You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- 2021 Physician Compensation Report - Updated 0821Document24 pages2021 Physician Compensation Report - Updated 0821Michael Knapp100% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- LR 1350 Operating InstructionsDocument1,495 pagesLR 1350 Operating InstructionsPatrick Polujan100% (12)
- Significant Supreme Court RulingsDocument5 pagesSignificant Supreme Court Rulingsapi-307941674No ratings yet
- 2mw Biomass Gasification Gas Power Plant ProposalDocument9 pages2mw Biomass Gasification Gas Power Plant ProposalsabrahimaNo ratings yet
- Standard Into-Plane Fueling Service Levels and SafetyDocument8 pagesStandard Into-Plane Fueling Service Levels and SafetyPrekelNo ratings yet
- Antimatter and RocketsDocument7 pagesAntimatter and Rocketsdm23rdNo ratings yet
- Antimatter Power PiantsDocument3 pagesAntimatter Power Piantsdm23rdNo ratings yet
- Norman Augustine CEO Iockheed Martin Advisory Committee On The Future of The United States Space ProgramDocument11 pagesNorman Augustine CEO Iockheed Martin Advisory Committee On The Future of The United States Space Programdm23rdNo ratings yet
- Aipha Centauri: The Ciosest Star To EarthDocument4 pagesAipha Centauri: The Ciosest Star To Earthdm23rdNo ratings yet
- Ultraviolet LightDocument5 pagesUltraviolet Lightdm23rdNo ratings yet
- Space Junk/Debris: Sputnik US Vanguard 1 SatelliteDocument5 pagesSpace Junk/Debris: Sputnik US Vanguard 1 Satellitedm23rdNo ratings yet
- TITANDocument2 pagesTITANdm23rdNo ratings yet
- The Nazca Lines HomeworkDocument2 pagesThe Nazca Lines Homeworkdm23rdNo ratings yet
- Writting An EssayDocument5 pagesWritting An Essaydm23rdNo ratings yet
- Making An AbstractDocument3 pagesMaking An Abstractdm23rdNo ratings yet
- Angel's Story Part 1Document3 pagesAngel's Story Part 1dm23rdNo ratings yet
- The Nazca Lines HomeworkDocument2 pagesThe Nazca Lines Homeworkdm23rdNo ratings yet
- Two Cases of Chronic Tonsillitis Studied by FDG-PETDocument3 pagesTwo Cases of Chronic Tonsillitis Studied by FDG-PETdm23rdNo ratings yet
- Sample Doc File 100kbDocument13 pagesSample Doc File 100kbakshay mishraNo ratings yet
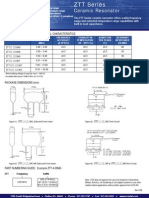
- Ceramic Resonator: Operating Conditions / Electrical CharacteristicsDocument1 pageCeramic Resonator: Operating Conditions / Electrical Characteristicsdm23rdNo ratings yet
- EULA For SyncToyDocument3 pagesEULA For SyncToyTotoPepeNo ratings yet
- WMP Firefox Plugin RelNotesDocument2 pagesWMP Firefox Plugin RelNotesyonielteduardNo ratings yet
- WMP EulaDocument3 pagesWMP EulaMatache GabrielaNo ratings yet
- Hidraulyc Pump LineDocument2 pagesHidraulyc Pump Linedm23rdNo ratings yet
- Two Cases of Chronic Tonsillitis Studied by FDG-PETDocument3 pagesTwo Cases of Chronic Tonsillitis Studied by FDG-PETdm23rdNo ratings yet
- At 89 C 52Document24 pagesAt 89 C 52Rohit MehtaNo ratings yet
- 8-Bit Microcontroller With 8K Bytes Flash AT89C52: FeaturesDocument23 pages8-Bit Microcontroller With 8K Bytes Flash AT89C52: FeaturesvbaixistaNo ratings yet
- Worksheet 2 - TLC - Updated Summer 2021Document4 pagesWorksheet 2 - TLC - Updated Summer 2021Bria PopeNo ratings yet
- Translating Child Development Research Into Practice - Can Teachers Foster Children's Theory of Mind in Primary SchoolDocument14 pagesTranslating Child Development Research Into Practice - Can Teachers Foster Children's Theory of Mind in Primary SchoolpecescdNo ratings yet
- Bandura Social Cognitive TheoryDocument93 pagesBandura Social Cognitive TheoryВикторияNo ratings yet
- 2.2 WaterDocument32 pages2.2 WaterHelena GlanvilleNo ratings yet
- Lem Cyclop Ewt Owner S Manual 10Document10 pagesLem Cyclop Ewt Owner S Manual 10josep_garcía_16No ratings yet
- What Is Aerobic Exercise?Document27 pagesWhat Is Aerobic Exercise?Zedy GullesNo ratings yet
- Clack 2983 WS1EE Twin Valve LDocument2 pagesClack 2983 WS1EE Twin Valve Lmohamed boufasNo ratings yet
- UAW-FCA Hourly Contract SummaryDocument20 pagesUAW-FCA Hourly Contract SummaryClickon DetroitNo ratings yet
- How To Make Panna CottaDocument3 pagesHow To Make Panna CottaBintNo ratings yet
- The Effect of Gas Metal Arc Welding (GMAW) Processes On Different Welding Parameters - DoneDocument5 pagesThe Effect of Gas Metal Arc Welding (GMAW) Processes On Different Welding Parameters - DoneAsim AliNo ratings yet
- FCE Writing 14 - ArticleDocument4 pagesFCE Writing 14 - Articlepingu70No ratings yet
- OSCE Pediatric Dentistry Lecture-AnswersDocument40 pagesOSCE Pediatric Dentistry Lecture-AnswersR MNo ratings yet
- Sikament®-4101 NS: Product Data SheetDocument2 pagesSikament®-4101 NS: Product Data SheetShihab AhamedNo ratings yet
- Performantele MTADocument5 pagesPerformantele MTAana aNo ratings yet
- 1 PBDocument16 pages1 PBRaffi GigiNo ratings yet
- 2014 EN AdvancedBootkitTechniquesOnAndroid ChenZhangqiShendiDocument66 pages2014 EN AdvancedBootkitTechniquesOnAndroid ChenZhangqiShendihombre pocilgaNo ratings yet
- Battle Healing PrayerDocument9 pagesBattle Healing PrayerSolavei LoanerNo ratings yet
- Neurology and Special Senses: High-Yield SystemsDocument72 pagesNeurology and Special Senses: High-Yield SystemsMahmoud Abu MayalehNo ratings yet
- Banaag Reflective Journal BlsDocument3 pagesBanaag Reflective Journal BlsR Hornilla ArcegaNo ratings yet
- PU-133AB - 規格GMXa spc 2022Document5 pagesPU-133AB - 規格GMXa spc 2022Ý TrầnNo ratings yet
- X FEDEX EIDocument13 pagesX FEDEX EINISREEN WAYANo ratings yet
- Corp Given To HemaDocument132 pagesCorp Given To HemaPaceNo ratings yet
- Test Unit 2 Urbanisation L P 12Document9 pagesTest Unit 2 Urbanisation L P 12Xuân NguyenNo ratings yet
- 2006 SM600Document2 pages2006 SM600Ioryogi KunNo ratings yet
- Genomics and Crop ImprovementDocument56 pagesGenomics and Crop Improvementsenguvelan100% (6)