You might also like
- Syncope CasesFrom EverandSyncope CasesRoberto García-CiveraNo ratings yet
- Basic Concept On NeuroanesthesiaDocument51 pagesBasic Concept On Neuroanesthesiabrojeem100% (1)
- Post Resus CareDocument35 pagesPost Resus Caredrjaikrish100% (1)
- Hypothermia For Brain Protection: Hipotermia Untuk Proteksi OtakDocument13 pagesHypothermia For Brain Protection: Hipotermia Untuk Proteksi OtakIndahKybingEinsteinNo ratings yet
- Perinatal Asphyxia: Prepared by Johannes NegesseDocument24 pagesPerinatal Asphyxia: Prepared by Johannes NegesseJhon NegesseNo ratings yet
- Curs 2-Managementul Pacientului Cu TCCDocument46 pagesCurs 2-Managementul Pacientului Cu TCCMarina ApostolNo ratings yet
- Pre-hospital Airway Management Guide for TBIDocument46 pagesPre-hospital Airway Management Guide for TBIMarius AlexandrescuNo ratings yet
- Disusun Oleh: Yoel Junio - 406171045 Pembimbing: Dr. Budi SP - AnDocument28 pagesDisusun Oleh: Yoel Junio - 406171045 Pembimbing: Dr. Budi SP - AnFelecia ChristyNo ratings yet
- PERIOPERATIVE MANAGEMENT OF BRAIN TRAUMADocument52 pagesPERIOPERATIVE MANAGEMENT OF BRAIN TRAUMAKimbek BuangkeNo ratings yet
- Brain Protection and ResuscitationDocument25 pagesBrain Protection and Resuscitationcitra dewiNo ratings yet
- Hypoxic Ischemic EncephalopathyDocument10 pagesHypoxic Ischemic EncephalopathyPadmaNo ratings yet
- Post-Cardiac Arrest Care ProtocolsDocument28 pagesPost-Cardiac Arrest Care ProtocolsAkib ArmanNo ratings yet
- Anesthesia For Supratentorial TumorsDocument68 pagesAnesthesia For Supratentorial TumorsnicoleoprollamanteNo ratings yet
- Traumatic Brain Injury PresentationDocument51 pagesTraumatic Brain Injury PresentationKah Sui Tan100% (2)
- Lec30 - Brain Protection and ResuscitationDocument30 pagesLec30 - Brain Protection and Resuscitationcitra dewiNo ratings yet
- Metabolic Coma DRDocument32 pagesMetabolic Coma DRKintan UtamiNo ratings yet
- RSCH TBI Guideline - v2Document32 pagesRSCH TBI Guideline - v2Edson Ricardo Lagos DominguezNo ratings yet
- Icu 2Document57 pagesIcu 2AMIT KUMAR DEYNo ratings yet
- Brain Death DiagnosisDocument86 pagesBrain Death Diagnosisharsha mummaka100% (1)
- D. Intralipid 20%: A. Temazepam B. Lorazepam C. NaloxoneDocument122 pagesD. Intralipid 20%: A. Temazepam B. Lorazepam C. NaloxoneOstazNo ratings yet
- Nervous System AlterationsDocument45 pagesNervous System AlterationsMajesty ParkerNo ratings yet
- Managing Brain Injury AnesthesiaDocument62 pagesManaging Brain Injury AnesthesiaKelvin KelvinNo ratings yet
- Outline Notes of CS 37-38 - Neurological TraumaDocument13 pagesOutline Notes of CS 37-38 - Neurological TraumaTaif SalimNo ratings yet
- Traumatic Care DR - GOLDENDocument34 pagesTraumatic Care DR - GOLDENBayu PutraNo ratings yet
- II-E Altered PerceptionDocument16 pagesII-E Altered PerceptionDharylle CariñoNo ratings yet
- Perinatal Asphyxia: For C-IDocument35 pagesPerinatal Asphyxia: For C-IYemata HailuNo ratings yet
- Raised Intracranial Pressure: BY DR - Tallat Pervaiz AliDocument37 pagesRaised Intracranial Pressure: BY DR - Tallat Pervaiz AliCh Khurram HasnainNo ratings yet
- Examination of The Comatose PatientDocument9 pagesExamination of The Comatose Patientakrw90No ratings yet
- Perinatal Asphyxia - Outline of Pathophysiology and Recent Trends in ManagementDocument31 pagesPerinatal Asphyxia - Outline of Pathophysiology and Recent Trends in Managementokwadha simionNo ratings yet
