You might also like
- SensoryProfile2 CaseStudy PDFDocument4 pagesSensoryProfile2 CaseStudy PDFEvelina LamsodieneNo ratings yet
- OT Services in Classroom PresentationDocument46 pagesOT Services in Classroom PresentationHusainiNo ratings yet
- Sensory Profile PowerpointDocument21 pagesSensory Profile PowerpointLama NammouraNo ratings yet
- Sensory Integration HandoutsDocument15 pagesSensory Integration HandoutsNAA NYC Metro Chapter86% (7)
- Sensory Integration - Information PacketDocument44 pagesSensory Integration - Information PacketConstanza Miranda Arriola100% (2)
- Sensory History QuestionnaireDocument6 pagesSensory History Questionnaireİpek OMUR100% (1)
- Basics TritoneDocument22 pagesBasics TritoneImani Balivaja100% (1)
- Short Sensory ProfileDocument11 pagesShort Sensory ProfileNurul Izzah Wahidul Azam100% (1)
- The Clinical Guide to Assessment and Treatment of Childhood Learning and Attention ProblemsFrom EverandThe Clinical Guide to Assessment and Treatment of Childhood Learning and Attention ProblemsNo ratings yet
- Fine Motor and Handwriting Skills ActivitiesDocument4 pagesFine Motor and Handwriting Skills Activitiesehopkins5_209No ratings yet
- GMFMscoresheetDocument6 pagesGMFMscoresheetAbdur RasyidNo ratings yet
- Apps For AutismDocument1 pageApps For Autismapi-407131623No ratings yet
- Beery Vmi Performance in Autism Spectrum DisorderDocument33 pagesBeery Vmi Performance in Autism Spectrum DisorderJayminertri Minorous100% (1)
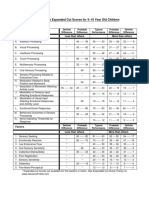
- Sensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenDocument1 pageSensory Profile Expanded Cut Scores For 3-10 Year Old ChildrenAyra MagpiliNo ratings yet
- Sensory Diet: Prepared by Christy E. Yee, OTRDocument12 pagesSensory Diet: Prepared by Christy E. Yee, OTRAlexandra StăncescuNo ratings yet
- Sensory Profile PowerpointDocument10 pagesSensory Profile PowerpointFedora Margarita Santander CeronNo ratings yet
- Occupational Therapy Screening Test: By: Occupational Therapy For Children & Learning Skills 4 KidsDocument9 pagesOccupational Therapy Screening Test: By: Occupational Therapy For Children & Learning Skills 4 KidsGa Bi33% (3)
- Allen Cogntive Disabilties ModelDocument29 pagesAllen Cogntive Disabilties ModelSarah Lyn White-Cantu100% (1)
- Sensory Profile: Submitted By-Amandeep Kaur M.O.T-Neuro, Sem 3 ENROLLMENT NO - A138141620004 Guided by - Ruby Ma'AmDocument42 pagesSensory Profile: Submitted By-Amandeep Kaur M.O.T-Neuro, Sem 3 ENROLLMENT NO - A138141620004 Guided by - Ruby Ma'Amamandeep kaurNo ratings yet
- Sensory Diet DocumentsDocument7 pagesSensory Diet Documentspratibhaumrariya100% (1)
- Occupational Therapy - Adolescence and Executive SkillsDocument3 pagesOccupational Therapy - Adolescence and Executive SkillsAnnbe BarteNo ratings yet
- Pediatric Treatment PlanDocument11 pagesPediatric Treatment PlanKayla Jensen100% (2)
- Examples of Occupational Therapy Goals For Sensory IntegrationDocument6 pagesExamples of Occupational Therapy Goals For Sensory IntegrationNaza AbdullahNo ratings yet
- SI Theory and PracticeDocument57 pagesSI Theory and PracticeMaria Laura Soria100% (2)
- Evidence Based Review of Interventions For Autism Used in or of Relevance To Occupational TherapyDocument14 pagesEvidence Based Review of Interventions For Autism Used in or of Relevance To Occupational Therapyapi-308033434No ratings yet
- Dyslexia BookletN PDFDocument33 pagesDyslexia BookletN PDFDr.V.Sivaprakasam100% (2)
- Milestone Chart For BabiesDocument8 pagesMilestone Chart For BabiesKaypee BorresNo ratings yet
- VMIpdfDocument6 pagesVMIpdfRidwan HadiputraNo ratings yet
- Witwer OT Developmental MilestonesDocument2 pagesWitwer OT Developmental Milestonespratibhaumrariya100% (3)
- How To Properly Use The Zapper and Magnetic PulserDocument7 pagesHow To Properly Use The Zapper and Magnetic PulserJiggaWhaaNo ratings yet
- Ot Goals NuevoDocument157 pagesOt Goals NuevoElbania PerezNo ratings yet
