You might also like
- Department of Pathology, Dhanalakshmi Srinivasan Medical College and Hospital, Siruvachur, Perambalur, Tamil Nadu, IndiaDocument14 pagesDepartment of Pathology, Dhanalakshmi Srinivasan Medical College and Hospital, Siruvachur, Perambalur, Tamil Nadu, IndiaaishaNo ratings yet
- KDM - Sid's Record Sheets v1.5Document14 pagesKDM - Sid's Record Sheets v1.5Blackops559No ratings yet
- Interocclusal RecordsDocument8 pagesInterocclusal RecordsJohnNo ratings yet
- Somatic TherapiesDocument170 pagesSomatic TherapiesDelyn Gamutan Millan100% (2)
- Effective Screening10Document4 pagesEffective Screening10ponekNo ratings yet
- Cie 10Document11 pagesCie 10Gabriella MGNo ratings yet
- NIH Public Access: Author ManuscriptDocument18 pagesNIH Public Access: Author ManuscriptYosua_123No ratings yet
- ACCP Cxca Screening 2011Document8 pagesACCP Cxca Screening 2011Lizeth López LeónNo ratings yet
- 329-Article Text-1733-1-10-20211207Document10 pages329-Article Text-1733-1-10-20211207antaresNo ratings yet
- Jfac 142Document25 pagesJfac 142Ana Paula Giolo FranzNo ratings yet
- To Do or Not To Do The Choice: Is Yours!Document44 pagesTo Do or Not To Do The Choice: Is Yours!zynal20038222No ratings yet
- PIIS2213398422000902Document7 pagesPIIS2213398422000902Manas BhatiaNo ratings yet
- Cervical Cancer - HivDocument1 pageCervical Cancer - HivShaba KilasiNo ratings yet
- 2011 Article 342Document4 pages2011 Article 342Gilang IrwansyahNo ratings yet
- Artigo Sobre CancerDocument10 pagesArtigo Sobre CancerSérgio Anick da Silva Brito SegundoNo ratings yet
- Breast Cancer ScreeningDocument21 pagesBreast Cancer ScreeningBolivar Isea100% (1)
- Trends in Delayed Breast Cancer Diagnosis After ReDocument9 pagesTrends in Delayed Breast Cancer Diagnosis After ReeugeniaNo ratings yet
- Screening for cervical cancer overviewDocument8 pagesScreening for cervical cancer overviewNike Angela PatriciaNo ratings yet
- Correlation of Cervical Screening TestsDocument7 pagesCorrelation of Cervical Screening TestsMarcos HoilNo ratings yet
- Screen-and-Treat Approaches For Cervical Cancer Prevention in Low-Resource SettingsDocument9 pagesScreen-and-Treat Approaches For Cervical Cancer Prevention in Low-Resource SettingsSaddam FuadNo ratings yet
- ART20176809Document5 pagesART20176809dkhatri01No ratings yet
- Effective Screening23Document10 pagesEffective Screening23ponekNo ratings yet
- Incidence and Risk Factors of Cervical Cancer in BangladeshDocument56 pagesIncidence and Risk Factors of Cervical Cancer in BangladeshTanvir AhmedNo ratings yet
- Colposcopy, Cervical Screening, and HPV: A Guide to Prevention and ManagementDocument155 pagesColposcopy, Cervical Screening, and HPV: A Guide to Prevention and ManagementAnnca RoXanna100% (1)
- HPV Type Distribution in Invasive Cervical Cancer and High-Grade Cervical Intraepithelial Neoplasia AcDocument9 pagesHPV Type Distribution in Invasive Cervical Cancer and High-Grade Cervical Intraepithelial Neoplasia AcFeli FelNo ratings yet
- Clinical Significance of HPV-DNA Testing For Precancerous Cervical LesionsDocument3 pagesClinical Significance of HPV-DNA Testing For Precancerous Cervical LesionsGede S PutrawanNo ratings yet
- Breast CA ScreeningDocument8 pagesBreast CA Screeningchristelm_1No ratings yet
- Evidence-Based Cervical Cancer Screening for Low-Resource SettingsDocument6 pagesEvidence-Based Cervical Cancer Screening for Low-Resource Settingschica_asNo ratings yet
- Cervical Cytology in Women With Abnormal Cervix.: Dr. Veena Rahatgaonkar, Dr. Savita MehendaleDocument4 pagesCervical Cytology in Women With Abnormal Cervix.: Dr. Veena Rahatgaonkar, Dr. Savita MehendaleIOSR Journal of PharmacyNo ratings yet
