You might also like
- Dyspareunia in Women: Patient InformationDocument6 pagesDyspareunia in Women: Patient InformationIndra Putra WendiNo ratings yet
- Oman Law For Radioactive MaterialDocument6 pagesOman Law For Radioactive MaterialTabish Shaikh100% (1)
- Usp 797GCDocument61 pagesUsp 797GCAwni1989No ratings yet
- HTM0101PartC STERILIZER PDFDocument99 pagesHTM0101PartC STERILIZER PDFLuis CárdenasNo ratings yet
- Whythe10 ppmCriterionShouldBeAbandonedDocument5 pagesWhythe10 ppmCriterionShouldBeAbandonedMuhammad AsifNo ratings yet
- Applications Guide Barrier Iso La Tor 110805Document11 pagesApplications Guide Barrier Iso La Tor 110805snatarajanNo ratings yet
- Guidelines For Routine Environmental Cleaning of The Operating RoomDocument13 pagesGuidelines For Routine Environmental Cleaning of The Operating RoomYnaffit Alteza UntalNo ratings yet
- Health Base CriteriaDocument4 pagesHealth Base Criteriatimex59No ratings yet
- Ensuring The Air Suplly Rate To A Cleanroom Complies With The Eu GGMP and Iso 14644-3 Recovery Rate RequirementsDocument3 pagesEnsuring The Air Suplly Rate To A Cleanroom Complies With The Eu GGMP and Iso 14644-3 Recovery Rate RequirementsluisNo ratings yet
- 2.2.46. Chromatographic Separation Techniques PDFDocument5 pages2.2.46. Chromatographic Separation Techniques PDFAmar ElezovicNo ratings yet
- White Paper Fedegari - Decontamination by Hydrogen Peroxide Use and TechnicaldevelopmentsDocument3 pagesWhite Paper Fedegari - Decontamination by Hydrogen Peroxide Use and TechnicaldevelopmentsannunakipeNo ratings yet
- Continued Process VerificationDocument4 pagesContinued Process VerificationAbdul KalimNo ratings yet
- White Paper Hepa Versus Ulpa FiltersDocument6 pagesWhite Paper Hepa Versus Ulpa FiltersAakash PatelNo ratings yet
- Environmental Monitoring Risk AssessmentDocument22 pagesEnvironmental Monitoring Risk AssessmentMarcelo CarvalhoNo ratings yet
- HVAC Facility in Pharmaceutical Industry by Tomal GoshwamiDocument36 pagesHVAC Facility in Pharmaceutical Industry by Tomal GoshwamiMd. JewelNo ratings yet
- DCVMN Heat Sterilisation v3 1 PDFDocument94 pagesDCVMN Heat Sterilisation v3 1 PDFmuzammil21_adNo ratings yet
- 2002 07 08 - Airflow Management & Control in Pharmaceutical HVAC ApplicationsDocument12 pages2002 07 08 - Airflow Management & Control in Pharmaceutical HVAC ApplicationsHubert BonamisNo ratings yet
- Cyclotron Radionuclides FDG PDFDocument172 pagesCyclotron Radionuclides FDG PDFMark Denham100% (1)
- HEPA Filter Testing - IssuesDocument3 pagesHEPA Filter Testing - Issueszivko13No ratings yet
- Moist Heat SterilizatiojnDocument16 pagesMoist Heat Sterilizatiojnajitjoshi950No ratings yet
- One 2 One Cross Contamination FinalDocument9 pagesOne 2 One Cross Contamination FinalBlank BacktobasicNo ratings yet
- Containment EnclosuresDocument1 pageContainment EnclosuresAsif KhanNo ratings yet
- JMP 34 161Document6 pagesJMP 34 161Johnson CNo ratings yet
- WP Gmp-En AnshDocument12 pagesWP Gmp-En AnshFelix ShihNo ratings yet
- AdvaMed CAPA GuideDocument26 pagesAdvaMed CAPA GuideOmer ZiaNo ratings yet
- Cip TankDocument2 pagesCip TankAshwin ChanilNo ratings yet
- Smoke STUDIES ARTICLE 2 25 15 PDFDocument7 pagesSmoke STUDIES ARTICLE 2 25 15 PDFschumonNo ratings yet
- HVAC Rev1Document54 pagesHVAC Rev1Blank SermNo ratings yet
- Article2-Clean Operation Manufacturing294002107513883542Document4 pagesArticle2-Clean Operation Manufacturing294002107513883542авдей александрNo ratings yet
