You might also like
- Mental Health BundleDocument55 pagesMental Health BundleEmma Daisy100% (1)
- FCE Word FormationDocument26 pagesFCE Word FormationThu ThủyNo ratings yet
- Ebtisam DTPDocument20 pagesEbtisam DTPAnup Lal RajbahakNo ratings yet
- Visiting The Dentist - Efe Gita Nov22023Document13 pagesVisiting The Dentist - Efe Gita Nov22023billahNo ratings yet
- Patient's Personal Details Form 1: CHI NumberDocument20 pagesPatient's Personal Details Form 1: CHI Numberdentalupdate123No ratings yet
- Corah's Dental Anxiety Scale, Revised (DAS-R) Dental-Phobia-Screening-ToolDocument1 pageCorah's Dental Anxiety Scale, Revised (DAS-R) Dental-Phobia-Screening-ToolChristiana TomescuNo ratings yet
- Social and Dental History Form 2: CHI NumberDocument2 pagesSocial and Dental History Form 2: CHI NumbermebibegNo ratings yet
- Tapping for Dental Fear and Anxiety: Simple Steps to Clear the Fear and Love Your Dentist AgainFrom EverandTapping for Dental Fear and Anxiety: Simple Steps to Clear the Fear and Love Your Dentist AgainNo ratings yet
- Checking Patient IdentitypptxDocument45 pagesChecking Patient IdentitypptxKurnihayati MuklasNo ratings yet
- Toothache Terminator : Natural Remedies for Rapid Relief: Home RemediesFrom EverandToothache Terminator : Natural Remedies for Rapid Relief: Home RemediesNo ratings yet
- Materi Bahasa Inggris Kelas Xi Semester GenapDocument15 pagesMateri Bahasa Inggris Kelas Xi Semester GenapTotok SaputroNo ratings yet
- New Patient Health History Form - Art of DentistryDocument4 pagesNew Patient Health History Form - Art of DentistryGiovanna L BarajasNo ratings yet
- NSPT Role PlayDocument10 pagesNSPT Role Playapi-284521361No ratings yet
- Impacted Wisdom Tooth, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandImpacted Wisdom Tooth, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Body LanguageDocument75 pagesBody LanguageCodrescu AncaNo ratings yet
- Visiting The Dentist British English StudentDocument4 pagesVisiting The Dentist British English StudentClement MenlahNo ratings yet
- Visiting The Dentist British English StudentDocument4 pagesVisiting The Dentist British English StudentEnglish Learning CenterNo ratings yet
- Learning Material Topic 9 Oral Hygiene and Denture CareDocument6 pagesLearning Material Topic 9 Oral Hygiene and Denture CareMuhammad Fajar NugrahaNo ratings yet
- SoravJain'sReelMasteryWorkbook 2Document4 pagesSoravJain'sReelMasteryWorkbook 2Sunny KapoorNo ratings yet
- At The Dentist British English StudentDocument4 pagesAt The Dentist British English StudentАнгелина СветличнаяNo ratings yet
- Visiting The Dentist British English TeacherDocument7 pagesVisiting The Dentist British English Teachero.potitskaNo ratings yet
- MODUL SMK 1Document16 pagesMODUL SMK 1dodi suprayogiNo ratings yet
- ECC ExampleDocument20 pagesECC ExampleNicole BrinkNo ratings yet
- Learning Material Topic 6 (Putri Pebriati.2a)Document4 pagesLearning Material Topic 6 (Putri Pebriati.2a)Icha siti AisyahNo ratings yet
- HelloDocument34 pagesHelloCorina CucoșNo ratings yet
- Teens 3A Revision Carrousel Unit 3 2024 THDocument97 pagesTeens 3A Revision Carrousel Unit 3 2024 THcharlotteNo ratings yet
- 76 - Going To The Dentist - USDocument10 pages76 - Going To The Dentist - USelafNo ratings yet
- AnnoyanceDocument7 pagesAnnoyanceZeeNo ratings yet
