You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Domain Knowledge Healthcare Industry Part 1Document3 pagesDomain Knowledge Healthcare Industry Part 1Swathy SanthoshNo ratings yet
- January 2022Document64 pagesJanuary 2022Eric Santiago0% (1)
- Teaching Plan ProjectDocument2 pagesTeaching Plan Projectapi-295425485No ratings yet
- Critical Thinking ExerciseDocument5 pagesCritical Thinking Exerciseapi-295425485No ratings yet
- Therapeutic Nursing Intervention PaperDocument10 pagesTherapeutic Nursing Intervention Paperapi-295425485No ratings yet
- Advocacy LetterDocument7 pagesAdvocacy Letterapi-295425485No ratings yet
- Theory Application PaperDocument13 pagesTheory Application Paperapi-295425485No ratings yet
- Practice Summary PaperDocument11 pagesPractice Summary Paperapi-295425485No ratings yet
- Welcome To ChinaDocument10 pagesWelcome To Chinaapi-295425485No ratings yet
- Discharge Planning ChecklistDocument6 pagesDischarge Planning ChecklistadeliaNo ratings yet
- BSullivan Cost ReportDocument30 pagesBSullivan Cost ReportinforumdocsNo ratings yet
- Sagepoint Letter, May 6, 2020Document2 pagesSagepoint Letter, May 6, 2020WJZNo ratings yet
- Full Index of Fact Sheets - Final 495838 7Document232 pagesFull Index of Fact Sheets - Final 495838 7garbagepatchNo ratings yet
- Zambia Per Province As As at 1St December, 2019: Health Professions Council of ZambiaDocument18 pagesZambia Per Province As As at 1St December, 2019: Health Professions Council of ZambiaPerera KusalNo ratings yet
- GZ Modifier ChartDocument1 pageGZ Modifier ChartvidhunenNo ratings yet
- CARE ScriptDocument3 pagesCARE ScriptJay SteeleNo ratings yet
- DHHS Denial of St. Francis AppealDocument2 pagesDHHS Denial of St. Francis Appealstreiff at redstateNo ratings yet
- Analysis of Us Health Care PolicyDocument7 pagesAnalysis of Us Health Care Policyapi-520841770No ratings yet
- Discussion 5.3Document2 pagesDiscussion 5.3Sarah ParkinNo ratings yet
- EOB Code Crosswalk To HIPPA Standard CodesDocument1,665 pagesEOB Code Crosswalk To HIPPA Standard CodesVikas TomarNo ratings yet
- Bulletin: IHCP To Cover COVID-19 Vaccine Counseling As Part of EPSDT BenefitDocument2 pagesBulletin: IHCP To Cover COVID-19 Vaccine Counseling As Part of EPSDT BenefitIndiana Family to FamilyNo ratings yet
- Lecture 02 Part 1 Starting A Clinical Engineering DepartmentDocument31 pagesLecture 02 Part 1 Starting A Clinical Engineering DepartmentZahraa student2No ratings yet
- Traits of A Successful Nurse ManagerDocument2 pagesTraits of A Successful Nurse ManagerBethChay Lacson100% (1)
- Medicare'S Dmepos Competitive Bidding Program: HearingDocument151 pagesMedicare'S Dmepos Competitive Bidding Program: HearingScribd Government DocsNo ratings yet
- CustomerWiseStockSales KEPLERHEALTHCAREONYX 102023Document13 pagesCustomerWiseStockSales KEPLERHEALTHCAREONYX 102023Chinmay PatelNo ratings yet
- All Volunteers! Join Us For A Pizza Party in Your Honor!Document6 pagesAll Volunteers! Join Us For A Pizza Party in Your Honor!City of Mobile, AlabamaNo ratings yet
- Worksheets For Determaining Evacuation Capability PDFDocument5 pagesWorksheets For Determaining Evacuation Capability PDFoana_avramNo ratings yet
- Parkview Healthcare Inspection ReportDocument84 pagesParkview Healthcare Inspection ReportGreg DaileyNo ratings yet
- Amandaresume 1Document2 pagesAmandaresume 1api-510011907No ratings yet
- Nur 420 Policy Action Plan SubmissionDocument12 pagesNur 420 Policy Action Plan Submissionapi-625175559No ratings yet
- Qualified Small Employer Health Reimbursement Arrangement (QSEHRA) WorksheetDocument3 pagesQualified Small Employer Health Reimbursement Arrangement (QSEHRA) Worksheetmalak osmanNo ratings yet
- Donut Hole LetterDocument2 pagesDonut Hole LetterPeter SullivanNo ratings yet
- Missoula Care RehabDocument37 pagesMissoula Care RehabNBC MontanaNo ratings yet
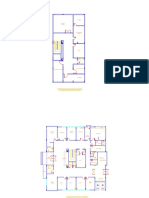
- Primary Healthcare Center DesignDocument4 pagesPrimary Healthcare Center DesignJihad Elias ChahlaNo ratings yet
- A Checklist For Incorporation of Video Visits (Telemedicine)Document2 pagesA Checklist For Incorporation of Video Visits (Telemedicine)Jeremy-ann HamNo ratings yet
- WellCare KY Medicaid InjectableInfusionFormDocument1 pageWellCare KY Medicaid InjectableInfusionFormKristichaNietyaNo ratings yet
- ACO Spotlight December 9 2020 Issue25Document7 pagesACO Spotlight December 9 2020 Issue25Nick BartzNo ratings yet