Professional Documents
Culture Documents
Jurnal Rad1
Uploaded by
Sandy MurtiningtyasOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Jurnal Rad1
Uploaded by
Sandy MurtiningtyasCopyright:
Available Formats
Wo m e n s I m a g i n g O r i g i n a l R e s e a r c h
Reisenauer et al.
Ultrasound-Guided Breast Interventions
Womens Imaging
Original Research
JOURNAL CLUB:
Downloaded from www.ajronline.org by Fudan University Library on 02/23/17 from IP address 61.129.42.15. Copyright ARRS. For personal use only; all rights reserved
Ultrasound-Guided Breast
Interventions: Low Incidence of
Infectious Complications With
JOURNA L CLUB Useof an Uncovered Probe
Chris Reisenauer 1 OBJECTIVE. The purpose of this study was to determine the incidence of infectious
Robert T. Fazzio complications after ultrasound-guided breast interventions performed with an intermediate-
Gina Hesley level disinfection protocol without an ultrasound probe cover.
MATERIALS AND METHODS. Two independent institutional databases were
Reisenauer C, Fazzio RT, Hesley G searched to identify breast infections in patients who underwent ultrasound-guided interven-
tions between January 2005 and July 2013. The departments of radiology and infectious dis-
eases independently maintained these databases. A comprehensive retrospective chart review
based on periprocedural antibiotic use and clinical documentation of infection was also per-
formed to reduce the likelihood of missing potential infectious complications.
RESULTS. A total of 12,708 ultrasound-guided breast procedures were performed in the
time frame of this study. All potential cases of procedure-related infection were included for
subspecialist review in an effort to give the most conservative (highest) estimate of infectious
complications. Among these cases, 14 documented cases of possible procedure-related infec-
tion were identified, for an overall incidence of 0.11%. All infections were localized skin or
soft-tissue infections and adequately treated with a short course of oral antibiotics. No cases
of more serious infections or sepsis were found. None of the reported infections required IV
antibiotic therapy, percutaneous intervention, surgical intervention, or hospitalization.
CONCLUSION. The incidence of infectious complications after an ultrasound-guided
breast intervention without an ultrasound probe cover is extremely low. Physicians can use
this information in the development of their disinfection protocols and to provide accurate in-
formation in counseling patients during preprocedural consultation.
ltrasound-guided interventionhas tion without specific attention to biopsy mo-
U become a primary tool in the di-
agnostic workup of breast lesions
[110]. The technique for per-
dality, disinfection protocol, or use of a probe
cover ranges from 0% [1, 3, 69] to 0.12% [5].
The largest cohort in a multiinstitutional study
forming a successful ultrasound-guided included 3765 patients who underwent both
Keywords: biopsy, breast, infection, procedure, ultrasound
breast biopsy has been thoroughly described percutaneous stereotactic and ultrasound-
in the literature [1113]. These interventions guided breast biopsies with a reported infec-
DOI:10.2214/AJR.16.16440 are safe, effective, and accurate owing to the tious complication rate of 0.08% [1].
lack of ionizing radiation and dynamic visu- Our institution proposed escalation of ul-
Received March 6, 2016; accepted after revision
alization capabilities. A large body of publi- trasound probe disinfection for breast inter-
November 12, 2016.
cations have documented the techniques and ventions to a high-level disinfection proto-
Based on a presentation at the Radiological Society of complications of continually evolving ultra- col and use of a probe cover in an effort to
North America 2015 annual meeting, Chicago, IL. sound-guided breast interventions for diag- standardize institutional practices. This pro-
1
nostic purposes [110]. posed practice change would have increased
All authors: Department of Radiology, Mayo Clinic
Minnesota, 200 1st St SW, Rochester, MN 55905.