- Performance and Diagnostic Accuracy of A Urine-Based Human Papillomavirus Assay in A Referral PopulationDocument7 pagesPerformance and Diagnostic Accuracy of A Urine-Based Human Papillomavirus Assay in A Referral PopulationJose de PapadopoulosNo ratings yet
- Full Title: Accuracy of Clinical Breast Examination's AbnormalitiesDocument21 pagesFull Title: Accuracy of Clinical Breast Examination's AbnormalitiesMaria AyaNo ratings yet
- Delivering Cervical Cancer Prevention in Low-Resource AreasDocument9 pagesDelivering Cervical Cancer Prevention in Low-Resource AreasSolihin HasnanNo ratings yet
- Cervical Cancer Screening With Human Papillomavirus DNA and Cytology in JapanDocument7 pagesCervical Cancer Screening With Human Papillomavirus DNA and Cytology in Japandella kharisma putriNo ratings yet
- Updates in Cervical Cytology: 90 Years of ProgressDocument11 pagesUpdates in Cervical Cytology: 90 Years of Progressmohamaed abbasNo ratings yet
- Study of Fine Needle Aspiration Cytology of Breast Lump: Correlation of Cytologically Malignant Cases With Their Histological FindingsDocument5 pagesStudy of Fine Needle Aspiration Cytology of Breast Lump: Correlation of Cytologically Malignant Cases With Their Histological FindingsArvind Vashi AroraNo ratings yet
- Cervical Cancer Screening and HPV Vaccine Acceptability Among Rural and Urban Women in Kilimanjaro Region, TanzaniaDocument9 pagesCervical Cancer Screening and HPV Vaccine Acceptability Among Rural and Urban Women in Kilimanjaro Region, TanzaniapangaribuansantaNo ratings yet
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument5 pagesBest Practice & Research Clinical Obstetrics and GynaecologyGeorge CarpNo ratings yet
- tmpF425 TMPDocument8 pagestmpF425 TMPFrontiersNo ratings yet
- Analytic Hierarchy Process in An Online QuestionnaireDocument84 pagesAnalytic Hierarchy Process in An Online QuestionnaireUlianti UmurahNo ratings yet
- Effect of Cervicitis On Visual Inspection With Acetic AcidDocument5 pagesEffect of Cervicitis On Visual Inspection With Acetic AcidmonicamoniccNo ratings yet
- A Major Issue in MedicineDocument29 pagesA Major Issue in MedicineSiti NajwaNo ratings yet
- Research Paper Cervical CancerDocument5 pagesResearch Paper Cervical Cancergz8bjzmj100% (1)
- e Tarjome E17331Document6 pagese Tarjome E17331فاطمه سادات قربانیNo ratings yet
- Mustafa 2016Document7 pagesMustafa 2016ejigsonNo ratings yet
- Identifying Normal Mammograms in A Large Screening Population Using Artificial IntelligenceDocument6 pagesIdentifying Normal Mammograms in A Large Screening Population Using Artificial IntelligenceDébora XavierNo ratings yet
- Pap TestDocument5 pagesPap Testimahere_suryaNo ratings yet
- MATERI WEBINAR PRODIA Ovarian CancerDocument57 pagesMATERI WEBINAR PRODIA Ovarian CancerSylvia LestariNo ratings yet
- Colorectal Cancer Screening: It Is Not Time For A Radical ShiftDocument2 pagesColorectal Cancer Screening: It Is Not Time For A Radical Shiftm_manuela2002No ratings yet
- Health Technology Assessment On Cervical Cancer Screening 20002014Document10 pagesHealth Technology Assessment On Cervical Cancer Screening 20002014Reni HariyantiNo ratings yet
- Thesis On Cervical Cancer ScreeningDocument6 pagesThesis On Cervical Cancer Screeningangelabaxtermanchester100% (1)
- Cervical Cancer Screening Literature ReviewDocument5 pagesCervical Cancer Screening Literature Reviewafdtovmhb100% (1)
- Oral Cancer Screening AidsDocument13 pagesOral Cancer Screening AidsnaveedtariqsyedNo ratings yet
- HPV and Cervical Cancer Research PaperDocument8 pagesHPV and Cervical Cancer Research Paperafmcuafnh100% (1)
- 19 - Benefits of Cervical Cancer Screening by Liquid-BasedDocument5 pages19 - Benefits of Cervical Cancer Screening by Liquid-BasedRenan RodriguesNo ratings yet
- Female Healthcare WorkersDocument9 pagesFemale Healthcare WorkersInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cancers 13 03840Document17 pagesCancers 13 03840Alaa OmarNo ratings yet