- SOS APPROACH Explanation For ParentsDocument5 pagesSOS APPROACH Explanation For ParentsAnn Villablanca100% (3)
- Knox Prescool PlayDocument7 pagesKnox Prescool Playkonna4539No ratings yet
- Handwriting Speed Assessment Pa TossDocument4 pagesHandwriting Speed Assessment Pa Tossdeni44450% (4)
- Rehabilitation of The Hand - HUNTER 005Document6 pagesRehabilitation of The Hand - HUNTER 005BeatrizIgelmo50% (4)
- Rehabilitation of The Hand - HUNTER 005Document6 pagesRehabilitation of The Hand - HUNTER 005BeatrizIgelmo50% (4)
- 10 Years PAt Dorsy PDFDocument32 pages10 Years PAt Dorsy PDFGurjeevNo ratings yet
- Learning Through PlayDocument2 pagesLearning Through PlayThe American Occupational Therapy Association100% (1)
- Contoh Ot ReportDocument10 pagesContoh Ot ReportHanum HamkaNo ratings yet
- Pediatric Occupational TherapyDocument13 pagesPediatric Occupational TherapyGeetha Priya Setty100% (3)
- Ota Watertown Si Clinical Assessment WorksheetDocument4 pagesOta Watertown Si Clinical Assessment WorksheetPaulina100% (1)
- The Parents Guide To Occupational Therap PDFDocument7 pagesThe Parents Guide To Occupational Therap PDFGabriela Lala0% (2)
- Tummy Time ToolsDocument6 pagesTummy Time ToolsflokaiserNo ratings yet
- Chapter 16: Application of Motor Control and Motor LearningDocument8 pagesChapter 16: Application of Motor Control and Motor LearningJireh Chambers100% (1)
- AutismMotorSkillEvaluationFINALBESt028.8 27 09Document6 pagesAutismMotorSkillEvaluationFINALBESt028.8 27 09Shayne Tee-MelegritoNo ratings yet
- Occupational Therapy Ia Sample ReportsDocument11 pagesOccupational Therapy Ia Sample Reportssneha duttaNo ratings yet
- Cerebral Palsy: Fauziah Rudhiati, M.Kep., Ns - Sp.Kep - AnDocument16 pagesCerebral Palsy: Fauziah Rudhiati, M.Kep., Ns - Sp.Kep - AnPopi NurmalasariNo ratings yet
- Dunn Sensory Profile InterpretationDocument5 pagesDunn Sensory Profile InterpretationScribdTranslationsNo ratings yet
- Azzam Scale in Practical Guide of Occupational TherapyFrom EverandAzzam Scale in Practical Guide of Occupational TherapyNo ratings yet
- CO OP AOTA - July - 2020Document10 pagesCO OP AOTA - July - 2020Ana Claudia GomesNo ratings yet
- Ot GuidelinesDocument107 pagesOt GuidelinesAhmed MaherNo ratings yet
- Chapter 8Document30 pagesChapter 8Karla CarazoNo ratings yet
- Pediatric Wheelchair Toolkit FINALDocument6 pagesPediatric Wheelchair Toolkit FINALIndiana Family to FamilyNo ratings yet
- Occupational Therapy - Play, SIs and BMTsDocument3 pagesOccupational Therapy - Play, SIs and BMTsAnnbe Barte100% (1)
- Handwriting and DyspraxiaDocument8 pagesHandwriting and DyspraxiaKirsty HayhoeNo ratings yet
- God's Pharmacy, Powerful POWER POINT PRESENTATIONDocument18 pagesGod's Pharmacy, Powerful POWER POINT PRESENTATIONpapa martin100% (1)
- OT Practice August 6 IssueDocument19 pagesOT Practice August 6 IssueThe American Occupational Therapy AssociationNo ratings yet
- Sfa Scool Function AssementDocument18 pagesSfa Scool Function AssementAnielle OliveiraNo ratings yet
- Sensory DietDocument4 pagesSensory Dietapi-571361183No ratings yet
- Early, Accurate Diagnosis and Early Intervention in Cerebral PalsyDocument11 pagesEarly, Accurate Diagnosis and Early Intervention in Cerebral PalsyRoberto López MataNo ratings yet
- AOTA Statement On Role of OT in NICUDocument9 pagesAOTA Statement On Role of OT in NICUMapi RuizNo ratings yet
- Ot Guidelines Child SpecificDocument34 pagesOt Guidelines Child Specific健康生活園Healthy Life Garden100% (1)
- Occupation Analysis in PracticeFrom EverandOccupation Analysis in PracticeLynette MackenzieNo ratings yet
- Sensory Diet Sample FormatDocument1 pageSensory Diet Sample FormatBernard CarpioNo ratings yet
- Article Play TherapyDocument19 pagesArticle Play TherapyBeatrizIgelmoNo ratings yet
- District Inset Proposal 2024Document6 pagesDistrict Inset Proposal 2024MANNY PAGADUAN83% (6)
