairbiology: Growth and PigmentationDocument1 pageHairbiology: Growth and PigmentationроманNo ratings yet
- Hair Loss and Herbs For TreatmentDocument13 pagesHair Loss and Herbs For TreatmentmuhtevaNo ratings yet
- Hairrestoration Intheethnicpatient Andreviewofhair Transplant FundamentalsDocument8 pagesHairrestoration Intheethnicpatient Andreviewofhair Transplant FundamentalsGabriel Urrea BoteroNo ratings yet
- Female Pattern Hair LossDocument5 pagesFemale Pattern Hair LossDavid Fernando Rojas BayonaNo ratings yet
- Articlehu 77Document14 pagesArticlehu 77Matheus De oliveiraNo ratings yet
- Xu 2017Document13 pagesXu 2017Stella SunurNo ratings yet
- Xu2017 PDFDocument13 pagesXu2017 PDFalysa ahadyahNo ratings yet
- An Open Clinical Study To Evaluate Safety and Efficacy of Hairzone Solution in The Management of Diffuse Hair LossDocument4 pagesAn Open Clinical Study To Evaluate Safety and Efficacy of Hairzone Solution in The Management of Diffuse Hair LossShrinivas PrabhuNo ratings yet
- Hair Loss Research PapersDocument6 pagesHair Loss Research Papersgzrvpcvnd100% (1)
- Anzai 2020Document6 pagesAnzai 2020Belen Llanquilef NavarroNo ratings yet
- Treatment of Monilethrix With Oral Minoxidil: Ase ReportDocument4 pagesTreatment of Monilethrix With Oral Minoxidil: Ase ReportClzth TFMNo ratings yet
- Hair Loss and Herbs For Treatment Lourith2013Document13 pagesHair Loss and Herbs For Treatment Lourith2013leonardorodriguezsabateNo ratings yet
- An Approach To Patients With AlopeciaDocument12 pagesAn Approach To Patients With AlopeciaMariana de la VegaNo ratings yet
- Hair Cosmetics: An Overview: Eview ArticleDocument15 pagesHair Cosmetics: An Overview: Eview ArticleThao PhamNo ratings yet
- Latest Hair Loss RESEARCH and TECHNIQUE Breakthrough in 2012Document8 pagesLatest Hair Loss RESEARCH and TECHNIQUE Breakthrough in 2012Dr Andrew KimNo ratings yet
- Eyebrow and Eyelash Alopecia A Clinical ReviewDocument13 pagesEyebrow and Eyelash Alopecia A Clinical ReviewAndreiaEscudeiroNo ratings yet
- Hair Care Promising Herbs: A Review: K. Rashid, V. Baskar Ananda Raj, P. S Shiji Kumar, K.M NishadDocument12 pagesHair Care Promising Herbs: A Review: K. Rashid, V. Baskar Ananda Raj, P. S Shiji Kumar, K.M NishaddeaducxNo ratings yet
- Reading Part A Hair LossDocument6 pagesReading Part A Hair Lossfernanda1rondelliNo ratings yet
- Low-Dose Oral Minoxidil in The Treatment of Alopecia - Evidence and Experience-Based Consensus Statement of Indian Experts - PMCDocument12 pagesLow-Dose Oral Minoxidil in The Treatment of Alopecia - Evidence and Experience-Based Consensus Statement of Indian Experts - PMCAbhinav ChawlaNo ratings yet
- Techniques and Applications of Hair Transplantation in Hair DiseasesDocument25 pagesTechniques and Applications of Hair Transplantation in Hair DiseasesMudassar SattarNo ratings yet
- Physical Means of Treating Unwanted Hair: R W & T S. ADocument10 pagesPhysical Means of Treating Unwanted Hair: R W & T S. Adipika awindaNo ratings yet
- Female Pattern Baldness - Diagnosis and TreatmentsDocument3 pagesFemale Pattern Baldness - Diagnosis and TreatmentsKadeer AlamNo ratings yet
- Microneedling en Alopecia Androgenética Comparando Dos Profundidades Diferentes de MicroagujasDocument7 pagesMicroneedling en Alopecia Androgenética Comparando Dos Profundidades Diferentes de MicroagujasLuisa BucioNo ratings yet
