You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5814)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- DCR Jumreirah Village - Tower Lots PDFDocument43 pagesDCR Jumreirah Village - Tower Lots PDFLino de jesus100% (1)
- Practical Ships Knowledge For CadetsDocument67 pagesPractical Ships Knowledge For CadetsHobbyLogic100% (2)
- Pub. 193 Skagerrak and Kattegat (Enroute), 14th Ed 2013Document169 pagesPub. 193 Skagerrak and Kattegat (Enroute), 14th Ed 2013cavris100% (1)
- Antidepressants AntidepressantsDocument38 pagesAntidepressants AntidepressantsjaneNo ratings yet
- Nautička Karta Dunava 12.2019 PDFDocument381 pagesNautička Karta Dunava 12.2019 PDFekozelj100% (2)
- Characteristics of A Drainage Basin & Management of Resources1.Ppt - 0Document45 pagesCharacteristics of A Drainage Basin & Management of Resources1.Ppt - 0AnuradhaKannan100% (1)
- India and GeopoliticsDocument15 pagesIndia and Geopoliticssatishq86% (7)
- Radiology Icm IiDocument8 pagesRadiology Icm IijaneNo ratings yet
- Medical Leadership Competency Framework: Landscape of HealthcareDocument15 pagesMedical Leadership Competency Framework: Landscape of HealthcarejaneNo ratings yet
- NIH Public Access: Delayed Antimicrobial Therapy Increases Mortality and Organ Dysfunction Duration in Pediatric SepsisDocument23 pagesNIH Public Access: Delayed Antimicrobial Therapy Increases Mortality and Organ Dysfunction Duration in Pediatric SepsisjaneNo ratings yet
- Mechanisms of Antibiotic Resistance in BacteriaDocument40 pagesMechanisms of Antibiotic Resistance in BacteriajaneNo ratings yet
- Intratympanic Membrane Congenital CholesteatomaDocument3 pagesIntratympanic Membrane Congenital CholesteatomajaneNo ratings yet
- By: Dr. Engelberta Sp. KJDocument14 pagesBy: Dr. Engelberta Sp. KJjaneNo ratings yet
- JawsDocument78 pagesJawsjaneNo ratings yet
- Substance Abuse Among Health Professionals: August 15, 2014Document25 pagesSubstance Abuse Among Health Professionals: August 15, 2014janeNo ratings yet
- Lymphokines & Cytokines: Immunology & DiseaseDocument34 pagesLymphokines & Cytokines: Immunology & DiseasejaneNo ratings yet
- Mechanisms of Antibiotic Resistance in BacteriaDocument41 pagesMechanisms of Antibiotic Resistance in BacteriajaneNo ratings yet
- To Physiology, Homeostasis, and Body Temperature: V. Sutarmo SetiadjiDocument20 pagesTo Physiology, Homeostasis, and Body Temperature: V. Sutarmo SetiadjijaneNo ratings yet
- Itching, Redness of The SkinDocument21 pagesItching, Redness of The SkinjaneNo ratings yet
- COMMUNICATION With Other ProfessionalsDocument12 pagesCOMMUNICATION With Other ProfessionalsjaneNo ratings yet
- LibraryDocument1 pageLibraryjaneNo ratings yet
- Transient Loss of Consciousness: History TakingDocument4 pagesTransient Loss of Consciousness: History TakingjaneNo ratings yet
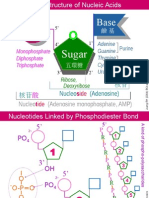
- NA01 StructureDocument5 pagesNA01 StructurejaneNo ratings yet
- STM Cels Lcture 1Document44 pagesSTM Cels Lcture 1janeNo ratings yet
- HandOUTS in HistoryDocument2 pagesHandOUTS in HistoryRyn CatNo ratings yet
- Adits Caves Karizi-Qanats and Tunnels in Afghanistan An Annotated BibliographytDocument87 pagesAdits Caves Karizi-Qanats and Tunnels in Afghanistan An Annotated Bibliographytkatgirl999No ratings yet
- Chapter 5: Compass TraversingDocument15 pagesChapter 5: Compass TraversingMausam JhaNo ratings yet
- Philippines and The Age of ExplorationDocument5 pagesPhilippines and The Age of ExplorationalalaLarusshhNo ratings yet
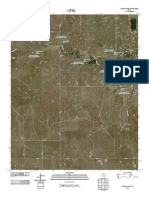
- Topographic Map of Young RanchDocument1 pageTopographic Map of Young RanchHistoricalMapsNo ratings yet
- Introduction of GeomaticDocument3 pagesIntroduction of GeomaticabdirahmanNo ratings yet
- AUEM4AsfZtarahan Mill List q1 2022 Ds IncomingDocument2 pagesAUEM4AsfZtarahan Mill List q1 2022 Ds IncomingWen WenNo ratings yet
- Central Business DistrictDocument2 pagesCentral Business DistrictSalzdgr8No ratings yet
- By: Yusuf Misbahuddin NPM: 115130113Document14 pagesBy: Yusuf Misbahuddin NPM: 115130113Yusuf MisbahuddinNo ratings yet
- Fiction vs. Non-Fiction Activity (Jane Yolen)Document3 pagesFiction vs. Non-Fiction Activity (Jane Yolen)Ryann LaBadNo ratings yet
- Head WorksDocument32 pagesHead WorksMuhammad FahadNo ratings yet
- Aranya Housing Case-StudyDocument16 pagesAranya Housing Case-StudyKshipra GajweNo ratings yet
- Sustainability Path Design GuidelinesDocument94 pagesSustainability Path Design GuidelinesMetro Los Angeles100% (1)
- ISSF 2016 05 Status of The Stocks Feb 2016Document94 pagesISSF 2016 05 Status of The Stocks Feb 2016awan syafrieNo ratings yet
- Eco 1Document19 pagesEco 1Shivanshu KhillanNo ratings yet
- Plane Table SurveyDocument4 pagesPlane Table SurveyAnonymous 0bI6BlNJLNo ratings yet
- Mining LegislationsDocument72 pagesMining LegislationsVinod Kumar SaoNo ratings yet
- Sulit: Bagi Setiap Soalan, Pilih Satu Jawapan Sahaja. Hitamkan Jawapan Kamu Pada Kertas Jawapan Objektif Yang DisediakanDocument14 pagesSulit: Bagi Setiap Soalan, Pilih Satu Jawapan Sahaja. Hitamkan Jawapan Kamu Pada Kertas Jawapan Objektif Yang DisediakanWong Chew NieNo ratings yet
- 02 MeasurementErrorsDocument22 pages02 MeasurementErrorsIrah Bonifacio100% (1)
- Contact List: Geographical Areas and GeomarketsDocument2 pagesContact List: Geographical Areas and GeomarketsHunterNo ratings yet
- YUANDocument15 pagesYUANYossi Chino BlancosNo ratings yet
- Permeability and SeepageDocument29 pagesPermeability and SeepageanmoltrueNo ratings yet
- Climate and Soil in The Netherlands IndiesDocument6 pagesClimate and Soil in The Netherlands IndiesScary CreaturesNo ratings yet
- Cryptobiotic Soil MythDocument7 pagesCryptobiotic Soil MythThe PetroglyphNo ratings yet