You might also like
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Epistaxis - Causes and ManagementDocument25 pagesEpistaxis - Causes and ManagementTabitha G100% (1)
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Presentation On Epistaxis in ChildrenDocument39 pagesPresentation On Epistaxis in ChildrenAdditi SatyalNo ratings yet
- EPISTAXISDocument25 pagesEPISTAXISSuprit Sn78% (9)
- Ent ExaminationDocument85 pagesEnt ExaminationDevi Yusfita100% (1)
- Taking History Exam in ENTDocument7 pagesTaking History Exam in ENTLumos NoxNo ratings yet
- History Taking and Physical Exam in ENTDocument75 pagesHistory Taking and Physical Exam in ENTSantosh hambardeNo ratings yet
- Deviated Nasal Septum: Ahmednagar Homoeopathic Medical College & Hospital AhmednagarDocument13 pagesDeviated Nasal Septum: Ahmednagar Homoeopathic Medical College & Hospital AhmednagarSuhas IngaleNo ratings yet
- Osce EarexamDocument2 pagesOsce EarexamminhaapNo ratings yet
- Antral WashDocument19 pagesAntral WashRavi Bhushan SinghNo ratings yet
- Spleen PercussionDocument13 pagesSpleen PercussionRatusweethella Intan Yudagrahania PuspitaNo ratings yet
- Ent InstrumentsDocument82 pagesEnt InstrumentsAsma sultanaNo ratings yet
- Ears, Nose and Throat Diseases: Prepared By: Hannelli BelingonDocument103 pagesEars, Nose and Throat Diseases: Prepared By: Hannelli BelingonPatricia Kamille I. PawidNo ratings yet
- Tracheostomy Procedure GuideDocument18 pagesTracheostomy Procedure GuideSudhanshu ShekharNo ratings yet
- Causes and Treatment of EpistaxisDocument40 pagesCauses and Treatment of EpistaxisSilar KhanNo ratings yet
- The Tonsils (Waldeyer's Ring) - Lingual - Pharyngeal - Palatine - Tubal - TeachMeAnatomyDocument4 pagesThe Tonsils (Waldeyer's Ring) - Lingual - Pharyngeal - Palatine - Tubal - TeachMeAnatomywachito ricoNo ratings yet
- Steroid in EntDocument113 pagesSteroid in Entdrazmy2006100% (1)
- Classifying and Treating Sinonasal TumorsDocument25 pagesClassifying and Treating Sinonasal TumorsMariam QaisNo ratings yet
- Epistaxis: "Bleeding From Inside The Nose"Document12 pagesEpistaxis: "Bleeding From Inside The Nose"Farrukh Mehmood100% (1)
- ENT History TakingDocument14 pagesENT History TakingST67% (3)
- HyphemaDocument19 pagesHyphemaLiyanti RinceNo ratings yet
- Appendicitis PPT 1Document30 pagesAppendicitis PPT 1Prashant Mishra100% (1)
- Nasal Obstruction and Headache Case ReportDocument31 pagesNasal Obstruction and Headache Case Reportgracy davidNo ratings yet
- Basic Physical Examination in ENTDocument44 pagesBasic Physical Examination in ENTKIWANUKA GEORGE100% (1)
- AneurysmDocument59 pagesAneurysmPriyaNo ratings yet
- CSF RhinorrhoeaDocument12 pagesCSF RhinorrhoeaSuprit Sn100% (5)
- Atrophic RhinitisDocument23 pagesAtrophic RhinitisdrtpkNo ratings yet
- Surgical CP ParotidDocument43 pagesSurgical CP ParotidValarmathiNo ratings yet
- PPIs Improve ENT Symptoms in GERD PatientsDocument5 pagesPPIs Improve ENT Symptoms in GERD PatientsHadia YaqubNo ratings yet
- OtosclerosisDocument44 pagesOtosclerosisSonal Sharma100% (1)
- EpistaxisDocument33 pagesEpistaxispaulyn ramosNo ratings yet
- Examination of An UlcerDocument2 pagesExamination of An UlcerHongMingNo ratings yet
- ENTDocument51 pagesENTBryan Paul Ramirez100% (1)