- AlopeciaDocument11 pagesAlopeciaAnonymous kltUTa100% (1)
- Alopecia AreataDocument8 pagesAlopecia AreataPedro López CastroNo ratings yet
- 13 Hair Boosting Remedies 2Document35 pages13 Hair Boosting Remedies 2Anonymous 2P5vzcSoDNo ratings yet
- HAIRLOSSDocument16 pagesHAIRLOSSIrawan Pandu Buditomo100% (1)
- Valproate-Induced Hair Loss - What To Tell Patients - MDedge PsychiatryDocument3 pagesValproate-Induced Hair Loss - What To Tell Patients - MDedge Psychiatrydo leeNo ratings yet
- Hair Transplantation: With Follicular Unit MicrograftsDocument2 pagesHair Transplantation: With Follicular Unit MicrograftsRavvaNo ratings yet
- Utilizing Dermal Papilla Cells For Hair and Skin GrowthDocument18 pagesUtilizing Dermal Papilla Cells For Hair and Skin Growthquinntai97No ratings yet
- Comprehensive Overview and Treatment Update On Hair LossDocument9 pagesComprehensive Overview and Treatment Update On Hair LossZuldan KaramiNo ratings yet
- Cataracts Pathophysiology and Managements: Abdulrahman Zaid AlshamraniDocument4 pagesCataracts Pathophysiology and Managements: Abdulrahman Zaid AlshamraniOcha24 TupamahuNo ratings yet
- EyelashDocument3 pagesEyelashMuhammad ZairulfikriNo ratings yet
- KukitDocument9 pagesKukitFarhan RahmadiNo ratings yet
- Minoxidil Mechanisms of Action On Hair Growthj.1365-2133.2004.05785.x PDFDocument9 pagesMinoxidil Mechanisms of Action On Hair Growthj.1365-2133.2004.05785.x PDFJames WuNo ratings yet
- Everything Ocu Lop Last I A Make e Up PermanentDocument8 pagesEverything Ocu Lop Last I A Make e Up PermanentDaritza C. MoyanoNo ratings yet
- Alopecia Androgenetica 2009Document9 pagesAlopecia Androgenetica 2009Franklin ArandaNo ratings yet
- Thesis Dry EyeDocument7 pagesThesis Dry Eyebsfp46eh100% (2)
- Promising Therapies For Treating And/or Preventing Androgenic AlopeciaDocument8 pagesPromising Therapies For Treating And/or Preventing Androgenic AlopeciabayuaulNo ratings yet
- Benefits of Scalp and Hair Treatment SLKDocument24 pagesBenefits of Scalp and Hair Treatment SLKRica VillaNo ratings yet
- Cooley 2013Document7 pagesCooley 2013rahulNo ratings yet
- Traction Alopecia February 2019 - Lay Reviewed February 2019Document5 pagesTraction Alopecia February 2019 - Lay Reviewed February 2019Asia GobourneNo ratings yet
- Alopecia: Mrs. Neeraja Rajiv Asst Professor Cardio-RespDocument52 pagesAlopecia: Mrs. Neeraja Rajiv Asst Professor Cardio-RespNEERAJA O S O S100% (1)
- Hair Research PaperDocument7 pagesHair Research Paperc9hpjcb3100% (1)
- First Intro Video PDFDocument10 pagesFirst Intro Video PDFmohamedNo ratings yet
- This Awareness of Multivitamin Hair Growth Uses and Benefit of Shampoo and Hair Ampule in Saudi AdultsDocument18 pagesThis Awareness of Multivitamin Hair Growth Uses and Benefit of Shampoo and Hair Ampule in Saudi AdultsIJAR JOURNALNo ratings yet
- The Experimental Study Effects of Coconut Milk and Egg White As A Pack To Enhance The Hair Health Among Adult Male and Female VolunteersDocument4 pagesThe Experimental Study Effects of Coconut Milk and Egg White As A Pack To Enhance The Hair Health Among Adult Male and Female VolunteersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Patient Education: Alopecia Areata (Beyond The Basics) - UpToDateDocument9 pagesPatient Education: Alopecia Areata (Beyond The Basics) - UpToDateAngga Julyananda PradanaNo ratings yet
