You might also like
- Administration ManualDocument18 pagesAdministration ManualMOKSH SHREE THAKURNo ratings yet
- NLADocument11 pagesNLAPedro CardosoNo ratings yet
- Probation Appraisal FormDocument3 pagesProbation Appraisal Formbook xpert1No ratings yet
- TOEFL Speaking RubricsDocument2 pagesTOEFL Speaking RubricsApoorv MahajanNo ratings yet
- Personnel RequisitionDocument2 pagesPersonnel RequisitionAgam Syahrul KhalifianiNo ratings yet
- JD PDFDocument89 pagesJD PDFapjbalamuruganNo ratings yet
- Human Resource (HR) Policies and ProceduresDocument4 pagesHuman Resource (HR) Policies and ProceduresDanish NawazNo ratings yet
- Code of Conduct Policy: Med Plus Group of CompaniesDocument12 pagesCode of Conduct Policy: Med Plus Group of CompanieskishoreNo ratings yet
- Hydrology Principles Analysis DesignDocument477 pagesHydrology Principles Analysis DesignCarel De Jager82% (17)
- Leave Application Form (New)Document1 pageLeave Application Form (New)GGC BroadbandNo ratings yet
- HR Policy: 1. General 1.1 Short Title, Extent and CommencementDocument12 pagesHR Policy: 1. General 1.1 Short Title, Extent and Commencementskywalk buildersNo ratings yet
- Turn-Over of Responsibilities Checklist PDFDocument1 pageTurn-Over of Responsibilities Checklist PDFJenn TanNo ratings yet
- Manpower Request Form FinalDocument1 pageManpower Request Form Finalkomal janiNo ratings yet
- Clearance Form: Ahamed Aslam 0358/107499 Engineering/HCNS 11.11.2016 29135618448 Mechanical EngineerDocument1 pageClearance Form: Ahamed Aslam 0358/107499 Engineering/HCNS 11.11.2016 29135618448 Mechanical EngineerAslamNo ratings yet
- Employee Final SettlementDocument1 pageEmployee Final SettlementZeeshan Mirza50% (2)
- HR Employee Clearance FormDocument3 pagesHR Employee Clearance FormRichard R M ThodéNo ratings yet
- All Visa InterviewDocument30 pagesAll Visa InterviewApoorv Mahajan100% (2)
- Requisition FormDocument1 pageRequisition FormAdnan AzharNo ratings yet
- Payroll Deduction FormDocument1 pagePayroll Deduction FormIoaneRNo ratings yet
- Reference Checking FormDocument3 pagesReference Checking FormEnza R100% (1)
- Leave Application Form-2Document4 pagesLeave Application Form-2api-3741191No ratings yet
- Application For Employment: Personal DataDocument2 pagesApplication For Employment: Personal DataAntoinette PerezNo ratings yet
- Training Requisition FormatDocument1 pageTraining Requisition FormatSGNo ratings yet
- Exit FormDocument2 pagesExit FormLucy Anajwala100% (1)
- Manpower Requisition (Project Cordinator-HQ)Document2 pagesManpower Requisition (Project Cordinator-HQ)ruhul01No ratings yet
- Training PolicyDocument6 pagesTraining Policygaza222No ratings yet
- Strategic Total Reward 20210710T091532Document8 pagesStrategic Total Reward 20210710T091532Loice WanjalaNo ratings yet
- AustralianGeomechanicsLLPLpaper38 2 5Document7 pagesAustralianGeomechanicsLLPLpaper38 2 5Apoorv MahajanNo ratings yet
- Internship Offer Letter Bin Younas TemplateDocument2 pagesInternship Offer Letter Bin Younas TemplateUsman Bin Younas100% (1)
- Revise Ob FormDocument1 pageRevise Ob FormJake MadzNo ratings yet
- Exit Interview FormDocument2 pagesExit Interview FormmtcadslpalingcastreNo ratings yet