- Dental Abscess, (Gum Boil) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDental Abscess, (Gum Boil) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Checking Patient Detail: Kurnihayati, M.PDDocument49 pagesChecking Patient Detail: Kurnihayati, M.PDFardan Putra SeptiawanNo ratings yet
- Learning Material Topic 6 Nose, Mouth, and Throat AssessmentDocument7 pagesLearning Material Topic 6 Nose, Mouth, and Throat AssessmentMuhammad Fajar NugrahaNo ratings yet
- Report Language and ChecklistDocument7 pagesReport Language and ChecklisteuzieNo ratings yet
- Expressing Opinion: IELTS Speaking Class IELTS Preparation Programme Leiden Institute 2019Document8 pagesExpressing Opinion: IELTS Speaking Class IELTS Preparation Programme Leiden Institute 2019Wardiati YusufNo ratings yet
- At The Dentist British English StudentDocument4 pagesAt The Dentist British English StudentClement MenlahNo ratings yet
- At The Dentist British English StudentDocument4 pagesAt The Dentist British English Studentkonsik.wioletaNo ratings yet
- Roadmap B2Document19 pagesRoadmap B2KaterynaNo ratings yet
- Tinnitus Handicap Inventory (THI)Document4 pagesTinnitus Handicap Inventory (THI)Dian SetyaningrumNo ratings yet
- Menopause Type QuestionnaireDocument2 pagesMenopause Type QuestionnairenhsajibNo ratings yet
- Homework Ideas For TeethDocument9 pagesHomework Ideas For Teethcfk3ncft100% (1)
- How to Keep Your Teeth for a Lifetime: What You Should Know About Caring for Your TeethFrom EverandHow to Keep Your Teeth for a Lifetime: What You Should Know About Caring for Your TeethNo ratings yet
- Blanche GrubeDocument21 pagesBlanche GrubesangroniscarlosNo ratings yet
- InterjectionDocument7 pagesInterjectionMartin DiazNo ratings yet
- Smile: Healthy Teet. Healthy BodyDocument10 pagesSmile: Healthy Teet. Healthy BodyJohanna KendallNo ratings yet
- Going To The Dentist Vocabulary Word List: A D H N SDocument24 pagesGoing To The Dentist Vocabulary Word List: A D H N Smiha_bz100% (1)
- 7b Oral Health Impact ProfileDocument2 pages7b Oral Health Impact ProfileTria Sesar AprianiNo ratings yet
- Contoh Kuesioner Modal SosialDocument16 pagesContoh Kuesioner Modal SosialSinta MaysilaNo ratings yet
- Dental FearsDocument10 pagesDental Fearshantimurova.nNo ratings yet
- Tooth Decay Easy Read GuideDocument29 pagesTooth Decay Easy Read GuideSTEM JordanNo ratings yet
- Well Being QuestionnaireDocument9 pagesWell Being QuestionnaireHafiz HassanNo ratings yet
- Mouth Assessment RubricDocument5 pagesMouth Assessment RubricChris SmithNo ratings yet
- Dialogue: Expressing One's OpinionDocument19 pagesDialogue: Expressing One's OpinionBugheanuNo ratings yet
- Deborah Olenev, C.C.H.: Homeopathic Questionnaire For Case TakingDocument5 pagesDeborah Olenev, C.C.H.: Homeopathic Questionnaire For Case Takingmonique_sm28No ratings yet
- Index of Marital SatisfactionDocument7 pagesIndex of Marital SatisfactionlawoffistsNo ratings yet
- DR - Steven Navel's Dental HealthDocument40 pagesDR - Steven Navel's Dental HealthGeorgiana IlincaNo ratings yet
- GingivitisDocument3 pagesGingivitisHiếu Nguyễn ĐứcNo ratings yet
- Why Do You Fear The Dentist?: o o o o o o o o o o o oDocument2 pagesWhy Do You Fear The Dentist?: o o o o o o o o o o o okevinbuscemiNo ratings yet
- My Health First: The Latest NewsDocument4 pagesMy Health First: The Latest NewsSophia CullNo ratings yet
- Intermediate 09 Unit 2 PPT 8 (Pages 20-21)Document24 pagesIntermediate 09 Unit 2 PPT 8 (Pages 20-21)DYNo ratings yet
