You might also like
- A Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Parathyroid Adenoma, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Frostbite and HypothermiaDocument43 pagesFrostbite and HypothermiaBlade DarkmanNo ratings yet
- Cold Injury and HypothermiaDocument31 pagesCold Injury and HypothermiatparamesparanNo ratings yet
- Acute TonsillitisDocument34 pagesAcute TonsillitisArvindhan100% (1)
- Infective Endocarditis CaseDocument3 pagesInfective Endocarditis CaseMershen GaniaNo ratings yet
- DB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaDocument5 pagesDB31 - Pathophysiology of Diabetes Mellitus and HypoglycemiaNeil Alcazaren かわいいNo ratings yet
- Myocardial InfarctionDocument25 pagesMyocardial Infarctionfam111222No ratings yet
- Manuscript Case Report Addison's Disease Due To Tuberculosis FinalDocument22 pagesManuscript Case Report Addison's Disease Due To Tuberculosis FinalElisabeth PermatasariNo ratings yet
- HHNK and DkaDocument4 pagesHHNK and Dkagoya100% (1)
- PurpuraDocument7 pagesPurpuraMarie Joe AbainzaNo ratings yet
- ThrombocytopeniaDocument2 pagesThrombocytopeniaNeoMedica100% (1)
- Stroke and Cerebrovascular DiseaseDocument14 pagesStroke and Cerebrovascular DiseaseMarwan M.No ratings yet
- Hyporeninemic HypoaldosteronismDocument12 pagesHyporeninemic HypoaldosteronismCésar Augusto Sánchez SolisNo ratings yet
- Perioperative HypothermiaDocument4 pagesPerioperative Hypothermiasri utari masyitahNo ratings yet
- Hepatic EncephalopathyDocument3 pagesHepatic EncephalopathyAnonymous GIGXKjfLNo ratings yet
- Cyclophosphamide For Injection, USPDocument2 pagesCyclophosphamide For Injection, USPemilia candraNo ratings yet
- Drug Classification - PhenytoinDocument3 pagesDrug Classification - Phenytoinkedwards108No ratings yet
- Hypertensive Cardiovascular DiseaseDocument5 pagesHypertensive Cardiovascular DiseaseAna Katrina OcanaNo ratings yet
- HemophiliaDocument4 pagesHemophiliaMechelle ChenNo ratings yet
- Anemia of Chronic Disease - Inflammation - UpToDateDocument36 pagesAnemia of Chronic Disease - Inflammation - UpToDateDomenica MurilloNo ratings yet
- DRUG STUDY FINAL (Onco) PDFDocument14 pagesDRUG STUDY FINAL (Onco) PDFFrancis Anthony LoslosoNo ratings yet
- A Subdural HematomaDocument12 pagesA Subdural HematomaGina Irene IshakNo ratings yet
- Guada A. Dumapit RN, ManDocument18 pagesGuada A. Dumapit RN, ManAnne B. BuenvenidaNo ratings yet
- Rosalina Q. de Sagun, M.D. Maria Antonia Aurora Moral - Valencia, M.DDocument52 pagesRosalina Q. de Sagun, M.D. Maria Antonia Aurora Moral - Valencia, M.DDaphne Jo ValmonteNo ratings yet
- City of Manila (Formerly City College of Manila) Mehan Gardens, ManilaDocument8 pagesCity of Manila (Formerly City College of Manila) Mehan Gardens, Manilaicecreamcone_201No ratings yet
- Clonidine Hydro ChlorideDocument4 pagesClonidine Hydro Chlorideapi-3797941100% (1)
- Coronary Artery DiseaseDocument3 pagesCoronary Artery Diseasetrew_wertNo ratings yet
- Case Study Worksheet EndocarditisDocument6 pagesCase Study Worksheet EndocarditisSharlee StoneNo ratings yet
- Case Presentation (Final)Document35 pagesCase Presentation (Final)Denie BoyonasNo ratings yet
- Concept Map Meningitis TheoryDocument3 pagesConcept Map Meningitis TheoryMia AuliaNo ratings yet
- PT EducationDocument4 pagesPT Educationapi-248017509No ratings yet
- Concept MapDocument9 pagesConcept MapAllene PaderangaNo ratings yet
- Case PresentationDocument6 pagesCase PresentationYrrem UbaganNo ratings yet
- Anatomy and Phsyiology of MeningococcemiaDocument2 pagesAnatomy and Phsyiology of MeningococcemiaKevin Comahig100% (1)
- HyponatremiaDocument6 pagesHyponatremiaJaymart Saclolo CostillasNo ratings yet