- Leseprobe FundamentalsDocument14 pagesLeseprobe FundamentalsDinesh SenathipathiNo ratings yet
- 2-5a MediaFillDocument37 pages2-5a MediaFillShobha RaniNo ratings yet
- Sterile Processing Monitoring ChecklistDocument3 pagesSterile Processing Monitoring ChecklistTianti PuadiNo ratings yet
- Mark PDFDocument42 pagesMark PDFdavincicode888No ratings yet
- Clean Rooms L Essentiel 3Document4 pagesClean Rooms L Essentiel 3Sweekar BorkarNo ratings yet
- Aada: Aao: Ade: Adme: Adi: Adr: Adrs: Agdufa: Ahu: Alcoa: Alcoa PlusDocument10 pagesAada: Aao: Ade: Adme: Adi: Adr: Adrs: Agdufa: Ahu: Alcoa: Alcoa PlusjhansiNo ratings yet
- Clean Room StandardsDocument12 pagesClean Room StandardslakshminarayananNo ratings yet
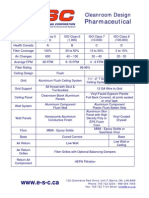
- Cleanroom Design Criteria PharmaceuticalDocument1 pageCleanroom Design Criteria PharmaceuticalNabil RamNo ratings yet
- WHO IVB 14.07 EngDocument14 pagesWHO IVB 14.07 EnggineNo ratings yet
- Bowie Dick Test Efhss Conf2006 Lecture17 enDocument42 pagesBowie Dick Test Efhss Conf2006 Lecture17 enPrakashKandaswamyNo ratings yet
- PLASMA and PLASMA PROTEINSDocument24 pagesPLASMA and PLASMA PROTEINSJude ChinecheremNo ratings yet
- Beximco Pharma MGT 210Document36 pagesBeximco Pharma MGT 210Romi SikderNo ratings yet
- Phuong - DryheatDocument5 pagesPhuong - DryheatqhpuongNo ratings yet
- Biological Evaluation of Medical Devices / Biosafety: Applicable ProductsDocument5 pagesBiological Evaluation of Medical Devices / Biosafety: Applicable ProductsAnonymous iqoU1mtNo ratings yet
- ParisonDocument12 pagesParisonJay KumarNo ratings yet
- Generation and Validation of Standard Operating Procedure For Dissolution ApparatusDocument18 pagesGeneration and Validation of Standard Operating Procedure For Dissolution ApparatusAbhishek JhaNo ratings yet
- SERVOTOUGH OxyExact 2200Document16 pagesSERVOTOUGH OxyExact 2200Karthik BNo ratings yet
- Procedure To Test The Efficacy of UV Lamp Against Microbial ChallengeDocument2 pagesProcedure To Test The Efficacy of UV Lamp Against Microbial ChallengevkNo ratings yet
- 2 Understanding Cleanroom Classification PDFDocument22 pages2 Understanding Cleanroom Classification PDFTECHNO DATENo ratings yet
- FDA Guide - Heart ValveDocument49 pagesFDA Guide - Heart ValveHector Barone100% (1)
- Hvac Solid (Who)Document75 pagesHvac Solid (Who)KundzoNo ratings yet
- Qualification of Shipping Containers: Supplement 13Document26 pagesQualification of Shipping Containers: Supplement 13TaNo ratings yet
- Schedule FDocument64 pagesSchedule FZeel DholakiaNo ratings yet
- ActiveCount Manual Rev.1.4Document30 pagesActiveCount Manual Rev.1.4Anonymous hISvHbfiB1100% (1)
- Validation NitrogenDocument4 pagesValidation NitrogenRohitsahuvapiNo ratings yet
- Quality Risk Management in Pharmaceutical Dispensing Center: M. Chitmetha, S. Prombanpong, and T. SomboonwiwatDocument8 pagesQuality Risk Management in Pharmaceutical Dispensing Center: M. Chitmetha, S. Prombanpong, and T. SomboonwiwatmmmmmNo ratings yet
- Vaisala On-Demand Webinar:: Listen To The Recording atDocument46 pagesVaisala On-Demand Webinar:: Listen To The Recording atMohammad IsmailNo ratings yet
- Cleaning Validation Approach 1Document19 pagesCleaning Validation Approach 1Dharmesh PatelNo ratings yet
- Stress Urinary Incontinence in Relation To Pelvic Floor Muscle StrengthDocument10 pagesStress Urinary Incontinence in Relation To Pelvic Floor Muscle StrengthNoraNo ratings yet