- Case Presentation: S. Suchitra 3 Year MBBS MVJ Medical College and Research HospitalDocument23 pagesCase Presentation: S. Suchitra 3 Year MBBS MVJ Medical College and Research Hospitalwarkhungam khumlo100% (1)
- Chronic Suppurative Otitis Media A Model Case Sheet by DrtbaluDocument2 pagesChronic Suppurative Otitis Media A Model Case Sheet by DrtbaluMaria Arifuddin0% (1)
- Name: Wong Wai Kheong Matrix No: BMS12081154Document13 pagesName: Wong Wai Kheong Matrix No: BMS12081154myolie wuNo ratings yet
- Otitis Media: Dr. YasserDocument64 pagesOtitis Media: Dr. YasserYasser GaberNo ratings yet
- Case Presentation: by Michael ArmstrongDocument21 pagesCase Presentation: by Michael ArmstrongWirawan Amirul BahriNo ratings yet
- Ear Infection Assessment and ManagementDocument8 pagesEar Infection Assessment and ManagementArt Christian Ramos100% (1)
- Functional Endoscopic Sinus Surgery (Fess) (3) JDocument20 pagesFunctional Endoscopic Sinus Surgery (Fess) (3) JJulianthy SuentoNo ratings yet
- Tricuspid Atresia VivekDocument66 pagesTricuspid Atresia Vivekmihalcea alin100% (1)
- Stridor in Children: By: Maj Vishal Gaurav Moderator: DR A SethiDocument33 pagesStridor in Children: By: Maj Vishal Gaurav Moderator: DR A SethiVishal GauravNo ratings yet
- Cholesteatoma Part 5 Congenital Cholesteatoma PDFDocument4 pagesCholesteatoma Part 5 Congenital Cholesteatoma PDFSuprit Sn100% (1)
- Fistula in AnoDocument3 pagesFistula in Anokhadzx80% (5)
- PneumothoraxDocument52 pagesPneumothoraxtrisna satrianaNo ratings yet
- Deviated Nasal SeptumDocument45 pagesDeviated Nasal Septumdrtpk100% (3)
- My Lecture NEMEC Temporal Bone CourseDocument37 pagesMy Lecture NEMEC Temporal Bone CourseAileen Delos Santos-GarciaNo ratings yet
- Case (Rhinitis Alergi) 2Document38 pagesCase (Rhinitis Alergi) 2christopherNo ratings yet
- EpistaxisDocument22 pagesEpistaxisDood100% (1)
- Difficulty in Speech After StrokeDocument6 pagesDifficulty in Speech After StrokeAJ RegaladoNo ratings yet
- Ear AssessmentDocument39 pagesEar AssessmentLyn MendeNo ratings yet
- Case Presentation Hepatitis A LuluDocument28 pagesCase Presentation Hepatitis A LuluBrenda KarinaNo ratings yet
- Atrial Septal DefectDocument3 pagesAtrial Septal Defectmu_crNo ratings yet
- PneumoniaDocument16 pagesPneumoniachrisshiroNo ratings yet
- (ENT-OPT-FRS) End-Posting Examination Questions (G3) - 20180208 - 160700Document23 pages(ENT-OPT-FRS) End-Posting Examination Questions (G3) - 20180208 - 160700Steph Stephanie100% (1)
- Ent MCQDocument52 pagesEnt MCQKhadar BashaNo ratings yet
- Nasogastric Tube InsertionDocument10 pagesNasogastric Tube InsertionPoh Thing LawNo ratings yet
- EPISTAXIS LectureDocument30 pagesEPISTAXIS LectureDhienWhieNo ratings yet
- Epistaxis: Ms. Shital BhutkarDocument37 pagesEpistaxis: Ms. Shital BhutkarSuhas IngaleNo ratings yet
- Physics Investigatory Project Class 12Document12 pagesPhysics Investigatory Project Class 12shivanginirai7No ratings yet
- A 1116Document15 pagesA 1116Rama S. SinghNo ratings yet
- Healthy Voice: by Dan VascDocument22 pagesHealthy Voice: by Dan VascscoutjohnyNo ratings yet
- Revised Provisional Selection List 30122022 1Document150 pagesRevised Provisional Selection List 30122022 1onlinetrash45No ratings yet
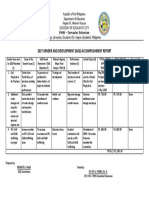
- GAD Accomplishment ReportDocument1 pageGAD Accomplishment ReportRenante Naga100% (6)
