You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Business Plan WeldingDocument28 pagesBusiness Plan WeldingAnonymous yXn8m6V100% (5)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- Original PDF Basic Building and Construction Skills 5th Australia Edition PDFDocument41 pagesOriginal PDF Basic Building and Construction Skills 5th Australia Edition PDFryan.whitson353100% (35)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- AMB 172-014 Frame Cad OperationDocument3 pagesAMB 172-014 Frame Cad OperationRues AgNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- RSDP 24 Years AssesmentDocument184 pagesRSDP 24 Years AssesmentAdi100% (3)
- ENMAX Principles Business EthicsDocument34 pagesENMAX Principles Business EthicsStoryKingNo ratings yet
- IM Revalida Review 2019Document75 pagesIM Revalida Review 2019Nathaniel CamangonNo ratings yet
- Genetic Engineering 2nd HalfDocument55 pagesGenetic Engineering 2nd HalfNathaniel CamangonNo ratings yet
- Ust-Fms 2A-Med 1 Shift A.Y. 2016-2017: Yellow GreenDocument6 pagesUst-Fms 2A-Med 1 Shift A.Y. 2016-2017: Yellow GreenNathaniel CamangonNo ratings yet
- Sahara Project Earth SciDocument2 pagesSahara Project Earth SciNathaniel CamangonNo ratings yet
- Measuring The Economy: Statistics and IssuesDocument42 pagesMeasuring The Economy: Statistics and IssuesNathaniel CamangonNo ratings yet
- The Genetic CodeDocument5 pagesThe Genetic CodeNathaniel CamangonNo ratings yet
- Skeletal Muscles DissectionDocument14 pagesSkeletal Muscles DissectionNathaniel CamangonNo ratings yet
- Isolation and Characterization of Complex Lipids From Chicken BrainDocument8 pagesIsolation and Characterization of Complex Lipids From Chicken BrainMaria Christina PaineNo ratings yet
- Muscular System Laboratory Guide: Dissection of The Muscles: See Pages 229-230 in The Lab ManualDocument16 pagesMuscular System Laboratory Guide: Dissection of The Muscles: See Pages 229-230 in The Lab ManualNathaniel CamangonNo ratings yet
- Anhydrous Ammonia Chemical Release Lake County Illinois April 2019Document5 pagesAnhydrous Ammonia Chemical Release Lake County Illinois April 2019eduardo moritzNo ratings yet
- Safety Data Sheet Lotte Chemical Titan Titanpro PP CopolymerDocument5 pagesSafety Data Sheet Lotte Chemical Titan Titanpro PP Copolymerpaul kevinNo ratings yet
- Department Order No. 13Document7 pagesDepartment Order No. 13Rodolfo Capitan JrNo ratings yet
- Influence of Psychosocial Safety Climate On Occupational Health and Safety A Scoping ReviewDocument13 pagesInfluence of Psychosocial Safety Climate On Occupational Health and Safety A Scoping ReviewIsabela FialhoNo ratings yet
- Basic Regulatory RequirementsDocument13 pagesBasic Regulatory Requirementsarchuw1No ratings yet
- Ra - Riyadh ProjectDocument13 pagesRa - Riyadh ProjectRais BurondkarNo ratings yet
- Kirti ProjectDocument85 pagesKirti Projectamazed4everNo ratings yet
- ANSI - Z358 - 1 - Check ListDocument12 pagesANSI - Z358 - 1 - Check ListLuis Andres Pradenas FuentesNo ratings yet
- Nalco BT-3000 MSDSDocument10 pagesNalco BT-3000 MSDSKathya CrusherNo ratings yet
- WSWP For Hamisa Installation of Lift FramesDocument6 pagesWSWP For Hamisa Installation of Lift FramesVictor Thembinkosi MakhubeleNo ratings yet
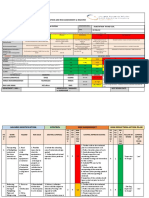
- Activity Title Mill Compound: 1. Hazard Identification 2. Risk Analysis 3.risk ControlDocument8 pagesActivity Title Mill Compound: 1. Hazard Identification 2. Risk Analysis 3.risk ControlizzahNo ratings yet
- BPR 100 80dDocument112 pagesBPR 100 80dBane RadovicNo ratings yet
- Ohnmar Lwin (EMBA - 28)Document90 pagesOhnmar Lwin (EMBA - 28)MinnNo ratings yet
- Biological CleanerDocument13 pagesBiological CleanerArdyas Wisnu BaskoroNo ratings yet
- Construction MethedologyDocument21 pagesConstruction MethedologyRajesh GangwalNo ratings yet
- Royal Plant Workers Vs Coca Cola Bottlers FulltextDocument7 pagesRoyal Plant Workers Vs Coca Cola Bottlers FulltextRowena FelloganNo ratings yet
- Cafco 300 Safety Data SheetDocument2 pagesCafco 300 Safety Data SheetSalman ShaikhNo ratings yet
- HS 019 Control of RecordsDocument13 pagesHS 019 Control of RecordsgrantNo ratings yet
- Scaffold cbc-21st CenturyDocument39 pagesScaffold cbc-21st CenturyAvegail P. Dela CruzNo ratings yet
- Ec Type Examination: Certi FicateDocument5 pagesEc Type Examination: Certi FicateNihilo333No ratings yet
- CAPSTONE RESEARCH GROUP 1 FinalDocument17 pagesCAPSTONE RESEARCH GROUP 1 Finalharrytalaban97No ratings yet
- Altea Accident&Incident Reporting V03Document12 pagesAltea Accident&Incident Reporting V03Abla NedjmaNo ratings yet
- LESSON 5 - Types and Uses of Personal Protective Equipment With Work Sheets and ActivitiesDocument9 pagesLESSON 5 - Types and Uses of Personal Protective Equipment With Work Sheets and ActivitiesIan Jay A. BahiaNo ratings yet
- MSDS 1011712Document11 pagesMSDS 1011712anibal_rios_rivasNo ratings yet
- Su-8 MsdsDocument9 pagesSu-8 MsdsHillary RyanNo ratings yet