- Anaemia On First Trimester PregnancyDocument11 pagesAnaemia On First Trimester PregnancyNoraNo ratings yet
- Antenatal Care and Its Effect On Risk of PihDocument11 pagesAntenatal Care and Its Effect On Risk of PihNoraNo ratings yet
- Thyroid Hormonal Changes Among Women With Polycystic Ovarian SyndromeDocument14 pagesThyroid Hormonal Changes Among Women With Polycystic Ovarian SyndromeNoraNo ratings yet
- Pregnancy in A Patient With Recurrent GlioblastomaDocument6 pagesPregnancy in A Patient With Recurrent GlioblastomaNoraNo ratings yet
- Abdul Halim, Abu Sayeed Md. Abdullah, Fazlur Rahman, Animesh BiswasDocument11 pagesAbdul Halim, Abu Sayeed Md. Abdullah, Fazlur Rahman, Animesh BiswasNoraNo ratings yet
- Preterm DeliveryDocument12 pagesPreterm DeliveryNoraNo ratings yet
- Nursing ManagerDocument30 pagesNursing ManagerNoraNo ratings yet
- Female Circumcision: Limiting The Harm (Version 2 Peer Review: 2 Approved, 1 Approved With Reservations)Document8 pagesFemale Circumcision: Limiting The Harm (Version 2 Peer Review: 2 Approved, 1 Approved With Reservations)NoraNo ratings yet
- Active Management of Pregnant Cancer PatientDocument9 pagesActive Management of Pregnant Cancer PatientNoraNo ratings yet
- Injections SiteDocument10 pagesInjections SiteNora100% (2)
- Bakri Balloon PDFDocument5 pagesBakri Balloon PDFNoraNo ratings yet
- Menu Makanan Untuk Pesakit Hospital: IsninDocument2 pagesMenu Makanan Untuk Pesakit Hospital: IsninNoraNo ratings yet
- Orientation ListDocument1 pageOrientation ListNoraNo ratings yet
- End of Life Care BrochureDocument2 pagesEnd of Life Care BrochureNoraNo ratings yet
- Pressure Points - Postnatal Care Planning PDFDocument15 pagesPressure Points - Postnatal Care Planning PDFNoraNo ratings yet
- Kwawu Foster Kwesi - Breast Cancer, Knowledge, Attitudes and Perception Amongs Female Soldiers of The Ghana Armed Forces in The Greater Accra Region - 2009 PDFDocument93 pagesKwawu Foster Kwesi - Breast Cancer, Knowledge, Attitudes and Perception Amongs Female Soldiers of The Ghana Armed Forces in The Greater Accra Region - 2009 PDFNoraNo ratings yet
- Didik UPSR 2017 TARIKH 9.1.2017 - 1079367617 PDFDocument15 pagesDidik UPSR 2017 TARIKH 9.1.2017 - 1079367617 PDFPencil Box100% (2)
- A Randomized Trial of Coached Versus Uncoached Maternal Pushing During The Second Stage of Labor 2006 American Journal of Obstetrics and GynecologyDocument4 pagesA Randomized Trial of Coached Versus Uncoached Maternal Pushing During The Second Stage of Labor 2006 American Journal of Obstetrics and GynecologyNoraNo ratings yet
- BSSDocument4 pagesBSSNoraNo ratings yet
- Prenatal Care by Connie Sussan AustenDocument31 pagesPrenatal Care by Connie Sussan AustenNoraNo ratings yet
- The Effect of A Training Program During Pregnancy On The Attitude and Intention of NulliparousDocument8 pagesThe Effect of A Training Program During Pregnancy On The Attitude and Intention of NulliparousNoraNo ratings yet
- Active Labor Duration and Dilation Rates Among Low Risk Nulliparous Women With Spontaneous Labor Onset A Systematic Review 2010 Journal of MidwiferyDocument11 pagesActive Labor Duration and Dilation Rates Among Low Risk Nulliparous Women With Spontaneous Labor Onset A Systematic Review 2010 Journal of MidwiferyNoraNo ratings yet
- Vaccination in Pregnancy PDFDocument7 pagesVaccination in Pregnancy PDFNoraNo ratings yet