- Original 2Document6 pagesOriginal 2medusineNo ratings yet
- Bmjopen 2014 005828Document9 pagesBmjopen 2014 005828antidius johnNo ratings yet
- Management of Cervical CancerDocument29 pagesManagement of Cervical CancersangheetaNo ratings yet
- Omidiji 2017Document7 pagesOmidiji 2017Dewa OkaNo ratings yet
- Knowledge, Attitude and Practice Toward Cervical Cancer and Cervical Cancer Screening and Its Associated Factors Among Women in The City of Bamenda, CameroonDocument17 pagesKnowledge, Attitude and Practice Toward Cervical Cancer and Cervical Cancer Screening and Its Associated Factors Among Women in The City of Bamenda, CameroonEditor IJTSRDNo ratings yet
- Rapid On-site Evaluation (ROSE): A Practical GuideFrom EverandRapid On-site Evaluation (ROSE): A Practical GuideGuoping CaiNo ratings yet
- Breast Cancer in Young WomenFrom EverandBreast Cancer in Young WomenOreste GentiliniNo ratings yet
- Strategies Hospitalists Can Take To Prevent Antibiotic ResistanceDocument10 pagesStrategies Hospitalists Can Take To Prevent Antibiotic ResistanceponekNo ratings yet
- Amniotic Laser PhotocoagulationDocument18 pagesAmniotic Laser PhotocoagulationponekNo ratings yet
- Resource Job Aid Excluding PregnancyDocument2 pagesResource Job Aid Excluding PregnancyponekNo ratings yet
- Lesi Pra Kanker Serviks LeafletDocument1 pageLesi Pra Kanker Serviks LeafletponekNo ratings yet
- Fetal Monitor WirelessDocument1 pageFetal Monitor WirelessponekNo ratings yet
- Kanker ServiksDocument308 pagesKanker ServiksponekNo ratings yet
- Kanker ServiksDocument308 pagesKanker ServiksponekNo ratings yet
- Resource Checklists Screening Clients Who Want Initiate Use LNG Ius English 2017Document3 pagesResource Checklists Screening Clients Who Want Initiate Use LNG Ius English 2017ponekNo ratings yet
- Conization of The CervixDocument5 pagesConization of The CervixponekNo ratings yet
- Checklist Iud EnglishDocument3 pagesChecklist Iud EnglishponekNo ratings yet
- Skripsi Tanpa Bab PembahasanDocument84 pagesSkripsi Tanpa Bab PembahasanponekNo ratings yet
- Sadiq KhanDocument5 pagesSadiq KhanponekNo ratings yet
- Sadiq KhanDocument5 pagesSadiq KhanponekNo ratings yet
- Checklist Iud EnglishDocument3 pagesChecklist Iud EnglishponekNo ratings yet
- Scientific Schedule: Alarm Course Day 1Document11 pagesScientific Schedule: Alarm Course Day 1ponekNo ratings yet
- Skripsi Tanpa Bab PembahasanDocument84 pagesSkripsi Tanpa Bab PembahasanponekNo ratings yet
- Checklist Dmpa EnglishDocument3 pagesChecklist Dmpa EnglishponekNo ratings yet
- Scientific Schedule: Alarm Course Day 1Document11 pagesScientific Schedule: Alarm Course Day 1ponekNo ratings yet
- Pharmacology Cardiovascular1Document33 pagesPharmacology Cardiovascular1ponekNo ratings yet
- Caesarean SectionDocument51 pagesCaesarean SectionFebrinata MahadikaNo ratings yet
- BF and Early Nutrition Mother DMDocument44 pagesBF and Early Nutrition Mother DMponekNo ratings yet
- BF and Early Nutrition Mother DMDocument44 pagesBF and Early Nutrition Mother DMponekNo ratings yet
- NCDsDocument40 pagesNCDsponekNo ratings yet
- REFERAT - Check List VBAC Antenatal Periode PDFDocument2 pagesREFERAT - Check List VBAC Antenatal Periode PDFponekNo ratings yet
- REFERAT - Neonatal HSV InfectionDocument5 pagesREFERAT - Neonatal HSV InfectionponekNo ratings yet
- Resus - Makrosomia (Ardicho) - REFERAT Macrosomia Prediction Using USGDocument4 pagesResus - Makrosomia (Ardicho) - REFERAT Macrosomia Prediction Using USGponekNo ratings yet
- Preclinical Condition MagementDocument27 pagesPreclinical Condition MagementponekNo ratings yet
- REFERAT - Neonatal HSV InfectionDocument5 pagesREFERAT - Neonatal HSV InfectionponekNo ratings yet
- Guidline TetanusDocument363 pagesGuidline TetanusferianaNo ratings yet