- Clinical Applications of Induced Hypothermia: Mark Luscombe John C AndrzejowskiDocument5 pagesClinical Applications of Induced Hypothermia: Mark Luscombe John C AndrzejowskiSajid NadafNo ratings yet
- How to Approach Comatose PatientsDocument37 pagesHow to Approach Comatose PatientsHuzefa MemonNo ratings yet
- Myasthenia Gravis: An Overview of Its Anatomy, Pathophysiology, Clinical Presentation, Diagnosis and TreatmentDocument41 pagesMyasthenia Gravis: An Overview of Its Anatomy, Pathophysiology, Clinical Presentation, Diagnosis and TreatmentNofilia Citra CandraNo ratings yet
- Intensive Care After Neurosurgery: Saeed Abbasi, MD, FCCMDocument81 pagesIntensive Care After Neurosurgery: Saeed Abbasi, MD, FCCMYen NgoNo ratings yet
- Head Injury Management: Ahimbisibwe Alaphael Lecturer DR - JulietDocument33 pagesHead Injury Management: Ahimbisibwe Alaphael Lecturer DR - JulietNinaNo ratings yet
- Aldrette Score (Nitasha Best) (Discharge Criteria From Pacu)Document72 pagesAldrette Score (Nitasha Best) (Discharge Criteria From Pacu)Parvathy R NairNo ratings yet
- EMD2 - K9 - Status EpilepticusDocument37 pagesEMD2 - K9 - Status EpilepticusJessica WijayaNo ratings yet
- Mrcs TrumaDocument120 pagesMrcs TrumaDoctor EbrahimNo ratings yet
- Shock & MODS: Understanding Types & Managing PatientsDocument20 pagesShock & MODS: Understanding Types & Managing PatientsFemale calmNo ratings yet
- Shock Said 20-21Document10 pagesShock Said 20-212859bathinaNo ratings yet
- Anesthetic Agents: VbanetDocument26 pagesAnesthetic Agents: Vbanetdona0010100% (1)
- Perinatal AsphyxiaDocument24 pagesPerinatal AsphyxiaZazzZaffaNo ratings yet
- Post Operative CareDocument67 pagesPost Operative Care5alifa55No ratings yet
- Neuro CCNDocument5 pagesNeuro CCNShy Dela PuertaNo ratings yet
- Emergency Neurological Life Support: Intracranial Hypertension and HerniationDocument7 pagesEmergency Neurological Life Support: Intracranial Hypertension and HerniationPablo IgnacioNo ratings yet
- 6 PacuDocument15 pages6 PacuFarrukh Ali KhanNo ratings yet
- Pharm Care in Stroke-1Document45 pagesPharm Care in Stroke-1Achmad Triwidodo AmoeNo ratings yet
- Cerebro Vascular DiseaseDocument25 pagesCerebro Vascular DiseaseMuhammad Asif NizamiNo ratings yet
- Journal Reading Acute Spinal Cord InjuryDocument14 pagesJournal Reading Acute Spinal Cord InjuryamandaNo ratings yet
- SYOKDocument76 pagesSYOKRiri EltadezaNo ratings yet
- Guidelines For The Management of Severe Traumatic Brain Injury 4th EditionDocument62 pagesGuidelines For The Management of Severe Traumatic Brain Injury 4th EditionNailahRahmahNo ratings yet
- Evidence-Based Principles OF Stroke ManagementDocument61 pagesEvidence-Based Principles OF Stroke ManagementBenjamin PrabhuNo ratings yet
- Neurological Disorders Key NotesDocument31 pagesNeurological Disorders Key NotesHannah aswiniNo ratings yet
- Shock: Asuhan Keperawatan Gawat DaruratDocument31 pagesShock: Asuhan Keperawatan Gawat DaruratNovia DepeNo ratings yet
- Van de Wiele 01 PDFDocument36 pagesVan de Wiele 01 PDFbiraj majumderNo ratings yet
- Neurologic and Neurosurgical Emergencies For Nursing StudentsDocument39 pagesNeurologic and Neurosurgical Emergencies For Nursing StudentsDr Ganeshgouda MajigoudraNo ratings yet
- Hypoxic Ischemic EncephalopathyDocument33 pagesHypoxic Ischemic EncephalopathyDr.P.NatarajanNo ratings yet
- Penanganan Cedera KepalaDocument28 pagesPenanganan Cedera KepalaRichesio Sapata TomokumoroNo ratings yet
- Cara Mengatasi Cedera Kepala Berat di UGDDocument28 pagesCara Mengatasi Cedera Kepala Berat di UGDJonathan wiradinataNo ratings yet