- At The Dentist British English TeacherDocument6 pagesAt The Dentist British English TeacherAki AgoNo ratings yet
- Questionnaire For Tic TacDocument2 pagesQuestionnaire For Tic Tacprateekgm001100% (1)
- When Is Oral Biopsy Not Needed?Document6 pagesWhen Is Oral Biopsy Not Needed?Bibek RajNo ratings yet
- QDWPlicDocument2 pagesQDWPlicBibek RajNo ratings yet
- For Mucocele Lesions - Careful Excisional BiopsyDocument11 pagesFor Mucocele Lesions - Careful Excisional BiopsyBibek RajNo ratings yet
- Curriculum Vitae: Personal DetailsDocument3 pagesCurriculum Vitae: Personal DetailsBibek RajNo ratings yet
- 3 UhnjkcDocument8 pages3 UhnjkcBibek RajNo ratings yet
- Biopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Document5 pagesBiopsy Is Derived From A Greek Word (By-Op-See) Bio - Meaning LIFE and Opsy - TO LOOK (Vision)Bibek RajNo ratings yet
- Inflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryDocument73 pagesInflammation: Presenter: Priyanka Shah Junior Resident Department of Pedodontics and Preventive DentistryBibek RajNo ratings yet
- JdsmcxnksDocument32 pagesJdsmcxnksBibek RajNo ratings yet
- JDJDJDJDocument23 pagesJDJDJDJBibek RajNo ratings yet
- Practical Skill Station Basic Life Support Key Teaching ObjectivesDocument3 pagesPractical Skill Station Basic Life Support Key Teaching ObjectivesBibek RajNo ratings yet
- Trapezoidal Flap. A Diagrammatic IllustrationDocument6 pagesTrapezoidal Flap. A Diagrammatic IllustrationBibek RajNo ratings yet
- DhdifogkDocument4 pagesDhdifogkBibek RajNo ratings yet
- Vitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsDocument6 pagesVitamin B-Functions, Food Sources and RDA Value Deficiency and Their Oral ManifestationsBibek RajNo ratings yet
- DrtfygbyuijDocument29 pagesDrtfygbyuijBibek RajNo ratings yet
- YudsbhcjDocument1 pageYudsbhcjBibek RajNo ratings yet
- YuybnunhhuhbDocument2 pagesYuybnunhhuhbBibek RajNo ratings yet
- FfghhthjgvyujhDocument1 pageFfghhthjgvyujhBibek RajNo ratings yet
- Background Methods: Review' (OHAR) Guidance in BriefDocument1 pageBackground Methods: Review' (OHAR) Guidance in BriefBibek RajNo ratings yet
- Background Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieDocument1 pageBackground Triads Framework: Jan Clarkson, Craig Ramsay, Linda Young, Paula Elouafkaoui and Heather CassieBibek RajNo ratings yet
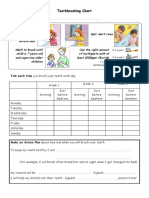
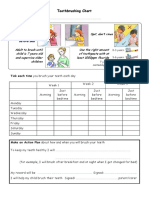
- Toothbrushing Chart PDFDocument1 pageToothbrushing Chart PDFBibek RajNo ratings yet
- Toothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayDocument1 pageToothbrushing Chart: Tick Each Time You Brush Your Teeth Each DayBibek RajNo ratings yet
- Ultrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationDocument2 pagesUltrasonic Cleaner Test Record: Ultrasonic Serial Number - LocationBibek RajNo ratings yet
- VfyggdbDocument33 pagesVfyggdbBibek RajNo ratings yet
- Warfarin and Your Dental Treatment: Information For PatientsDocument5 pagesWarfarin and Your Dental Treatment: Information For PatientsBibek RajNo ratings yet
- Rapid: Reducing Antibiotic Prescribing in DentistryDocument5 pagesRapid: Reducing Antibiotic Prescribing in DentistryBibek RajNo ratings yet
- TG 6 YhunjDocument48 pagesTG 6 YhunjBibek RajNo ratings yet
- Polestar BrousureDocument20 pagesPolestar BrousureB MNo ratings yet
- DSP-List NamibiaDocument10 pagesDSP-List NamibiaPerera KusalNo ratings yet