- Medical Student Clinical Assessment Form: (Mm/dd/yy) (Mm/dd/yy)Document4 pagesMedical Student Clinical Assessment Form: (Mm/dd/yy) (Mm/dd/yy)Natasha Reddy0% (1)
- Tax On Corporation - NotesDocument9 pagesTax On Corporation - NotesMervidelleNo ratings yet
- College Accounting A Contemporary Approach 4th Edition Haddock Test BankDocument16 pagesCollege Accounting A Contemporary Approach 4th Edition Haddock Test Bankneymar94100% (6)
- 2020 Bar Exam Syllabus in Legal and Judicial EthicsDocument11 pages2020 Bar Exam Syllabus in Legal and Judicial EthicsMyBias KimSeokJinNo ratings yet
- Movement Difficulties in Developmental Disorders: Practical Guidelines for Assessment and ManagementFrom EverandMovement Difficulties in Developmental Disorders: Practical Guidelines for Assessment and ManagementNo ratings yet
- D Vocabulary Free Time ActivitiesDocument2 pagesD Vocabulary Free Time Activitiesguest4760% (5)
- Food & Drinks: Who Wants To Be The Top Banana in The Kitchen?Document34 pagesFood & Drinks: Who Wants To Be The Top Banana in The Kitchen?BeatrizIgelmoNo ratings yet
- Flightarrivals PDFDocument1 pageFlightarrivals PDFBeatrizIgelmoNo ratings yet
- Eatingoutexercises PDFDocument2 pagesEatingoutexercises PDFBeatrizIgelmoNo ratings yet
- 7th R.C. Chopra Memorial National Moot Court Competition2019 Pages 6 7 PDFDocument2 pages7th R.C. Chopra Memorial National Moot Court Competition2019 Pages 6 7 PDFSuhail KhanNo ratings yet
- Sterilization and Aseptic TechniqueDocument3 pagesSterilization and Aseptic TechniqueE.coilman100% (3)
- Infinitus Aka Marcus On MM LinesDocument2 pagesInfinitus Aka Marcus On MM LinesMilan CvetkovicNo ratings yet
- Bokashi As An Amendment and Source of Nitrogen in Sustainable Agricultural Systems: A ReviewDocument12 pagesBokashi As An Amendment and Source of Nitrogen in Sustainable Agricultural Systems: A ReviewDavid Andrés Vásquez StuardoNo ratings yet
- Sapna Project File PDFDocument57 pagesSapna Project File PDFPreet PreetNo ratings yet
- Spectrum TRD3 Tests EOT2 SpeakingDocument1 pageSpectrum TRD3 Tests EOT2 SpeakingTTNLittleGeniusNo ratings yet
- Darcy's Law BasicsDocument13 pagesDarcy's Law BasicsHarsh BhattNo ratings yet
- Mindfulness-Based Stress Reduction Improves Irritable Bowel Syndrome (IBS) Symptoms Via Specific Aspects of MindfulnessDocument10 pagesMindfulness-Based Stress Reduction Improves Irritable Bowel Syndrome (IBS) Symptoms Via Specific Aspects of MindfulnessN RNo ratings yet
- Forces and InclinesDocument16 pagesForces and InclinesCarlo Gimarino SalazarNo ratings yet
- Mba - Group 5 - Cooperative Strategy FinalDocument21 pagesMba - Group 5 - Cooperative Strategy FinalAwneeshNo ratings yet
- CognosyDocument11 pagesCognosyadia masooraNo ratings yet
- Bioavailability of Raw and Cooked EggsDocument7 pagesBioavailability of Raw and Cooked EggsVirtuosoXNo ratings yet
- Unit 2 FinalDocument58 pagesUnit 2 Finalshankar kmNo ratings yet
- Price Sally - Art Anthropology and Museums. Post Colonial Directions in The USADocument14 pagesPrice Sally - Art Anthropology and Museums. Post Colonial Directions in The USASantiago ZapataNo ratings yet
- Circuit Stewards Handbook 2021Document34 pagesCircuit Stewards Handbook 2021Qhayiya NjomeniNo ratings yet
- Altre Magie Per L5RDocument6 pagesAltre Magie Per L5RandromedafaustoNo ratings yet
- Basics of RF Electronics: Alessandro GalloDocument29 pagesBasics of RF Electronics: Alessandro GalloMONICA LOHNo ratings yet
- Mini Mental Parkinson Test Standardization and NorDocument4 pagesMini Mental Parkinson Test Standardization and NordianisvillarrealNo ratings yet
- Draft 4 Final Draft Language UsageDocument5 pagesDraft 4 Final Draft Language Usageapi-374432083No ratings yet
- Paper+26+ (2022 4 1) +Heirloom+Food+Preservation+Techniques+and+LanguagesDocument8 pagesPaper+26+ (2022 4 1) +Heirloom+Food+Preservation+Techniques+and+LanguagesHaruki AkemiNo ratings yet
- Stack Recursion Quick Sort WordDocument38 pagesStack Recursion Quick Sort WordrajNo ratings yet