You might also like
- Teaching The Student With Special Needs in The Secondary Level Music ClassroomDocument4 pagesTeaching The Student With Special Needs in The Secondary Level Music ClassroomMary ArchuletaNo ratings yet
- Neurology MnemonicsDocument27 pagesNeurology MnemonicsMuhammad Luqman Nul Hakim100% (1)
- Music TherapyDocument44 pagesMusic Therapyjelenaugrinic7039No ratings yet
- Music TherapyDocument18 pagesMusic Therapygenesis129No ratings yet
- The Efficacy of Music For Pain ReliefDocument49 pagesThe Efficacy of Music For Pain ReliefSuharyonoNo ratings yet
- Hearing LossDocument4 pagesHearing LossNobita DoraemonNo ratings yet
- Music Education Philosophy Juli ChiribogaDocument9 pagesMusic Education Philosophy Juli Chiribogaapi-552824615No ratings yet
- Cranial Nerve AssessmentDocument17 pagesCranial Nerve AssessmentMahendran Jayaraman100% (1)
- Science 3 DLP 4 - Parts of Ears and Their FunctionsDocument11 pagesScience 3 DLP 4 - Parts of Ears and Their Functionsmary grace musni100% (1)
- The Impact of Music Therapy On Mental HealthDocument5 pagesThe Impact of Music Therapy On Mental Healthapi-561468026No ratings yet
- Introduction To The Art of Listening To MusicDocument6 pagesIntroduction To The Art of Listening To Musicnefeli123100% (1)
- Journal of Music TherapyDocument88 pagesJournal of Music TherapySafa SolatiNo ratings yet
- Music 2MT3 Test BankDocument13 pagesMusic 2MT3 Test BankSheila KwokNo ratings yet
- Bachelor of Science Music TherapyDocument32 pagesBachelor of Science Music TherapyRodrigo Quiroga de GolemNo ratings yet
- Music Therapy Treatment Summary FinalDocument4 pagesMusic Therapy Treatment Summary Finalapi-294168248No ratings yet
- Ill Sing You A SongDocument18 pagesIll Sing You A Songapi-440383908No ratings yet
- Essential of Music TherapyDocument47 pagesEssential of Music TherapyShairuz Caesar Briones Dugay100% (2)
- Poised in The Creative NowDocument13 pagesPoised in The Creative NowVeri PalladinoNo ratings yet
- Benefits of Using Music Therapy in Mental Disorders 2090 2719 1000116 PDFDocument4 pagesBenefits of Using Music Therapy in Mental Disorders 2090 2719 1000116 PDFPallavi Ghanekar100% (1)
- Contributions of Nordoff-RobbinsDocument210 pagesContributions of Nordoff-Robbinsmarc_corominas_pujadoNo ratings yet
- Coping With Loneliness Through Music PDFDocument4 pagesCoping With Loneliness Through Music PDFJack NiggerNo ratings yet
- Article: Trinity Laban Conservatoire of Music and Dance, UK Institute of Education, University of London, UKDocument17 pagesArticle: Trinity Laban Conservatoire of Music and Dance, UK Institute of Education, University of London, UKFilipe FernandesNo ratings yet
- Manual of Temporal Bone DissectionDocument82 pagesManual of Temporal Bone DissectionBungbu Tn100% (4)
- Essentials of Music Therapy AssessmentDocument643 pagesEssentials of Music Therapy AssessmentWassim JomaaNo ratings yet
- Envisioning The Future of Music TherapyDocument162 pagesEnvisioning The Future of Music TherapyJFF100% (2)
- Patrick J. Willems - Genetic Hearing Loss (2004, Marcel Dekker) PDFDocument500 pagesPatrick J. Willems - Genetic Hearing Loss (2004, Marcel Dekker) PDFCarmen-BadeaNo ratings yet
- Music Education Around The WorldDocument9 pagesMusic Education Around The Worldapi-526605468No ratings yet