- Paeds 2023Document7 pagesPaeds 2023ct303 uuuNo ratings yet
- Seminar QuestionsDocument1 pageSeminar QuestionsIAMVIBENo ratings yet
- A Color Atlas of Diseases of The Eye and Skin PDFDocument416 pagesA Color Atlas of Diseases of The Eye and Skin PDFyaraamadoNo ratings yet
- Demographic and Clinical Profile of Patients Who Underwent Refractive Surgery ScreeningDocument8 pagesDemographic and Clinical Profile of Patients Who Underwent Refractive Surgery ScreeningPierre A. RodulfoNo ratings yet
- Guillain Barre SyndromeDocument19 pagesGuillain Barre SyndromeCrisMartAgullanaNo ratings yet
- Guide To Passing Primary FRCA 2014 Update1 PDFDocument9 pagesGuide To Passing Primary FRCA 2014 Update1 PDFSuhas KapseNo ratings yet
- ImmunologyDocument92 pagesImmunology[161]Shuaib AktherNo ratings yet
- 15-En Asfa Water Test ReportDocument47 pages15-En Asfa Water Test ReportTrọng Anh DươngNo ratings yet
- Drug Name Magnified Effects With AlcoholDocument1 pageDrug Name Magnified Effects With AlcoholMuhibpi IbrahimNo ratings yet
- Chaturvedi 2004Document2 pagesChaturvedi 2004Umer HussainNo ratings yet
- Meditech Downtime QRG 4 15 10Document6 pagesMeditech Downtime QRG 4 15 10Katarina CombsNo ratings yet
- Steroids Conversion Chart & ANTI-Coagulant Chart For Covid CasesDocument3 pagesSteroids Conversion Chart & ANTI-Coagulant Chart For Covid CasesJashveerBediNo ratings yet
- Venipuncture RubricDocument1 pageVenipuncture Rubricdever2017No ratings yet
- ErythropoiesisDocument11 pagesErythropoiesisْNo ratings yet
- Different Faces of HIV in A Single Patient: Case StudyDocument3 pagesDifferent Faces of HIV in A Single Patient: Case StudyAdvanced Research PublicationsNo ratings yet
- Occurrence of Candida Albicans in Periodontitis PDFDocument7 pagesOccurrence of Candida Albicans in Periodontitis PDFAbdoNo ratings yet
- 0 - MDI-P (Precursor ASEA) - Studiu Efect Germeni Agresivi - Baltch 2000Document7 pages0 - MDI-P (Precursor ASEA) - Studiu Efect Germeni Agresivi - Baltch 2000andrushkkutzaNo ratings yet
- EdcDocument3 pagesEdcJohnjohn MateoNo ratings yet
- DementiaDocument20 pagesDementiaUsama AliNo ratings yet
- Infection and Bacterial InvasionDocument40 pagesInfection and Bacterial InvasionTrisha BravoNo ratings yet
- Evidence-Based Treatment of Attention Deficit/ Hyperactivity Disorder in A Preschool-Age Child: A Case StudyDocument10 pagesEvidence-Based Treatment of Attention Deficit/ Hyperactivity Disorder in A Preschool-Age Child: A Case StudyCristinaNo ratings yet
- Dexmedetomidine Vs Propofol - RCT - Merry Andriany 406162043Document7 pagesDexmedetomidine Vs Propofol - RCT - Merry Andriany 406162043Merry AndrianyNo ratings yet
- 영상 의학과3Document11 pages영상 의학과3eosfieldNo ratings yet
- Basic EchocardiographyDocument54 pagesBasic Echocardiographyramon100% (23)
- Clinical and Psychometric Validation of The Geriatric Depression Scale GDS For Portuguese EldersDocument15 pagesClinical and Psychometric Validation of The Geriatric Depression Scale GDS For Portuguese EldersTeresa GasparNo ratings yet
- PPAG Alcohol Content in Peds Meds Poster-4!10!18Document2 pagesPPAG Alcohol Content in Peds Meds Poster-4!10!18herlinaNo ratings yet
- General Science Solutions For Class 8 Science Chapter 2Document6 pagesGeneral Science Solutions For Class 8 Science Chapter 2Ashwini KhareNo ratings yet
- TaeniasisDocument4 pagesTaeniasisSigrid MNo ratings yet