- RTMSI - Personnel Movement FormDocument1 pageRTMSI - Personnel Movement FormShereen AbbangöNo ratings yet
- Staff Vetting TemplateDocument1 pageStaff Vetting Templateney issaNo ratings yet
- Asset Disposal Form: A) To Be Completed by Department Head/Division HeadDocument2 pagesAsset Disposal Form: A) To Be Completed by Department Head/Division HeadPotchara KulNo ratings yet
- Annual Training Calender Eti 12Document1 pageAnnual Training Calender Eti 12anand shankarNo ratings yet
- Employee Status Change: Type of Change Current Information New InformationDocument2 pagesEmployee Status Change: Type of Change Current Information New InformationTara GreskoviakNo ratings yet
- Accident Investgation Fom 632Document5 pagesAccident Investgation Fom 632emeka2012No ratings yet
- Advance Cash Request FormDocument1 pageAdvance Cash Request FormTanesh SelvarajuNo ratings yet
- Paf FormDocument4 pagesPaf FormFauzi LyandaNo ratings yet
- BVLGARI Recruitment Reference Check Form-MgrDocument3 pagesBVLGARI Recruitment Reference Check Form-MgrChristian ReyesNo ratings yet
- HR Position Requisition FormDocument1 pageHR Position Requisition FormRichard R M ThodéNo ratings yet
- Entertainment FORMDocument2 pagesEntertainment FORMAchmad NabihNo ratings yet
- Status Change FormDocument1 pageStatus Change FormComsale HRNo ratings yet
- Revised Hours of Work Policy 071021Document19 pagesRevised Hours of Work Policy 071021Faridatul MelurNo ratings yet
- Employee Movement Form.v01 - Recg - Mohamed Adam Izhar Bin Mohamed RidzwanDocument1 pageEmployee Movement Form.v01 - Recg - Mohamed Adam Izhar Bin Mohamed RidzwanXiao Minn NeohNo ratings yet
- Project Report SampleDocument118 pagesProject Report SampleaadishNo ratings yet
- Chapter 16 MotivationDocument10 pagesChapter 16 MotivationKhánh Linh PhạmNo ratings yet
- Background Check FormDocument2 pagesBackground Check FormIrish PallesNo ratings yet
- Rejoining Form: INSTRUCTION: When Employee Returns From Annual Leave, Emergency Leave, Official Business Trip or Not AsDocument1 pageRejoining Form: INSTRUCTION: When Employee Returns From Annual Leave, Emergency Leave, Official Business Trip or Not Assameh100% (1)
- Clearance Form (To Be Completed Before Leaving)Document2 pagesClearance Form (To Be Completed Before Leaving)Tafadzwa Edson PasiNo ratings yet
- 01H - Duty Resumption Form (Rev.01)Document1 page01H - Duty Resumption Form (Rev.01)AslamNo ratings yet
- 11 Employees Transfer Request FormDocument1 page11 Employees Transfer Request FormsekarNo ratings yet
- Rules and Regulations For All International HousesDocument3 pagesRules and Regulations For All International HousesHenryy555No ratings yet
- Manpower Request Form (MRF) : HRM-OO1-0Document1 pageManpower Request Form (MRF) : HRM-OO1-0Irvin Baltazar SamaniegoNo ratings yet
- Employee Transfer Form ExampleDocument1 pageEmployee Transfer Form ExampleMahendra KumaraNo ratings yet
- Employee Record Form: Employee'S Passport PhotographDocument3 pagesEmployee Record Form: Employee'S Passport PhotographRicksonNo ratings yet
- Employee Absence Reporting RulesDocument3 pagesEmployee Absence Reporting RulesFrancisco RamirezNo ratings yet
- Sample Reference Check QuestionsDocument2 pagesSample Reference Check QuestionsImeeNo ratings yet