- Mol S Poveda - Et - Al 2019 Pediatric - DermatologyDocument2 pagesMol S Poveda - Et - Al 2019 Pediatric - DermatologyMaria TebiesNo ratings yet
- Hair Loss In Women: The Ultimate Hair Loss Book For Every WomanFrom EverandHair Loss In Women: The Ultimate Hair Loss Book For Every WomanNo ratings yet
- 12 Harish K-Rajesh R-Yasar-Arafath A-Ramzan-Beevi MDocument15 pages12 Harish K-Rajesh R-Yasar-Arafath A-Ramzan-Beevi MMichaelNo ratings yet
- Lice and Scabies: Treatment UpdateDocument11 pagesLice and Scabies: Treatment UpdateYar ZepolNo ratings yet
- Research 10Document11 pagesResearch 10Nandini SeetharamanNo ratings yet
- Hair and Scalp Evaluation: The Trichogram: Practical DermatologyDocument10 pagesHair and Scalp Evaluation: The Trichogram: Practical DermatologyFelipe NunesNo ratings yet
- Article Kératines VitroDocument5 pagesArticle Kératines VitroTHIBAUTNo ratings yet
- Alpha-Gf GFC Study International Journal of Research in DermatologyDocument10 pagesAlpha-Gf GFC Study International Journal of Research in DermatologyraoNo ratings yet
- Ivocular HetcamDocument10 pagesIvocular HetcamIndra syahputraNo ratings yet
- IJCPR, Vol 2, Issue 4, Article 3Document10 pagesIJCPR, Vol 2, Issue 4, Article 3Indra syahputraNo ratings yet
- DMDM H MSDSDocument5 pagesDMDM H MSDSIndra syahputraNo ratings yet
- BeakersDocument1 pageBeakersIndra syahputraNo ratings yet
- Gastritis 22 Sep 14Document25 pagesGastritis 22 Sep 14Indra syahputraNo ratings yet
- Sme Guide v4 OnlineDocument24 pagesSme Guide v4 OnlineIndra syahputraNo ratings yet
- A Review of The Range of Effects of Niacinamide in Human SkinDocument6 pagesA Review of The Range of Effects of Niacinamide in Human SkinpicorikiNo ratings yet
- White Pepper (Piper Nigrurn, Linn.) To Commercial: Comparison of Antioxidant Activity of Extract From Seeds ofDocument9 pagesWhite Pepper (Piper Nigrurn, Linn.) To Commercial: Comparison of Antioxidant Activity of Extract From Seeds ofIndra syahputraNo ratings yet
- P 09 S 222Document6 pagesP 09 S 222Indra syahputraNo ratings yet
- The Cardiac GlycosidesDocument22 pagesThe Cardiac GlycosidesIndra syahputraNo ratings yet
- Evaluation of The Health Beneficial Properties of The Aromatic Ether Myristicin, A Volatile Oil Derived From Various Plants SourcesDocument17 pagesEvaluation of The Health Beneficial Properties of The Aromatic Ether Myristicin, A Volatile Oil Derived From Various Plants SourcesIndra syahputraNo ratings yet
- Caesalpinia SappanDocument5 pagesCaesalpinia SappanIndra syahputraNo ratings yet
- Terpenes Glycosides2Document33 pagesTerpenes Glycosides2Indra syahputraNo ratings yet
- TCM ChineseDocument11 pagesTCM ChineseIndra syahputraNo ratings yet
- WC 500166364Document22 pagesWC 500166364Indra syahputraNo ratings yet
- IJASVM 52026b3b5e5d3Document8 pagesIJASVM 52026b3b5e5d3Indra syahputraNo ratings yet
- Cardiac GlycosidesDocument8 pagesCardiac GlycosidesIndra syahputraNo ratings yet
- Gatuline RC-GB 1Document12 pagesGatuline RC-GB 1Indra syahputraNo ratings yet
- Dandelion Extract MSDSDocument3 pagesDandelion Extract MSDSIndra syahputraNo ratings yet
- C SappanDocument10 pagesC SappanIndra syahputraNo ratings yet
- C SappanDocument8 pagesC SappanIndra syahputraNo ratings yet
- C. SappanDocument4 pagesC. SappanIndra syahputraNo ratings yet