- BRAIN DEATH ROLE OF IntensivistDocument41 pagesBRAIN DEATH ROLE OF Intensivistharsha mummakaNo ratings yet
- 167 FullDocument5 pages167 FullTina HerreraNo ratings yet
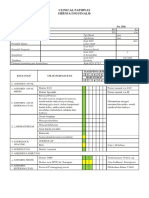
- CP AppendectomyDocument6 pagesCP AppendectomyTina HerreraNo ratings yet
- Pie 2018Document5 pagesPie 2018Tina HerreraNo ratings yet
- Clinical Pathway for Inguinal Hernia RepairDocument6 pagesClinical Pathway for Inguinal Hernia RepairTina HerreraNo ratings yet
- Clinical Pathway Limphadenopaty ColiDocument6 pagesClinical Pathway Limphadenopaty ColiTina HerreraNo ratings yet
- Clinical Pathway Apendisitis AcutaDocument7 pagesClinical Pathway Apendisitis AcutaTina HerreraNo ratings yet
- Jurnal PoneDocument21 pagesJurnal PoneTina HerreraNo ratings yet
- Tumor Immune Escape Mechanisms: Yi Ting Koh,, M. Luz García-Hernández,, and W. Martin KastDocument26 pagesTumor Immune Escape Mechanisms: Yi Ting Koh,, M. Luz García-Hernández,, and W. Martin KastTina HerreraNo ratings yet
- Guia de Bologna-2013Document14 pagesGuia de Bologna-2013andreigustvNo ratings yet
- Comparing Propranolol and Corticosteroids for Pediatric HemangiomasDocument9 pagesComparing Propranolol and Corticosteroids for Pediatric HemangiomasTina HerreraNo ratings yet
- CP Early Breast CancerDocument8 pagesCP Early Breast CancerTina HerreraNo ratings yet
- Aaam Face Thread c5 2019 FlyerDocument1 pageAaam Face Thread c5 2019 FlyerTina HerreraNo ratings yet
- Aaam Face Thread c5 2019 FlyerDocument1 pageAaam Face Thread c5 2019 FlyerTina HerreraNo ratings yet
- Controversy in Head Injury, Abdul Hafid PDFDocument31 pagesControversy in Head Injury, Abdul Hafid PDFTina HerreraNo ratings yet
- Comparing Propranolol and Corticosteroids for Pediatric HemangiomasDocument9 pagesComparing Propranolol and Corticosteroids for Pediatric HemangiomasTina HerreraNo ratings yet
- Controversy in Head Injury, Abdul Hafid PDFDocument31 pagesControversy in Head Injury, Abdul Hafid PDFTina HerreraNo ratings yet
- Biomolecular and Immunological, Sofia MDocument64 pagesBiomolecular and Immunological, Sofia MTina HerreraNo ratings yet
- National Guideline, Peter LDocument51 pagesNational Guideline, Peter LTina HerreraNo ratings yet
- Intracranial Pathophysiology, Zainal MDocument25 pagesIntracranial Pathophysiology, Zainal MTina HerreraNo ratings yet
- Thoracic Lumbar, Eko AgusDocument32 pagesThoracic Lumbar, Eko AgusTina HerreraNo ratings yet
- Brain Protection, M.Ramli PDFDocument50 pagesBrain Protection, M.Ramli PDFTina HerreraNo ratings yet
- Biomelecular Aspect, Irawan YusufDocument23 pagesBiomelecular Aspect, Irawan YusufTina HerreraNo ratings yet
- Pharmacotherapy of Traumatic Brain Injury (2015)Document6 pagesPharmacotherapy of Traumatic Brain Injury (2015)Tina HerreraNo ratings yet
- Pre-Hospital Severe Traumatic Brain Injury - Comparison of Outcome in Paramedic Versus Physician Staffed Emergency Medical Services (2016)Document7 pagesPre-Hospital Severe Traumatic Brain Injury - Comparison of Outcome in Paramedic Versus Physician Staffed Emergency Medical Services (2016)Tina HerreraNo ratings yet
- Outcome of Surgically Treated Traumatic Extradural Hematoma (2016)Document9 pagesOutcome of Surgically Treated Traumatic Extradural Hematoma (2016)Tina HerreraNo ratings yet
- Brain Protection, M.Ramli PDFDocument50 pagesBrain Protection, M.Ramli PDFTina HerreraNo ratings yet
- Soal Ujian NeurotraumaDocument22 pagesSoal Ujian NeurotraumaTina HerreraNo ratings yet
- Jurnal NCDocument12 pagesJurnal NCTina HerreraNo ratings yet