- HRD20 - Inter Hotel Staff Transfer FormDocument1 pageHRD20 - Inter Hotel Staff Transfer FormCyber BiteNo ratings yet
- Withdrawal of Job OfferDocument1 pageWithdrawal of Job OfferJohn Sowp MacTavishNo ratings yet
- Medical DR - PCMO Job Announcement Peace CorpsDocument2 pagesMedical DR - PCMO Job Announcement Peace CorpsU.s. Africa CommandNo ratings yet
- Office AssignmentDocument1 pageOffice AssignmentlintangNo ratings yet
- Prize Redemption FormDocument1 pagePrize Redemption FormRahul GuptaNo ratings yet
- Application For EmploymentDocument3 pagesApplication For EmploymentBente OtsoNo ratings yet
- Employee Requisition: A. Superior DetailDocument4 pagesEmployee Requisition: A. Superior DetaillintangNo ratings yet
- Background Check FormDocument1 pageBackground Check FormJheallaine Andrea dela Peña-ChuaNo ratings yet
- Business Entertainment FormDocument1 pageBusiness Entertainment FormRichard Zaw100% (1)
- Leave Request Form R 170425Document1 pageLeave Request Form R 170425rbp9m9zz7rNo ratings yet
- Recruiter Name: Infinite Dragon Life Insurance AgencyDocument17 pagesRecruiter Name: Infinite Dragon Life Insurance Agencybob huli ngalanNo ratings yet
- NS Concrete Report (Trial Mix M-50)Document4 pagesNS Concrete Report (Trial Mix M-50)Apoorv MahajanNo ratings yet
- Heaven Engineers & Contractors Pvt. LTD.: 128, Pocket-14, Sector-20, Rohini, New Delhi-110085Document1 pageHeaven Engineers & Contractors Pvt. LTD.: 128, Pocket-14, Sector-20, Rohini, New Delhi-110085Apoorv MahajanNo ratings yet
- Hydrocell XL: High Performance, Cross Linked, Closed Cell, Non-Absorbent, Polyethylene Joint Fi LlerDocument2 pagesHydrocell XL: High Performance, Cross Linked, Closed Cell, Non-Absorbent, Polyethylene Joint Fi LlerApoorv MahajanNo ratings yet
- Government of India Central Public Works Department Office of Executive Engineer, Ajmer Central Division, Ajmer (Rajasthan)Document76 pagesGovernment of India Central Public Works Department Office of Executive Engineer, Ajmer Central Division, Ajmer (Rajasthan)Apoorv MahajanNo ratings yet
- Acoustimax Non-Woven Solutions For Acoustic ManagementDocument4 pagesAcoustimax Non-Woven Solutions For Acoustic ManagementApoorv MahajanNo ratings yet
- 001-MoEF Approval With Gazette NotificationDocument3 pages001-MoEF Approval With Gazette NotificationApoorv MahajanNo ratings yet
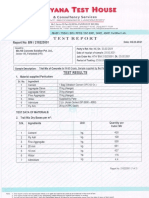
- Conforming To The Acceptable LimitsDocument1 pageConforming To The Acceptable LimitsApoorv MahajanNo ratings yet
- Safe N Silent Data Sheet inDocument2 pagesSafe N Silent Data Sheet inApoorv MahajanNo ratings yet
- Recommended Order of ReadingDocument1 pageRecommended Order of ReadingApoorv MahajanNo ratings yet
- Incoming Material DetailDocument15 pagesIncoming Material DetailApoorv MahajanNo ratings yet
- Struct Steel - STD WtsDocument3 pagesStruct Steel - STD WtsnayabaaNo ratings yet
- Analysis of SeabiscuitDocument47 pagesAnalysis of SeabiscuitApoorv MahajanNo ratings yet
- C E Career GuideDocument17 pagesC E Career GuideApoorv MahajanNo ratings yet
- Education System - India: 1. Transcripts That Only Show Subject MarksDocument6 pagesEducation System - India: 1. Transcripts That Only Show Subject MarksApoorv MahajanNo ratings yet
