You might also like
- Practical Transfusion Medicine for the Small Animal PractitionerFrom EverandPractical Transfusion Medicine for the Small Animal PractitionerNo ratings yet
- Hyperbaric MedDocument3 pagesHyperbaric MedJiggsNo ratings yet
- Nutrient Requirements of Domesticated RuminantsFrom EverandNutrient Requirements of Domesticated RuminantsNo ratings yet
- Cep07014 - Dispositivo de InfusãoDocument32 pagesCep07014 - Dispositivo de InfusãoEduardoNo ratings yet
- Baxter (Flo-Gard 6201) Volumetric Infusion Pump Flow Rate Accuracy - Test Design and Performance VerificationDocument21 pagesBaxter (Flo-Gard 6201) Volumetric Infusion Pump Flow Rate Accuracy - Test Design and Performance VerificationKousha TalebianNo ratings yet
- Journal of Carcinogenesis and Mutagenesis Research: Chemotherapy Pumps: Preparation and CounselingDocument5 pagesJournal of Carcinogenesis and Mutagenesis Research: Chemotherapy Pumps: Preparation and CounselingmochkurniawanNo ratings yet
- Enteral Feeding Devices With A Retention Balloon: Standard Test Methods ForDocument7 pagesEnteral Feeding Devices With A Retention Balloon: Standard Test Methods ForAhmad Zubair RasulyNo ratings yet
- Rigel Medical Guide To Infusion Pump Testing Us v1Document28 pagesRigel Medical Guide To Infusion Pump Testing Us v1catatanNo ratings yet
- Content ServerDocument10 pagesContent ServerCampbellhernanNo ratings yet
- Equipment For SurgeryDocument19 pagesEquipment For SurgerysanathNo ratings yet
- What Is Infusion Pump?Document6 pagesWhat Is Infusion Pump?Maria Alejandra Isaza suarezNo ratings yet
- Innovated overhead line for tube feedingsDocument78 pagesInnovated overhead line for tube feedingsMiNa SUy FullNo ratings yet
- Selecting A New Analyzer For The Hematology Laboratory:The Experience at Ohiohealth HospitalsDocument10 pagesSelecting A New Analyzer For The Hematology Laboratory:The Experience at Ohiohealth Hospitalspieterinpretoria391No ratings yet
- In-Use Stability Studies and Associated Labeling Statements For Multiple-Dose Injectable Animal Drug Products Guidance For IndustryDocument11 pagesIn-Use Stability Studies and Associated Labeling Statements For Multiple-Dose Injectable Animal Drug Products Guidance For IndustryVivi maifitrizaNo ratings yet
- AutomatedDocument17 pagesAutomatedapi-413377677No ratings yet
- BS_2143_Human_Recombinant_Insulin_finalDocument6 pagesBS_2143_Human_Recombinant_Insulin_finalGiang PhuonglyNo ratings yet
- Occupational English Test Oet Reading Part BC Test 04Document16 pagesOccupational English Test Oet Reading Part BC Test 04AndreaNo ratings yet
- Total Product Life Cycle: Infusion Pump - Premarket Notification (510 (K) ) Submissions DRAFT GUIDANCEDocument34 pagesTotal Product Life Cycle: Infusion Pump - Premarket Notification (510 (K) ) Submissions DRAFT GUIDANCEMatteo AgenoNo ratings yet
- Biostep AND Biostep Clinical Pro Semi-Recumbent Elliptical: IodexDocument48 pagesBiostep AND Biostep Clinical Pro Semi-Recumbent Elliptical: IodexvictorNo ratings yet
- Shelf Life Dating of Botanical Supplement Ingredients and ProductsDocument38 pagesShelf Life Dating of Botanical Supplement Ingredients and ProductsSandro ManchegoNo ratings yet
- Mcu Hospital - Filemon D. Tanchoco Foundation: Clinical Internship 2022 E-PortfolioDocument2 pagesMcu Hospital - Filemon D. Tanchoco Foundation: Clinical Internship 2022 E-PortfolioAngelica Joy GonzalesNo ratings yet