- Pengendalian Pengadaan Alat Kesehatan Habis Pakai di RSBTDocument12 pagesPengendalian Pengadaan Alat Kesehatan Habis Pakai di RSBTponekNo ratings yet
- 3rd Year MUHS Winter 2022Document10 pages3rd Year MUHS Winter 2022Juned LabbaiNo ratings yet
- Transfusion-Related Acute Lung Injury (TRALI)Document20 pagesTransfusion-Related Acute Lung Injury (TRALI)WilliamRayCassidyNo ratings yet
- Form Audit ReagensiaDocument2 pagesForm Audit ReagensiaPaulina SetiatiNo ratings yet
- Urine Screening of Metabolic DisordersDocument24 pagesUrine Screening of Metabolic DisordersMark Arlo Hernandez SegundoNo ratings yet
- Basic ECG Interpretation Practice Test: DIRECTIONS: The Following Test Consists of 20 QuestionsDocument10 pagesBasic ECG Interpretation Practice Test: DIRECTIONS: The Following Test Consists of 20 Questionsmihaela_bondocNo ratings yet
- QiGong Global SummitDocument45 pagesQiGong Global SummittoanomisNo ratings yet
- RISE MagazineDocument20 pagesRISE MagazineMitch GastinNo ratings yet
- Lab and Blood Bank Safe DisposalDocument8 pagesLab and Blood Bank Safe DisposalShawqi AlmughniNo ratings yet
- Kate Laver's Primary FRCA Guide: My Revision (For Exam in June)Document3 pagesKate Laver's Primary FRCA Guide: My Revision (For Exam in June)M H DuNo ratings yet
- General Directory Site: Walter C. Mackenzie Health Sciences CentreDocument1 pageGeneral Directory Site: Walter C. Mackenzie Health Sciences CentreAli MullaNo ratings yet
- Jamaicas Health SystemsDocument33 pagesJamaicas Health Systemsgdudex118811No ratings yet
- Swings light from one eye to otherPatient: Pupil constricts only when light is shone on eye and not when light is shone on other eyeIndicates relative afferent pupillary defect (RAPDDocument39 pagesSwings light from one eye to otherPatient: Pupil constricts only when light is shone on eye and not when light is shone on other eyeIndicates relative afferent pupillary defect (RAPDAdarsh KeshariNo ratings yet
- 210-241 UrinaryDocument34 pages210-241 UrinaryYaj Cruzada100% (1)
- Register Meranti 2018Document178 pagesRegister Meranti 2018Rifat Bow AbdilahNo ratings yet
- NormaltestreportDocument1 pageNormaltestreportTayyeb KhanNo ratings yet
- ICAR JRF/SRF Exam Question Bank for Veterinary StudentsDocument281 pagesICAR JRF/SRF Exam Question Bank for Veterinary StudentsHarish ShindeNo ratings yet
- SJK (C) Chung Hua Lingga Monthly Test (1) Year 4 ScienceDocument21 pagesSJK (C) Chung Hua Lingga Monthly Test (1) Year 4 ScienceChia CassyNo ratings yet
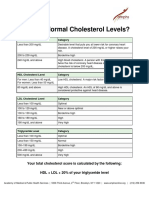
- Cholesterol Handout - ENGLDocument2 pagesCholesterol Handout - ENGLOladipupo Adejumobi LawalNo ratings yet
- MRCPI Part II Obstetric & Gynecology Exam FormatDocument3 pagesMRCPI Part II Obstetric & Gynecology Exam FormatNitasha Maqsood100% (1)
- Analyzing alleged "bittenDocument7 pagesAnalyzing alleged "bittenvi tiNo ratings yet
- Final Medicine Bulletin 2017 18Document339 pagesFinal Medicine Bulletin 2017 18Avramut IulianNo ratings yet
- Nutrition, aging, and sleep changes in older adultsDocument21 pagesNutrition, aging, and sleep changes in older adultsChester NicoleNo ratings yet
- Blocking Polyspermy and Pregnancy Tests ExplainedDocument13 pagesBlocking Polyspermy and Pregnancy Tests ExplainedHafizah ZakiahNo ratings yet
- Play It As It Lays EssayDocument6 pagesPlay It As It Lays Essayapi-474677222No ratings yet
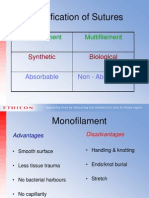
- Classification of Sutures: Monofilament MultifilamentDocument17 pagesClassification of Sutures: Monofilament Multifilamentlina_m354No ratings yet
- VasectomyDocument60 pagesVasectomyVlad ValentinNo ratings yet
- EUCOMP Glossaries Provide Comparable Health Care DataDocument341 pagesEUCOMP Glossaries Provide Comparable Health Care DataDiana IorgulescuNo ratings yet