- Singing Dialogue - Music Therapy With Persons - PDF RoomDocument360 pagesSinging Dialogue - Music Therapy With Persons - PDF Roomyike TangNo ratings yet
- An Introduction To Music TherapyDocument16 pagesAn Introduction To Music TherapyMarCañellasRuizNo ratings yet
- Music Therapy OutlineDocument4 pagesMusic Therapy OutlineMarylyn Anne AtotNo ratings yet
- Literature Review of Music TherapyDocument6 pagesLiterature Review of Music TherapyKevinNo ratings yet
- Dynamics and Hormonal Mechanisms. Effects of Stress On Immune Cell DistributionDocument18 pagesDynamics and Hormonal Mechanisms. Effects of Stress On Immune Cell DistributionJFFNo ratings yet
- Inner EarDocument18 pagesInner EarSharmela BrijmohanNo ratings yet
- Chapter 11 Sense OrgansDocument18 pagesChapter 11 Sense OrgansMichael Oconnor100% (2)
- Music Is Limitless: A Community Music Therapy Project ProposalDocument47 pagesMusic Is Limitless: A Community Music Therapy Project ProposalCrecer Con la MúsicaNo ratings yet
- Community Music Therapy and Intellectual DisabilityDocument111 pagesCommunity Music Therapy and Intellectual DisabilityTitokNo ratings yet
- MT Music Ed 2006Document4 pagesMT Music Ed 2006Ioan ComanNo ratings yet
- 040 - Human Performance Limitations - QuestionsDocument47 pages040 - Human Performance Limitations - QuestionsEASA ATPL Question Bank75% (4)
- Tplasty Cartilage Slides 080319 PDFDocument46 pagesTplasty Cartilage Slides 080319 PDFasiyazaidiaNo ratings yet
- Music Therapy and MusicMedicineDocument7 pagesMusic Therapy and MusicMedicineAnjuka100% (1)
- Music Therapy For Children With Severe and Profound Multiple Disabilities: A Review of Literature.Document15 pagesMusic Therapy For Children With Severe and Profound Multiple Disabilities: A Review of Literature.logwork81No ratings yet
- Music and EmotionDocument3 pagesMusic and EmotionJulioCesarAlcazarPinilla100% (1)
- Music Therapy For Children Down S PDFDocument8 pagesMusic Therapy For Children Down S PDFRaul Alejandro Celis MaturanaNo ratings yet
- What Is Music TherapyDocument20 pagesWhat Is Music Therapyeve sthNo ratings yet
- Adam Rouilly Ear - SlidesDocument5 pagesAdam Rouilly Ear - Slidesih8bart100% (2)
- Otitis MediaDocument14 pagesOtitis MediaMelissa DavidNo ratings yet
- Music Centered Music Therapy 1nbsped 9781891278891 9781891278259Document388 pagesMusic Centered Music Therapy 1nbsped 9781891278891 9781891278259M sNo ratings yet
- Felicity Baker Music Therapy SongwritingDocument15 pagesFelicity Baker Music Therapy SongwritingSam CrowNo ratings yet
- Music Therapy ProposalDocument4 pagesMusic Therapy ProposalSandley Majan Sabang50% (2)
- The Way Music Influences Our Mentality 1Document15 pagesThe Way Music Influences Our Mentality 1api-607979922100% (1)
- Significant Moments in Music Therapy 2005Document23 pagesSignificant Moments in Music Therapy 2005Tomas SærmarkNo ratings yet
- History of Music TherapyDocument4 pagesHistory of Music TherapyJonathan Malimban PrietoNo ratings yet
- Senior Project Paper-5Document10 pagesSenior Project Paper-5api-409933006No ratings yet