- Design and Material Optimization VentilatorDocument8 pagesDesign and Material Optimization VentilatorHadhi Hassan KhanNo ratings yet
- Draft Guidance On Tapentadol Hydrochloride IR TabletDocument1 pageDraft Guidance On Tapentadol Hydrochloride IR Tabletmjamil0995No ratings yet
- Acute Pancreatitis Part 3Document23 pagesAcute Pancreatitis Part 3Jerome CidNo ratings yet
- Infusion Pumps, Large-Volume - 040719081048Document59 pagesInfusion Pumps, Large-Volume - 040719081048Freddy Cruz BeltranNo ratings yet
- A High-Value, Low-Cost Bubble Continuous Positive Airway Pressure System For Low-Resource Settings: Technical Assessment and Initial Case ReportsDocument6 pagesA High-Value, Low-Cost Bubble Continuous Positive Airway Pressure System For Low-Resource Settings: Technical Assessment and Initial Case ReportsnshamapNo ratings yet
- Guia Contadores HematologicosDocument15 pagesGuia Contadores HematologicosSATURNONo ratings yet
- Positive Displacement PumpsDocument11 pagesPositive Displacement PumpsMohammed Al-AzawyNo ratings yet
- CDC Viral Transport Medium SOPDocument8 pagesCDC Viral Transport Medium SOPLyra Dennise LlidoNo ratings yet
- Aa AmericanDocument17 pagesAa AmericanJimmy LaboratoristaNo ratings yet
- Metered Dose Nasal SprayDocument10 pagesMetered Dose Nasal Sprayhaanh.truong229No ratings yet
- Guidance Industry Serving Sizes Foods That Can Reasonably Be Consumed One Eating OccasionDocument18 pagesGuidance Industry Serving Sizes Foods That Can Reasonably Be Consumed One Eating OccasionAlifah MauludinahNo ratings yet
- 1 s2.0 S2468067222001201 MainDocument11 pages1 s2.0 S2468067222001201 Mainvoronenok11No ratings yet
- Summer Training ON: Biomedical EquipmentsDocument20 pagesSummer Training ON: Biomedical EquipmentsAkansha HandaNo ratings yet
- 8introduction of Infusion SystemDocument6 pages8introduction of Infusion SystemGhulam MurtazaNo ratings yet
- Viral Transport MediumDocument8 pagesViral Transport MediumRajendran Dinesh KumarNo ratings yet
- WA DOHMedicalSurgeCatalogueDocument9 pagesWA DOHMedicalSurgeCataloguehaseebNo ratings yet
- Performance Improvement Team Worksheet (Focus-Pdca) Doc2Document4 pagesPerformance Improvement Team Worksheet (Focus-Pdca) Doc2api-283388869No ratings yet
- Disposable Infusion PumpsDocument20 pagesDisposable Infusion PumpsRaul SosaNo ratings yet
- Hospital CateringDocument15 pagesHospital CateringitzmeaneeshNo ratings yet
- Revised Joint Commission Standards for Medical EquipmentDocument6 pagesRevised Joint Commission Standards for Medical EquipmentVer Bautista0% (1)
- Matrixing: FPP To Be Marketed in The ProposedDocument4 pagesMatrixing: FPP To Be Marketed in The ProposedRachel HowardNo ratings yet
- Intersect ENT (XENT) Company PresentationDocument26 pagesIntersect ENT (XENT) Company PresentationmedtechyNo ratings yet
- College of Medicine and Health Science School of Pharmacy Hospital Pharmacy Practice ReportDocument10 pagesCollege of Medicine and Health Science School of Pharmacy Hospital Pharmacy Practice ReporthabtamuNo ratings yet
- Uji Potensi Antibiotik Turbidimetri USP 41Document8 pagesUji Potensi Antibiotik Turbidimetri USP 41nicholasNo ratings yet
- Jafar Zadeh 2016Document6 pagesJafar Zadeh 2016Bogdan FlorinNo ratings yet
- VSI Executive SummaryDocument9 pagesVSI Executive SummaryRyan MenorcaNo ratings yet
- WP Medical Device Endotoxin TestingDocument6 pagesWP Medical Device Endotoxin TestingJeevanend ArumugamNo ratings yet
- CDC Viral Transport Medium SOPDocument8 pagesCDC Viral Transport Medium SOPNurul PalesseiNo ratings yet