- Rheumatic Heart DiseaseDocument13 pagesRheumatic Heart Diseasedy15No ratings yet
- Pathophysiology of Congestive Heart Failure NarrativeDocument4 pagesPathophysiology of Congestive Heart Failure NarrativeAlfred BucabucaNo ratings yet
- Alzheimer Dementia: Starting, Stopping Drug Therapy: ReviewDocument6 pagesAlzheimer Dementia: Starting, Stopping Drug Therapy: ReviewAnonymous ZUaUz1wwNo ratings yet
- Liver CirrhosisDocument60 pagesLiver CirrhosisCamilla Zharine P. BantaNo ratings yet
- Minggu 5 LP THALASSEMIADocument14 pagesMinggu 5 LP THALASSEMIAMuhammad PanduNo ratings yet
- Nursing Care of Stroke - NewDocument4 pagesNursing Care of Stroke - Newninda saputriNo ratings yet
- NCP 1Document3 pagesNCP 1kat2111993No ratings yet
- Monro KellieDocument6 pagesMonro Kellievirz23No ratings yet
- Generic Name:: Drug Name Indicatio N Mechanism of Action Side Effects Nursing ResponsibilitiesDocument1 pageGeneric Name:: Drug Name Indicatio N Mechanism of Action Side Effects Nursing Responsibilitiesgrace pitogoNo ratings yet
- 403 Full PDFDocument10 pages403 Full PDFKuroto YoshikiNo ratings yet
- BSN4D-SG2 DM Type2Document201 pagesBSN4D-SG2 DM Type2Charisse CaydanNo ratings yet
- Case Stydy Angina PectorisDocument46 pagesCase Stydy Angina PectorissharenNo ratings yet
- Introduction - MIDocument10 pagesIntroduction - MIkhimiiiNo ratings yet
- Jade R. Dinolan BSN-4: Diagnosi SDocument5 pagesJade R. Dinolan BSN-4: Diagnosi SJhade Relleta100% (1)
- Addison's Disease (Primary Adrenal Insufficiency)Document5 pagesAddison's Disease (Primary Adrenal Insufficiency)sunnnydayNo ratings yet
- Danger Signs of PregnancyDocument3 pagesDanger Signs of PregnancyNesly Khyrozz LorenzoNo ratings yet
- Study Guide 1 - Leadership and FollowershipDocument11 pagesStudy Guide 1 - Leadership and FollowershipMark Vincent GallenoNo ratings yet
- Idiopathic Thrombocytopenic PurpuraDocument8 pagesIdiopathic Thrombocytopenic PurpuraMonette Abalos MendovaNo ratings yet
- Head InjuryDocument2 pagesHead InjuryPheiyi WongNo ratings yet
- Anorexia NervosaDocument11 pagesAnorexia NervosaSashMalikNo ratings yet
- Nursing Care Plan: Mission-Vision: Care Using Knowledge and CompassionDocument3 pagesNursing Care Plan: Mission-Vision: Care Using Knowledge and CompassionBen Jeremy del MarNo ratings yet
- Drug StudyDocument15 pagesDrug StudyMarc AnchetaNo ratings yet
- NCP-Case Presentation (CHF)Document4 pagesNCP-Case Presentation (CHF)Jessamine EnriquezNo ratings yet
- Cover SheetDocument32 pagesCover SheetRegina PerkinsNo ratings yet
- Wilkenson's Article On Defining AttributesDocument6 pagesWilkenson's Article On Defining AttributesRegina Perkins100% (1)
- Substance Differences: BetweenDocument5 pagesSubstance Differences: BetweenRegina PerkinsNo ratings yet
- Writing A Literature ReviewDocument12 pagesWriting A Literature ReviewRegina PerkinsNo ratings yet
- Emotional Intelligence and Diversity Model (Gardenswartz, Cherbosque, Rowe, 2010)Document11 pagesEmotional Intelligence and Diversity Model (Gardenswartz, Cherbosque, Rowe, 2010)Regina PerkinsNo ratings yet
- Causes and Management of Stress at Work: S MichieDocument6 pagesCauses and Management of Stress at Work: S MichieRegina PerkinsNo ratings yet
- Cystic 1Document13 pagesCystic 1Regina PerkinsNo ratings yet
- Modern Architecture: Frank Lloyd WrightDocument7 pagesModern Architecture: Frank Lloyd WrightRegina PerkinsNo ratings yet
- Barbiturate Overdose and HypoventilationDocument9 pagesBarbiturate Overdose and HypoventilationRegina PerkinsNo ratings yet
- Disease of Lids and Lacrim Al Apparatus: The First Affiliated Hospital of Zhengzhou UniversityDocument46 pagesDisease of Lids and Lacrim Al Apparatus: The First Affiliated Hospital of Zhengzhou Universityapi-19916399No ratings yet