- FlamingoDocument23 pagesFlamingoApoorv MahajanNo ratings yet
- Buong Paper NG Research FINALDocument167 pagesBuong Paper NG Research FINALJemarita EspidolNo ratings yet
- Megatrend Outputs: GBM: Human Resource Management 2022KDocument8 pagesMegatrend Outputs: GBM: Human Resource Management 2022KMohammad KamruzzamanNo ratings yet
- Phil. Employ Services and Resources, Inc. vs. Joseph Paramio, Et. AlDocument5 pagesPhil. Employ Services and Resources, Inc. vs. Joseph Paramio, Et. AlDanny FentomNo ratings yet
- Shrudi Nadar BlackbookDocument35 pagesShrudi Nadar Blackbookravina bhuvadNo ratings yet
- Chapter 10Document5 pagesChapter 10여자라라No ratings yet
- Employee Training: Facility Name: NPDES Permit NumberDocument2 pagesEmployee Training: Facility Name: NPDES Permit NumbersubhanmusadiqNo ratings yet
- CENG-6104 Organization and Labor Managment Group AssignmentDocument14 pagesCENG-6104 Organization and Labor Managment Group AssignmentAndu TadesseNo ratings yet
- Netflix HR Policies CaseDocument5 pagesNetflix HR Policies CaseArpit NaruNo ratings yet
- Human Resource Management at TCS LTDDocument30 pagesHuman Resource Management at TCS LTDNirmal NairNo ratings yet
- Test Bank For Employment Law 6th Edition MoranDocument4 pagesTest Bank For Employment Law 6th Edition MoranPhillipRamirezezkyc100% (84)
- USPS Response To Congressman Dutch RuppersbergerDocument3 pagesUSPS Response To Congressman Dutch RuppersbergerMallory SofastaiiNo ratings yet
- Bangladesh University of Professionals (BUP)Document3 pagesBangladesh University of Professionals (BUP)Naznin AkterNo ratings yet
- Pengurusan Sumber Manusia Antarabangsa: ArticleDocument12 pagesPengurusan Sumber Manusia Antarabangsa: ArticleNURSYAMIMI BINTI AB WAHAB -No ratings yet
- Pathao (Ob)Document13 pagesPathao (Ob)Tamim Rahman100% (1)
- HRMG Unit-4Document8 pagesHRMG Unit-4rakshit konchadaNo ratings yet
- What Is HR ConsultingDocument2 pagesWhat Is HR ConsultingRustashNo ratings yet
- Talent Management: Proprietary Content. ©great Learning. All Rights Reserved. Unauthorized Use or Distribution ProhibitedDocument29 pagesTalent Management: Proprietary Content. ©great Learning. All Rights Reserved. Unauthorized Use or Distribution ProhibitedCorpsalesNo ratings yet
- Employer Reference LetterDocument7 pagesEmployer Reference Letterafiwhyqrv100% (2)
- Management Style: Prepared By: John Kayle BorjaDocument12 pagesManagement Style: Prepared By: John Kayle BorjaJohn Kayle BorjaNo ratings yet
- Employee HR Policies in Hospitality Industries: (With Special Refrence To OYO)Document60 pagesEmployee HR Policies in Hospitality Industries: (With Special Refrence To OYO)ANKIT saran saran jat100% (2)
- Nile Siddiqui PrintDocument52 pagesNile Siddiqui PrintAyesh Zaman SiddiquiNo ratings yet
- Arghya Sengupta: ObjectiveDocument2 pagesArghya Sengupta: ObjectiveHRD CORP CONSULTANCYNo ratings yet
- Case Incident ExampleDocument2 pagesCase Incident ExampleLika ChanturiaNo ratings yet
- Performance Management: DR Kwesi Atta Sakyi, ZcasDocument14 pagesPerformance Management: DR Kwesi Atta Sakyi, ZcasEdson MungaNo ratings yet
- HRM Finals ExamDocument3 pagesHRM Finals ExamJay Val techNo ratings yet