- Infusion Pumps: Desirable SpecificationsDocument7 pagesInfusion Pumps: Desirable SpecificationswgwsafNo ratings yet
- Lily Chu and David K Robinson: Industrial Choices For Protein Production by Large-Scale Cell CultureDocument8 pagesLily Chu and David K Robinson: Industrial Choices For Protein Production by Large-Scale Cell CultureCarina OliveiraNo ratings yet
- A Cleaning and Calibration Method For The Spiropro Portable Spirometer'S Pneumotachometer Tube in A Remote Field StudyDocument10 pagesA Cleaning and Calibration Method For The Spiropro Portable Spirometer'S Pneumotachometer Tube in A Remote Field StudyMihai PetrescuNo ratings yet
- Bair Hugger SWOT Analysis and Pricing StrategyDocument6 pagesBair Hugger SWOT Analysis and Pricing StrategyeasydataNo ratings yet
- Article On Heart ValvesDocument16 pagesArticle On Heart Valvesrohit860No ratings yet
- Effect of Bladder Volume On Measured Intravesical Pressure: A Prospective Cohort StudyDocument6 pagesEffect of Bladder Volume On Measured Intravesical Pressure: A Prospective Cohort StudyJimmy Israel Rodríguez LópezNo ratings yet
- What Is Infusion Pump?Document4 pagesWhat Is Infusion Pump?BMTNo ratings yet
- Smart Infusion Pump: A Boon To The Health Care IndustryDocument4 pagesSmart Infusion Pump: A Boon To The Health Care IndustryseventhsensegroupNo ratings yet
- Fitzpatrick 2005Document3 pagesFitzpatrick 2005A. J100% (1)
- Fda 2006 P 0073 0006Document34 pagesFda 2006 P 0073 0006milaNo ratings yet
- Fact Sheets Graseby 1200Document10 pagesFact Sheets Graseby 1200Cherry EstradaNo ratings yet
- Jingle Bell Rock - SATBDocument6 pagesJingle Bell Rock - SATBtonylee24100% (1)
- Troponin T Vs Troponin I ComparisonDocument9 pagesTroponin T Vs Troponin I Comparisontonylee1962No ratings yet
- IBS-Q For HCPDocument2 pagesIBS-Q For HCPtonylee24No ratings yet
- BAby It's Cold Outside (Duet)Document4 pagesBAby It's Cold Outside (Duet)tonylee24No ratings yet
- 2005 J Physiol-Brubakk-Single Air Dive Endothelial FunctionDocument6 pages2005 J Physiol-Brubakk-Single Air Dive Endothelial FunctionTony LeeNo ratings yet
- Hyperbaric Oxygen For Post Concussive SyndromeDocument28 pagesHyperbaric Oxygen For Post Concussive Syndrometonylee24No ratings yet
- Effects of Culture On Musical Pitch PerceptionDocument8 pagesEffects of Culture On Musical Pitch Perceptiontonylee24No ratings yet
- The Mechanism of Speech Processing in Congenital Amusia: Evidence From Mandarin SpeakersDocument11 pagesThe Mechanism of Speech Processing in Congenital Amusia: Evidence From Mandarin Speakerstonylee24No ratings yet
- HBO2 For FlapsDocument8 pagesHBO2 For Flapstonylee24No ratings yet
- Cross-Language Perception of Non-Native Tonal Contrasts: Effects of Native Phonological and Phonetic InfluencesDocument20 pagesCross-Language Perception of Non-Native Tonal Contrasts: Effects of Native Phonological and Phonetic Influencestonylee24No ratings yet
- Smoking Cessation in RSNDocument5 pagesSmoking Cessation in RSNtonylee24No ratings yet
- Hyperbaric Oxygen For Post Concussive SyndromeDocument28 pagesHyperbaric Oxygen For Post Concussive Syndrometonylee24No ratings yet
- The Linked Dual Representation Model of Vocal Perception and ProductionDocument12 pagesThe Linked Dual Representation Model of Vocal Perception and Productiontonylee24No ratings yet
- The Mechanism of Speech Processing in Congenital Amusia: Evidence From Mandarin SpeakersDocument11 pagesThe Mechanism of Speech Processing in Congenital Amusia: Evidence From Mandarin Speakerstonylee24No ratings yet