- Product ListDocument1 pageProduct ListIndra syahputraNo ratings yet
- Jia Libro 80pgDocument80 pagesJia Libro 80pgocoxodoNo ratings yet
- Latisse PiDocument12 pagesLatisse PiIndra syahputraNo ratings yet
- Cardiac GlycosidesDocument8 pagesCardiac GlycosidesIndra syahputraNo ratings yet
- Arc ErrorDocument77 pagesArc ErrorIndra syahputraNo ratings yet
- Simulation PDFDocument14 pagesSimulation PDFdanaionelaiulianNo ratings yet
- Bioactivities of PegagaDocument13 pagesBioactivities of PegagaKhalizatul KasimNo ratings yet
- Hemodynamic MonitoringDocument35 pagesHemodynamic MonitoringWiz SamNo ratings yet
- AIA IHS Clinics With TCM - Generic (120613)Document43 pagesAIA IHS Clinics With TCM - Generic (120613)junkaiiiNo ratings yet
- Chevron Thailand Employee and Contractor Handbook EngDocument200 pagesChevron Thailand Employee and Contractor Handbook EngAndré Lima100% (1)
- Jonsen 4 Box MethodDocument5 pagesJonsen 4 Box MethodsawsanNo ratings yet
- Comparison of Intraocular Pressure After Water Drinking Test in Primary Open Angle Glaucoma Patients Controlled With Latanoprost and TrabeculectomyDocument7 pagesComparison of Intraocular Pressure After Water Drinking Test in Primary Open Angle Glaucoma Patients Controlled With Latanoprost and TrabeculectomyDimas Djiwa DNo ratings yet
- Pengembangan Model Kepribadian Konselor Efektif Berbasis Budaya Siri' Na PesseDocument9 pagesPengembangan Model Kepribadian Konselor Efektif Berbasis Budaya Siri' Na PesseTjatur SurantullohNo ratings yet
- Johnson ReportDocument10 pagesJohnson ReportHarihar SharmaNo ratings yet
- Sagar SinghDocument4 pagesSagar SinghzombieNo ratings yet
- Hyoscine ButylbromideDocument2 pagesHyoscine ButylbromideKenneth ColeNo ratings yet
- The Daily Tar Heel For April 12, 2016Document8 pagesThe Daily Tar Heel For April 12, 2016The Daily Tar HeelNo ratings yet
- BioassayDocument38 pagesBioassayMuhammad Masoom AkhtarNo ratings yet
- Suplemento 1Document56 pagesSuplemento 1Dessirhe LaraNo ratings yet
- Aliza Updated ResumeDocument2 pagesAliza Updated Resumeapi-359939852No ratings yet
- Chapter 01Document22 pagesChapter 01kita5437100% (1)
- Liver Vascular Anatomy - A RefresherDocument10 pagesLiver Vascular Anatomy - A Refresherilham nugrohoNo ratings yet
- Grade 7 Health ModuleDocument22 pagesGrade 7 Health ModuleMeann Joy Barrios Mendoza100% (1)
- YMCA Program Guide - 2016Document44 pagesYMCA Program Guide - 2016Pickens County YMCANo ratings yet
- A Chance To Save Millions of Lives by Freeing Up Drug Patents - Advanced PDFDocument5 pagesA Chance To Save Millions of Lives by Freeing Up Drug Patents - Advanced PDFhahahapsuNo ratings yet
- Muhanga District Development Plan 2013-2018-1 01Document116 pagesMuhanga District Development Plan 2013-2018-1 01Joseph Tuseku Officiel100% (1)
- Assignment: Name: Qolbu Adi Wicaksono NIM: 19109011014Document3 pagesAssignment: Name: Qolbu Adi Wicaksono NIM: 19109011014Hafshah AgustinaNo ratings yet
- The Emergence of India's Pharmaceutical IndustryDocument41 pagesThe Emergence of India's Pharmaceutical Industryvivekgupta2jNo ratings yet
- Hizon Interview Group 2Document3 pagesHizon Interview Group 2Dan HizonNo ratings yet
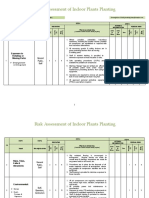
- Risk Assessment of Indoor Plants PlantingDocument5 pagesRisk Assessment of Indoor Plants Plantingطارق رضوانNo ratings yet