Although infectious complications of cost and procedure quality control time with-
Address correspondence to G. Helsey breast procedures have been studied [18, 14], out a definite benefit to patient safety. There-
(helsey.gina@mayo.edu) we are unaware of a single large-scale study of fore, we conducted a large-scale review using
the incidence of infectious complications af- prospective and retrospective data to deter-
AJR 2017; 208:17 ter ultrasound-guided breast procedures spe- mine the types and incidence of infectious
0361803X/17/20851
cifically performed with an intermediate-lev- complications in an effort to provide infor-
el disinfection protocol without an ultrasound mation about the efficacy of intermediate-
American Roentgen Ray Society probe cover. The reported incidence of infec- level disinfection without a probe cover and
AJR:208, May 2017 1
Reisenauer et al.
accurate infectious risk estimation to pa- small or complex cystic lesions. A small number of wipe for 5 minutes before use in a procedure. Af-
tients undergoing ultrasound-guided proce- biopsies were performed with a Neothermia device ter the procedure, visible soiling was wiped from
dures. The study was descriptive, and we did (Intact Medical Corporation), which is an 8-gauge the transducer with a dry disposable towel, and
not attempt to identify underlying risk fac- device that entails use of radiofrequency technol- the transducer was cleaned with a sanitizing wipe
tors for infectious complications. ogy to obtain a surgical-quality specimen for his- and wrapped with a sanitizing wipe to ensure the
Downloaded from www.ajronline.org by Fudan University Library on 02/23/17 from IP address 61.129.42.15. Copyright ARRS. For personal use only; all rights reserved
tologic analysis and margin assessment. Aspira- transducer stayed wet for the necessary wet con-
Materials and Methods tions were performed with sterile needles ranging tact time of 5 minutes. All procedures were per-
Patients from 16- to 25-gauge. Of the 12,708 procedures, formed without an ultrasound probe cover.
We performed 12,708 ultrasound-guided breast 9415 were core needle or vacuum-assisted biop-
procedure events for 9066 patients over the 8-year sies; the other 3293 procedures were needle aspira- Identification of Positive Cases
7-month period January 2005 through July 2013. tions. Most of the biopsies were performed with- With institutional review board approval, we
In this study time frame, 755 patients declined out an introducer needle. The average number of reviewed medical records from January 2005 to
authorization to use their medical records for re- passes for a biopsy or fine-needle aspiration was July 2013 using infectious disease and radiology
search and were excluded from analysis. Proce- approximately five. The biopsy site was routine- department databases and algorithm-directed ret-
dure events were defined as a single diagnostic ly marked with a titanium, stainless steel, or ce- rospective chart review. The infection prevention
or therapeutic session, which may have includ- ramic clip immediately after the procedure. After and control (IPC) committee at our institution con-
ed more than one procedure site. For example, a the biopsy, a procedural assistant immediately ap- ducts prospective surveillance for selected positive
small minority of patients underwent multisite bi- plied firm pressure for 510 minutes in effort to specimen culture results, including those of patients
opsies in a single session because they had syn- achieve hemostasis and prevent hematoma devel- who have undergone radiology procedures. Culture
chronous suspicious lesions, and each biopsy site opment. Standardized postprocedural care instruc- specimens are obtained by the primary physician
was reported in a single dictation. Consequently, tions were provided to the patient. These instruc- on the basis of clinical findings, laboratory data, or
multisite interventions in a single session were tions included intermittent cold pack application concern for infection. In addition to reviewing cul-
dictated in a combined report in our archiving sys- for 2 hours, nonaspirin pain reliever as needed, ture data, the IPC committee prospectively moni-
tem and referred to as a single procedure event. avoidance of submerging the area for 24 hours, tors daily surgical lists and daily hospital admission
All patients who underwent an ultrasound-guided and avoiding strenuous activity or lifting anything data for visits to the hospital or operating room for
procedure were included in the search parameters. heavier than 10 pounds (4.5 kg) for 24 hours. the treatment of infection. When a case is identified
Patients who underwent surgical intervention af- The ultrasound transducer preparation and with either of these methods, an infection control
ter an ultrasound-guided procedure were excluded disinfection process evolved over the time frame practitioner thoroughly reviews the patients elec-
from the study only after their surgical dates. of our study. Before 2011, the transducer was tronic records with a specific interest in any pre-
cleansed with povidone-iodine (Betadine, Purdue ceding intervention. An infection control physician
Procedures and Techniques Products) before the procedure and then soaked then reviews the case and decides whether the in-
The procedures performed included ultra- with a disposable towel treated with quaternary fection can be attributed to the procedure on the ba-
sound-guided biopsies and aspirations. Sono- ammonium chloride disinfectant (HB Quat, 3M) sis of the procedure timing, clinical circumstances,
graphic guidance was achieved with a Philips and wrapped for approximately 5 minutes after and additional pertinent data.