- Musical Experience Shapes Human Brainstem Encoding of Linguistic Pitch PatternsDocument7 pagesMusical Experience Shapes Human Brainstem Encoding of Linguistic Pitch Patternstonylee24No ratings yet
- A Dual-Stream Neuroanatomy of SingingDocument15 pagesA Dual-Stream Neuroanatomy of Singingtonylee24No ratings yet
- Musical Experience Shapes Human Brainstem Encoding of Linguistic Pitch PatternsDocument7 pagesMusical Experience Shapes Human Brainstem Encoding of Linguistic Pitch Patternstonylee24No ratings yet
- Congenital Amusia (Or Tone-Deafness) Interferes With Pitch Processing in Tone LanguagesDocument15 pagesCongenital Amusia (Or Tone-Deafness) Interferes With Pitch Processing in Tone Languagestonylee24No ratings yet
- Pitch Perception and Production in Congenital Amusia: Evidence From Cantonese SpeakersDocument13 pagesPitch Perception and Production in Congenital Amusia: Evidence From Cantonese Speakerstonylee24No ratings yet
- Relating Pitch Awareness To Phonemic Awareness in Children: Implications For Tone-Deafness and DyslexiaDocument5 pagesRelating Pitch Awareness To Phonemic Awareness in Children: Implications For Tone-Deafness and Dyslexiatonylee24No ratings yet
- Tone-Deafness - A New Disconnection Syndrome?Document14 pagesTone-Deafness - A New Disconnection Syndrome?tonylee24No ratings yet
- Action-Perception Mismatch in Tone-DeafnessDocument5 pagesAction-Perception Mismatch in Tone-Deafnesstonylee24No ratings yet
- Phonological Processing in Adults With Deficits in Musical Pitch RecognitionDocument13 pagesPhonological Processing in Adults With Deficits in Musical Pitch Recognitiontonylee24No ratings yet
- Musicians and Tone-Language Speakers Share Enhanced Brainstem Encoding But Not Perceptual Benefits For Musical PitchDocument23 pagesMusicians and Tone-Language Speakers Share Enhanced Brainstem Encoding But Not Perceptual Benefits For Musical Pitchtonylee24No ratings yet
- Brainstem Encoding of Speech and Musical StimDocument19 pagesBrainstem Encoding of Speech and Musical Stimtonylee24No ratings yet
- Tone Language Fluency Impairs Pitch DiscriminationDocument5 pagesTone Language Fluency Impairs Pitch Discriminationtonylee24No ratings yet
- The Genetics of Congenital Amusia (Tone Deafness) : A Family-Aggregation StudyDocument7 pagesThe Genetics of Congenital Amusia (Tone Deafness) : A Family-Aggregation Studytonylee24No ratings yet
- Widespread Auditory Deficits in Tune DeafnessDocument29 pagesWidespread Auditory Deficits in Tune Deafnesstonylee24No ratings yet
- Am J Hum Gen 2000 PDFDocument4 pagesAm J Hum Gen 2000 PDFtonylee24No ratings yet
- CIC-presentation of RP-577 PresentationDocument181 pagesCIC-presentation of RP-577 PresentationIbrahim Eldesoky75% (4)
- Way Back To The BibleDocument19 pagesWay Back To The BiblePearlCladelLapidezNo ratings yet
- Presentation - On SVAMITVADocument18 pagesPresentation - On SVAMITVAPraveen PrajapatiNo ratings yet
- Android Activity Lifecycle OverviewDocument8 pagesAndroid Activity Lifecycle OverviewMario FedericiNo ratings yet
- Ps1 GeneralDocument2 pagesPs1 Generalkulin123456No ratings yet
- Asme A112.4.14-2004 PDFDocument14 pagesAsme A112.4.14-2004 PDFAmer AmeryNo ratings yet
- A Review Paper On Rice Quality Analysis Using Image Processing TechniqueDocument5 pagesA Review Paper On Rice Quality Analysis Using Image Processing TechniqueIJRASETPublicationsNo ratings yet