- Separation Processes Lecture 1 IntroductionDocument14 pagesSeparation Processes Lecture 1 Introductionabood assrfndyNo ratings yet
- Types of ProcurementDocument7 pagesTypes of ProcurementrahulNo ratings yet
- Computer Science ProjectDocument6 pagesComputer Science ProjectMohit KumarNo ratings yet
- Pearly Co Cleared Funds ForecastDocument8 pagesPearly Co Cleared Funds ForecastPutin Phy0% (1)
- General Psychology Mid Term ExamDocument2 pagesGeneral Psychology Mid Term Examapi-534780597No ratings yet
- 2 - FNCPDocument5 pages2 - FNCPIlda Lekka RequizaNo ratings yet
- IRC Girl Shine Part 4 DigitalDocument124 pagesIRC Girl Shine Part 4 DigitalMónica SalesNo ratings yet
- Ishrae 365 2009 PDFDocument16 pagesIshrae 365 2009 PDFZeeshan HasanNo ratings yet
- Hyundai forklift specification dimensionsDocument6 pagesHyundai forklift specification dimensionsАлександр ОлейникNo ratings yet
- 03 - 03 Product Index PDFDocument5 pages03 - 03 Product Index PDFWilder Fernando Vilca OreNo ratings yet
- MFT28 - Greg Plitt's 4-Week Military Fitness Trainer by MET-RxDocument7 pagesMFT28 - Greg Plitt's 4-Week Military Fitness Trainer by MET-RxRayNo ratings yet
- The Taste of Tradition: Submitted byDocument14 pagesThe Taste of Tradition: Submitted byvijay malikNo ratings yet
- Sakshijain75.Final ProDocument46 pagesSakshijain75.Final ProOm AherNo ratings yet
- Barlow 2Document56 pagesBarlow 2Lupu Adrian NicuNo ratings yet
- Ufara QasrinDocument14 pagesUfara Qasrinroni setiawanNo ratings yet
- FD2000 DatasheetDocument2 pagesFD2000 DatasheetIvan MihajlovicNo ratings yet
- ANPATH1 ReviewerDocument17 pagesANPATH1 ReviewerRashid DayaoNo ratings yet
- Indian Medical Tourism Industry: A Pathway For The Healthy Future of IndiaDocument13 pagesIndian Medical Tourism Industry: A Pathway For The Healthy Future of IndiaPranjal MaluNo ratings yet
- Winged Scapula Caused by Dorsal Scapular.21Document4 pagesWinged Scapula Caused by Dorsal Scapular.21emilio9fernandez9gatNo ratings yet
- Top 50 Most Delicious Taco Reci - Julie HatfieldDocument267 pagesTop 50 Most Delicious Taco Reci - Julie HatfieldMazhar Aslam100% (2)
- Candidates applied for Medical Officer post on contract basisDocument11 pagesCandidates applied for Medical Officer post on contract basiszephyrNo ratings yet
- Role of Drugs That Affect Renin Angiotensin SystemDocument22 pagesRole of Drugs That Affect Renin Angiotensin Systemash ashNo ratings yet
- Sea Level Rise Threatens Coastal CommunitiesDocument13 pagesSea Level Rise Threatens Coastal CommunitiesGunawan La OdeNo ratings yet
- Pharmaceutical Microbiology - B.pharmDocument383 pagesPharmaceutical Microbiology - B.pharmkeyurNo ratings yet
- PCS-9656 Arc ProtectionDocument3 pagesPCS-9656 Arc ProtectionganeshNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (20)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- Daniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisFrom EverandDaniel Kahneman's "Thinking Fast and Slow": A Macat AnalysisRating: 3.5 out of 5 stars3.5/5 (130)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Summary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: How to Be an Adult in Relationships: The Five Keys to Mindful Loving by David Richo: Key Takeaways, Summary & Analysis IncludedRating: 4 out of 5 stars4/5 (11)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)