- Juslin, P. N., & Vastfjall, D. (2008) - Emotional Responses To Music - The Need To Consider Underlying Mechanisms. Behavioral and Brain Sciences, 31 (5), 559.Document63 pagesJuslin, P. N., & Vastfjall, D. (2008) - Emotional Responses To Music - The Need To Consider Underlying Mechanisms. Behavioral and Brain Sciences, 31 (5), 559.goni56509No ratings yet
- Awit Bulilit Choir Competition 2019 Mechanics (7!26!19)Document4 pagesAwit Bulilit Choir Competition 2019 Mechanics (7!26!19)Millie LagonillaNo ratings yet
- Synthesis Paper On The Use of Hip-Hop and Rap Music in Music TherapyDocument9 pagesSynthesis Paper On The Use of Hip-Hop and Rap Music in Music TherapyJosh kuhlNo ratings yet
- Basic Vocal Pedagogy For Amateur SingersDocument42 pagesBasic Vocal Pedagogy For Amateur SingersDixie LacuestaNo ratings yet
- Music Therapy in Education LeafletDocument1 pageMusic Therapy in Education Leafletjelenaugrinic7039No ratings yet
- Music Therapy ResearchDocument2 pagesMusic Therapy ResearchDanielle LewisNo ratings yet
- Tanner Growth StudyDocument13 pagesTanner Growth StudyBen BurlinsonNo ratings yet
- Music Therapy Today (Magazin) : Therapeutic Usefulness of Music - Volume VII, Issue 1 (March 2006)Document289 pagesMusic Therapy Today (Magazin) : Therapeutic Usefulness of Music - Volume VII, Issue 1 (March 2006)ElJay AremNo ratings yet
- Where Is ThumbkinDocument1 pageWhere Is ThumbkinHelen Meriz SagunNo ratings yet
- Music and Medicine The Affect of Music On The Human BeingDocument10 pagesMusic and Medicine The Affect of Music On The Human BeingTariq J FaridiNo ratings yet
- Music of The PhilippinesDocument19 pagesMusic of The PhilippinesLjose P ZantuaNo ratings yet
- ALDRIDGE, NEUGEBAUER AND GUSTORFF - A Preliminary Study of Creative Music Therapy in The Treatment of Children With Developmental DelayDocument17 pagesALDRIDGE, NEUGEBAUER AND GUSTORFF - A Preliminary Study of Creative Music Therapy in The Treatment of Children With Developmental DelayCamila Rocha FerrariNo ratings yet
- Annotated Bibliography - Music EvolutionDocument7 pagesAnnotated Bibliography - Music EvolutionAndrew MajorNo ratings yet
- Music 2MT3 Quizzes 2019 WITHOUT Answers Quiz 1Document11 pagesMusic 2MT3 Quizzes 2019 WITHOUT Answers Quiz 1Sheila KwokNo ratings yet
- Chapter 9. The Use of Group Vocal Improvisation As A Music Therapy Technique in A Mental Health SettingDocument10 pagesChapter 9. The Use of Group Vocal Improvisation As A Music Therapy Technique in A Mental Health SettingEmilia Hamerlik100% (1)
- The Effects of Music Therapy For Older People With PDFDocument7 pagesThe Effects of Music Therapy For Older People With PDFJenny MaulidyaNo ratings yet
- Music Therapy and Mental Health PDFDocument2 pagesMusic Therapy and Mental Health PDFBianca DineaNo ratings yet
- The Role of Play in Music Education For Young ChildrenDocument35 pagesThe Role of Play in Music Education For Young ChildrenalbacaminsNo ratings yet
- Orff Schulwerk: Visited: April, 6th, 10.38amDocument6 pagesOrff Schulwerk: Visited: April, 6th, 10.38amVíctorNo ratings yet
- Physiological Effects of Music Therapy 2Document7 pagesPhysiological Effects of Music Therapy 2api-745276865No ratings yet
- Moylan 2007Document19 pagesMoylan 2007JFFNo ratings yet
- Internet Survival Guide - 2016Document489 pagesInternet Survival Guide - 2016chinNo ratings yet