- Muhammad Farrukh QAMAR - Assessment 2 Student Practical Demonstration of Tasks AURAMA006 V2Document19 pagesMuhammad Farrukh QAMAR - Assessment 2 Student Practical Demonstration of Tasks AURAMA006 V2Rana Muhammad Ashfaq Khan0% (1)
- FaucifilesDocument302 pagesFaucifilesLady WellingtonNo ratings yet
- Learn From Customers to Improve Products and ServicesDocument8 pagesLearn From Customers to Improve Products and ServicesQuan Hoang AnhNo ratings yet
- Logging Levels in Log4j - Tutorialspoint ExamplesDocument3 pagesLogging Levels in Log4j - Tutorialspoint ExamplesJai PannuNo ratings yet
- The Impact of COVID-19 On The Steel IndustryDocument25 pagesThe Impact of COVID-19 On The Steel IndustryAyesha KhalidNo ratings yet
- Astm A710Document3 pagesAstm A710Cristian Otivo100% (1)
- Banking and Fintech in 2022Document45 pagesBanking and Fintech in 2022Shahbaz talpurNo ratings yet
- The Black Emperor's Grand Grimoire - by Frank GenghisDocument144 pagesThe Black Emperor's Grand Grimoire - by Frank GenghisFrank Genghis0% (2)
- Arduino Mario Bros Tunes With Piezo Buzzer and PWMDocument6 pagesArduino Mario Bros Tunes With Piezo Buzzer and PWMClaudia GrijalvaNo ratings yet
- EAPP Report - Advertisement FallacyDocument13 pagesEAPP Report - Advertisement FallacyくんcharlsNo ratings yet
- Regina Downtown Community Support Team ReportDocument28 pagesRegina Downtown Community Support Team ReportJeremy SimesNo ratings yet
- Impact of Sugarcane Molasses in Concrete As Time Retarding and Water Reducing AdmixtureDocument131 pagesImpact of Sugarcane Molasses in Concrete As Time Retarding and Water Reducing AdmixtureMohamed MoralesNo ratings yet
- Calculate the proof strength of 70% v/v alcohol.Step 1) 70% v/v x 1.753 = 122.71Step 2) 122.71 - 100 = 22.71The proof strength of 70% v/v alcohol is 22.71% over proofDocument46 pagesCalculate the proof strength of 70% v/v alcohol.Step 1) 70% v/v x 1.753 = 122.71Step 2) 122.71 - 100 = 22.71The proof strength of 70% v/v alcohol is 22.71% over proofPrashant307100% (1)
- Brfo193 Radiotherapy Dose Fractionation Third-Edition PDFDocument137 pagesBrfo193 Radiotherapy Dose Fractionation Third-Edition PDFMed MedNo ratings yet
- Maruti Institute of Nursing, Itarsi: Maternal Nursing Child Health Nursing Medical Surgical Nursing Nursing FoundationDocument4 pagesMaruti Institute of Nursing, Itarsi: Maternal Nursing Child Health Nursing Medical Surgical Nursing Nursing FoundationHarshaNo ratings yet
- New Product Performance Advantages For Extending Large, Established Fast Moving Consumer Goods (FMCG) BrandsDocument18 pagesNew Product Performance Advantages For Extending Large, Established Fast Moving Consumer Goods (FMCG) Brandssmart_kidzNo ratings yet
- 1st Summative Test in Tle SmawDocument2 pages1st Summative Test in Tle Smawjenky agnoteNo ratings yet
- Set 177Document599 pagesSet 177adilfarooq25No ratings yet
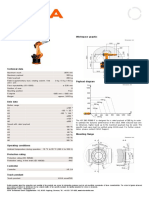
- KR 280 R3080 F technical specificationsDocument1 pageKR 280 R3080 F technical specificationsDorobantu CatalinNo ratings yet
- Installing Juniper Router OS JunOS 10 1 in Qemu VM For GNS3Document4 pagesInstalling Juniper Router OS JunOS 10 1 in Qemu VM For GNS3Adrian Ionut NituNo ratings yet
- Providing Clean Water and Financial Assistance in Binangonan RizalDocument29 pagesProviding Clean Water and Financial Assistance in Binangonan RizalArebeeJayBelloNo ratings yet
- Business Model Canvas TemplateDocument5 pagesBusiness Model Canvas TemplateAsraihan Raihan100% (1)