Healthcare IU22 unit. Both L17-5 and L12-5 the procedure. From 2011 to July 2013, the trans- Like the IPC committee, the department of ra-
Philips Healthcare transducers were used; the ducer was cleansed with a sanitizing wipe (iso- diology prospectively evaluated all patients who
L12-5 transducer was used for most of the proce- propanol and quaternary ammonium compounds, had undergone ultrasound-guided breast proce-
dures. Prepackaged sterile biopsy kits were used. Sani-Cloth Plus, Professional Disposables In- dures to monitor for complications from 2002
The main contents included a sterile applicator ternational) to remove any debris. The trans- to 2011. This task was performed by a radiology
preparation, a number 11 scalpel, needles, nee- ducer was then wrapped with a clean sanitizing nurse who placed a telephone call to the patient
dle counter, all-purpose sponges, and an adhesive
bandage. Sterile towels were placed around the in-
terventional field. Sterile single-packet ultrasound
gel was used. Approximately 10 mL of lidocaine
with or without a bicarbonate buffer was used for
local anesthesia. Epinephrine was not mixed with
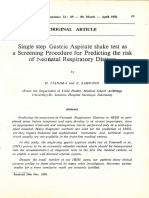
the lidocaine. All procedures were performed by
radiologists using techniques standardized across
our institution with little procedural variation. The
radiologists paid careful attention to preventing
contact between the biopsy needle and the trans-
ducer during sampling (Fig. 1).
Biopsies were performed with either a spring-
loaded core needle or vacuum-assisted biopsy de-
vice ranging from 8 to 18 gauge. Most of the ul-
trasound-guided biopsies were performed with a Fig. 1Photograph
shows biopsy technique
14-gauge spring-loaded device; a minority were and relation between
performed with a vacuum-assisted device for very needle and probe.
2 AJR:208, May 2017
Ultrasound-Guided Breast Interventions
TABLE 1: Possible Procedure-Related Cases of Cellulitis
Technique
No. of Independent
Case No. of Procedure Passes per Site or No. of Age
Downloaded from www.ajronline.org by Fudan University Library on 02/23/17 from IP address 61.129.42.15. Copyright ARRS. For personal use only; all rights reserved
No. Procedure Sites per Breast Device Samples Obtained Year (y) Signs and Symptoms Clinical Outcomea
1 Biopsy 2, right 9-gauge vacuum- 2 passes 2006 58 Erythema Oral cephalexin
assisted
2 Biopsy 3, right 14-gauge spring-loaded; 7 passes; 2 passes; 2006 67 Erythema, warm to Oral cephalexin
9-gauge vacuum- 5and6 samples touch
assisted
3 Biopsy; fine-needle 3, right 2 14-gauge core needle; 4 passes 2007 59 Erythema with Oral cephalexin
aspiration 1fine-needle aspiration warmth, nodularity,
of right axilla slight tenderness
4 Biopsy 1, left 14-gauge spring-loaded 5 passes 2009 73 Erythema, slight Oral cephalexin
warmth
5 Biopsyb 1, left 9-gauge vacuum- 4 passes 2010 44 Erythema, tenderness Oral levofloxacin
assisted
6 Cyst aspiration 1, right 20-gauge needle 2011 46 Small hematoma Oral ciprofloxacin
witherythema,
warm to touch
7 Biopsy 2, right 9-gauge vacuum- 8 and 2 passes 2012 49 Patchy erythema Oral dicloxacillin
assisted
8 Biopsy 3, right 14-gauge spring-loaded 4, 5, and 5 passes 2012 42 Erythema, warmth Oral cephalexin
automatic
9 Biopsy 1, left 14-gauge 5 passes 2013 48 Erythema Oral cefadroxil
10 Biopsyb 1, left En bloc radiofrequency 2005 58 Erythema, warmth, Oral amoxicillin
tenderness
11 Biopsy 1, right 9-gauge vacuum- 5 samples 2006 78 Erythema Oral cephalexin
assisted
12 Biopsy 1, left 14-gauge automatic 5 passes 2011 56 Erythema, tenderness Oral cephalexin
13 Biopsy 1, left 13-gauge 3 passes 2012 66 Erythema, pain Oral cephalexin
14 Biopsy 1, left 14-gauge spring-loaded 5 passes 2013 67 Erythema, warmth, Oral levofloxacin
automatic tenderness
a All infections resolved with antibiotic treatment.
bCase detected in radiology surveillance database.