- Attachment and Psychosomatic Medicine: Developmental Contributions To Stress and DiseaseDocument12 pagesAttachment and Psychosomatic Medicine: Developmental Contributions To Stress and DiseaseJFFNo ratings yet
- Anderson 2002Document14 pagesAnderson 2002JFFNo ratings yet
- Ref 190Document10 pagesRef 190JFFNo ratings yet
- Neuropsychological Function in Children With Maltreatment-Related Posttraumatic Stress DisorderDocument4 pagesNeuropsychological Function in Children With Maltreatment-Related Posttraumatic Stress DisorderJFFNo ratings yet
- Caffeine Can Decrease Subjective Energy Depending On The Vehicle With Which It Is Consumed and When It Is MeasuredDocument13 pagesCaffeine Can Decrease Subjective Energy Depending On The Vehicle With Which It Is Consumed and When It Is MeasuredJFFNo ratings yet
- Art CaffeineDocument12 pagesArt CaffeineJFFNo ratings yet
- Invited Review The Links Between Stress and Illness: Andrew SteptoeDocument12 pagesInvited Review The Links Between Stress and Illness: Andrew SteptoeJFFNo ratings yet
- Vocabulary of Our Senses PDFDocument3 pagesVocabulary of Our Senses PDFDavid EcheverriaNo ratings yet
- DAFTAR PUSTAKA Presbikusis Yeni WidayantiDocument3 pagesDAFTAR PUSTAKA Presbikusis Yeni WidayantiYeni WidayantiNo ratings yet
- Rad UMR0777491 4020126 1701Document4 pagesRad UMR0777491 4020126 1701sureshmaila9966No ratings yet
- Compilation of Sharir Kriya Vigyan On KARNA EARDocument52 pagesCompilation of Sharir Kriya Vigyan On KARNA EARBijay GhimireNo ratings yet
- Neural Control & Coordination PowernotesDocument2 pagesNeural Control & Coordination PowernotesSushmit Srivastava100% (1)
- filePV 27 05 377Document9 pagesfilePV 27 05 377pifmanNo ratings yet
- The Minds Machine Foundations of Brain and Behavior 4Th Edition Neil Verne Watson Full ChapterDocument63 pagesThe Minds Machine Foundations of Brain and Behavior 4Th Edition Neil Verne Watson Full Chapterjames.keeter432100% (12)
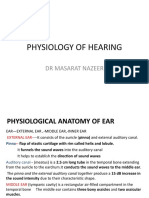
- Physiology of Hearing: DR Masarat NazeerDocument12 pagesPhysiology of Hearing: DR Masarat NazeerMusarrat NazeerNo ratings yet
- Retraction Pocket and CholesteatomaDocument22 pagesRetraction Pocket and CholesteatomaYasar KhanNo ratings yet
- Cochlear Implants Are Miraculous and Maddening - BloombergDocument6 pagesCochlear Implants Are Miraculous and Maddening - BloombergParker KohlNo ratings yet
- CH 09 09Document13 pagesCH 09 09ssoeliauwanNo ratings yet
- Audio Visual Entrainment AVEDocument17 pagesAudio Visual Entrainment AVEoscarnineNo ratings yet
- Open Access Atlas of Otolaryngology, Head & Neck Operative SurgeryDocument3 pagesOpen Access Atlas of Otolaryngology, Head & Neck Operative SurgeryMiggy GNo ratings yet
- (ENT) 1.04 Problems of Inner Ear 1 - Calavera (Aug 24)Document11 pages(ENT) 1.04 Problems of Inner Ear 1 - Calavera (Aug 24)Noreen Hannah GabrielNo ratings yet
- Inventis, AudiometerDocument11 pagesInventis, Audiometerfarmasi rajalNo ratings yet
- Part Number 2205-0100 Rev BDocument79 pagesPart Number 2205-0100 Rev BWilliamDLVNo ratings yet
- Tinnitus Today December 1998 Vol 23, No 4Document29 pagesTinnitus Today December 1998 Vol 23, No 4American Tinnitus AssociationNo ratings yet
- Suharyono Stikes Rs Baptis KediriDocument69 pagesSuharyono Stikes Rs Baptis KediriDhea LaksonoNo ratings yet