You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- WordPress SEO ChecklistDocument7 pagesWordPress SEO ChecklistTLC for Coaches100% (2)
- Lab Report 5Document7 pagesLab Report 5enieynazNo ratings yet
- LABSHEET-1 Introduction To The Wireshark and Analysis of A Given Set of ProtocolsDocument13 pagesLABSHEET-1 Introduction To The Wireshark and Analysis of A Given Set of ProtocolsAnupama InturiNo ratings yet
- RedddDocument123 pagesRedddKarthik RajuNo ratings yet
- Gas Dynamics and Jet PropulsionDocument315 pagesGas Dynamics and Jet PropulsionSuresh BiradarNo ratings yet
- Accomplishment Clubs ProjectDocument3 pagesAccomplishment Clubs Projectshai24No ratings yet
- Farnaz Thesis PDFDocument145 pagesFarnaz Thesis PDFnurdin_sumantriNo ratings yet
- Exercise Chapter 1 Maps and Globes PDFDocument5 pagesExercise Chapter 1 Maps and Globes PDFSuvashreePradhan100% (1)
- Vector CANoeDocument7 pagesVector CANoeZaferNo ratings yet
- Emerson DeltaV Networking WhitepaperDocument7 pagesEmerson DeltaV Networking WhitepaperAnonymous qiAIfBHnNo ratings yet
- Drives: AC Inverters Sensorless Vector Closed Loop Vector Servo Drives DC Drives MotorsDocument44 pagesDrives: AC Inverters Sensorless Vector Closed Loop Vector Servo Drives DC Drives Motorsjohxav10No ratings yet
- Bolt Load Software: ANSI B16.5 Api 6A Api 17Sv Norsok L-005 SPO Compact Flanges Taperlok FlangesDocument2 pagesBolt Load Software: ANSI B16.5 Api 6A Api 17Sv Norsok L-005 SPO Compact Flanges Taperlok Flangesloveanbu24No ratings yet
- HistoryDocument1 pageHistoryRaymond BaroneNo ratings yet
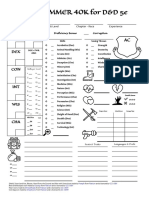
- WARHAMMER 40K For D&D 5e: Character Name Class & Level Chapter - Race ExperienceDocument1 pageWARHAMMER 40K For D&D 5e: Character Name Class & Level Chapter - Race ExperienceJacob CooperNo ratings yet
- Empirical Analysis On Employee Relationship Management at Software Companies With Special Reference To Chennai City.Document16 pagesEmpirical Analysis On Employee Relationship Management at Software Companies With Special Reference To Chennai City.CHEIF EDITORNo ratings yet
- Library Management System - RudrahariDocument62 pagesLibrary Management System - RudrahariNitesh Bhura100% (4)
- Helping Kids Develop Conflict Resolution SkillsDocument3 pagesHelping Kids Develop Conflict Resolution SkillsDiya MariaNo ratings yet
- Dot Painting RubricDocument1 pageDot Painting Rubricapi-312657832No ratings yet
- Comparison and ContrastDocument9 pagesComparison and ContrastCrash BandicootNo ratings yet
- Template For JournalDocument2 pagesTemplate For JournalNastarres SoulmatesNo ratings yet
- Verification OverviewDocument123 pagesVerification OverviewSamNo ratings yet
- PhdThesis SheffieldDocument202 pagesPhdThesis SheffieldDebasisMohapatraNo ratings yet
- New Employee Orientation Program Checklist 1Document3 pagesNew Employee Orientation Program Checklist 1Ai LeenNo ratings yet
- RPMS Porfolio Template (Long)Document17 pagesRPMS Porfolio Template (Long)MarifeNo ratings yet
- Cool New Features in Python 3Document3 pagesCool New Features in Python 3DEEP725No ratings yet
- Killzone Rules v3Document25 pagesKillzone Rules v3dracomaxisNo ratings yet
- TVL Illustration Week 4Document15 pagesTVL Illustration Week 4Victor Moraca Sinangote0% (1)
- Amazon Has Just Shown Off The Most Advanced Technology StoreDocument3 pagesAmazon Has Just Shown Off The Most Advanced Technology StoreEmanuel VasconcelosNo ratings yet
- Solomon y Corbit - 1978 - An Opponent-Process Theory of MotivationDocument14 pagesSolomon y Corbit - 1978 - An Opponent-Process Theory of Motivationmario_garcés_4No ratings yet
- 11 Anh INTENSIVE LISTENING LESSON 01.12Document2 pages11 Anh INTENSIVE LISTENING LESSON 01.12Ha Huy KhanhNo ratings yet