- Understand The Process and Experience of Dementia: Unit DEM 301Document23 pagesUnderstand The Process and Experience of Dementia: Unit DEM 301Mary0% (1)
- NYS OPWDD March 28th COVID-19 Protocol For Essential PersonnelDocument2 pagesNYS OPWDD March 28th COVID-19 Protocol For Essential PersonnelLaw&CrimeNo ratings yet
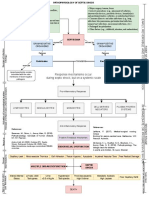
- Pathophysiology of Septic Shock Draft 1Document1 pagePathophysiology of Septic Shock Draft 1Ju Lie AnnNo ratings yet
- Laparoscopic Correction of Perforated Peptic Ulcer First Choice A Review of LiteratureDocument9 pagesLaparoscopic Correction of Perforated Peptic Ulcer First Choice A Review of LiteratureLe Hu ThaNo ratings yet
- MINDMAPDocument2 pagesMINDMAPrayzaoliveira.ausNo ratings yet
- Hypnoparenting Effects Towards Fatigue As An Impact of Chemotherapy Among Pediatric Patients With Acute Lymphoblastic LeukemiaDocument7 pagesHypnoparenting Effects Towards Fatigue As An Impact of Chemotherapy Among Pediatric Patients With Acute Lymphoblastic LeukemiaMuhammad HaezarNo ratings yet
- NCP ReviseDocument10 pagesNCP ReviseMaui TingNo ratings yet
- Digestive-System QADocument6 pagesDigestive-System QASageNo ratings yet
- Drug Studies For Muscular and Lymphatic SystemDocument6 pagesDrug Studies For Muscular and Lymphatic SystemLili M.No ratings yet
- Is A Mask Necessary in The Operating TheatreDocument3 pagesIs A Mask Necessary in The Operating TheatreGermano MatiasNo ratings yet
- Candida VulvovaginitisDocument20 pagesCandida VulvovaginitisVicobeingoNo ratings yet
- Client Information On Actinomycin-DDocument1 pageClient Information On Actinomycin-Dandru_s15No ratings yet
- Down Syndrome: Down Syndrome or Down's Syndrome, Also Known As Trisomy 21, Is ADocument3 pagesDown Syndrome: Down Syndrome or Down's Syndrome, Also Known As Trisomy 21, Is ASkill MasterNo ratings yet
- Drug Study (Schizo)Document5 pagesDrug Study (Schizo)aliannaNo ratings yet
- Presentation On Care of Critically Ill PatientDocument9 pagesPresentation On Care of Critically Ill Patientanamika sharmaNo ratings yet
- 10-Week Physical Activity Program For A Hypertensive Obese AdultDocument19 pages10-Week Physical Activity Program For A Hypertensive Obese AdultPhysiotherapist AliNo ratings yet
- Mas To Pa ThyDocument29 pagesMas To Pa ThyIng YingNo ratings yet
- Natural Herbs For Hidradenitis SuppurativaDocument2 pagesNatural Herbs For Hidradenitis SuppurativaJohn SmithNo ratings yet
- Medicine - BhanuDocument469 pagesMedicine - BhanuHIMAVARADHAN UNo ratings yet
- Backwell's 5 Min Veterinary ConsultDocument120 pagesBackwell's 5 Min Veterinary ConsultAndra Elena Pricop100% (2)
- WHO Report On Neglected Tropical DiseasesDocument184 pagesWHO Report On Neglected Tropical DiseasesN Aright ForestNo ratings yet
- Sexually Transmitted DiseasesDocument76 pagesSexually Transmitted Diseasessomaya abdulhakimNo ratings yet
- Skill Simple SchizophreniaDocument11 pagesSkill Simple SchizophreniasaidahrahmatNo ratings yet
- DinovoDocument1 pageDinovo17031 MD. IFTAKHAR HASSAN SAZALNo ratings yet
- Ictericia Neonatal: Guias NiceDocument54 pagesIctericia Neonatal: Guias NiceNat G. CuevasNo ratings yet
- 01 - 3【English】 (Sample) Prevaccination Screening QuestionnaireDocument1 page01 - 3【English】 (Sample) Prevaccination Screening QuestionnaireThet Ko WinNo ratings yet
- Jurnal InternasionalDocument110 pagesJurnal InternasionalRafi DevianaNo ratings yet
- Effect of Colonoscopy Screening On RisksDocument10 pagesEffect of Colonoscopy Screening On RisksAnderson SilvaNo ratings yet
- Mitral Valve SurgeryDocument2 pagesMitral Valve SurgeryLena MarieNo ratings yet