within 48 hours after the procedure and asked within the electronic medical record 2 days before sidered were removed from the final incidence cal-
about signs and symptoms related to postproce- and 30 days after the procedure, including infec- culation. Cases of potential infection thought to be
dural infection or hematoma. The nurse specifi- tion, mastitis, and cellulitis. Every biopsy pa- ambiguous or almost certainly resulting from the
cally asked whether the patient had increasing site tient chart included in the study time frame was ultrasound-guided procedure were included in the
redness, increasing tenderness, worsening bleed- searched for antibiotic use 2 days before and 30 statistical calculation and designated as possibly
ing, abnormal site warmth, or increasing swell- days after the procedure. A comprehensive list of related to the procedure.
ing. The nurse asked patients whether they felt all antibiotics used at our institution (240 antibiot-
feverish or had measured their temperature. Fi- ics) was used. Our goal was to find any individu- Results
nally, the nurse obtained a pain score on a tradi- al who may have had an infection or received an Infection Rates
tional 10-point scale and compared it with an im- antibiotic prescription within the aforementioned Our institution performed 12,708 ultra-
mediately postprocedural pain score. A pain score periprocedural time frame. A physician conduct- sound-guided procedure events from Janu-
greater than 4 was flagged for provider review. If ed a manual review of the information to identify ary 2005 to July 2013. Among these cases,
a patient was in the hospital, the nurse performed possible postprocedural infectious complications. 14 possible procedure-related infections oc-
a chart review. This process was discontinued in All potential cases of procedure-related infec- curred during that period, for an overall in-
2011 for the breast imaging practice because of the tion identified with these three approaches were cidence of 0.11%. The postprocedural in-
extremely low postprocedural complication rate. further evaluated by an infectious disease physi- fection rate for procedures performed with
Last, to ensure adequate infection detection, cian. Cases in which the complication was too far core and vacuum biopsy devices was 0.14%
a thorough retrospective computer and manual removed from the intervention to ensure causality, (13/9415). The postprocedural infection rate
chart review was undertaken. All charts of pa- physical examination findings were unsupportive for smaller-gauge aspiration procedures was
tients who had undergone an ultrasound-guid- of infection, or infection was less likely related to 0.03% (1/3293). The infections were 14 cas-
ed breast procedure were searched for keywords the procedure when the clinical history was con- es of skin and soft-tissue infection (Table 1).
AJR:208, May 2017 3
Reisenauer et al.
No cases of more advanced infection or sep- Given that procedures were performed time would likely decrease the time allotted
sis were identified. without ultrasound probe covers or a high- for procedures with no substantial addition
level disinfection protocol, this review fo- to patient safety. Before implementation of a
Infection Prevention and Control Strategy cused on detection of infection when an in- more costly and time-consuming high-level
Versus Radiologic Surveillance Versus termediate-level disinfection protocol was disinfection process, the breast imaging di-
Downloaded from www.ajronline.org by Fudan University Library on 02/23/17 from IP address 61.129.42.15. Copyright ARRS. For personal use only; all rights reserved
Retrospective Chart Review used. From an infectious disease standpoint, vision attempted to validate the safety of in-
No cases were identified through the pro- intermediate-level disinfection has been termediate-level disinfection without a probe
spective data compiled by the IPC committee found to kill vegetative bacteria, mycobac- cover. Given the extremely low risk of infec-
database. The low detection sensitivity of the teria, most viruses, and fungi [15]. Alterna- tion identified in this study and contributions
IPC database should be directly related to the tively, high-level disinfection has been found from other related studies, which showed in-
low severity of the focal skin and soft-tissue to kill all microorganisms except for a small fection rates ranging from as low as 0% [3,
infections and lack of clinical need for blood number of bacterial spores [15]. The imple- 69] to 0.12% [5], escalation of disinfection
or tissue cultures, admission, or surgical drain- mentation of a high-level disinfection proto- to higher than intermediate level for the pur-
age, which are required for IPC detection. col and use of a probe cover would increase pose of nosocomial infection control was de-
Two cases were identified in the radiolo- microbial coverage with the consequence of termined to be unnecessary in our practice.
gy surveillance database. The patients in the additional cost and time in every procedure. Our institutions transducer disinfection
other 12 cases had no symptoms or concerns The U.S. Centers for Disease Control and protocol was amended in part on the basis of
during the immediate surveillance period, Prevention recommends high-level disinfec- the results of this study and adapted as effec-
experienced symptoms after the 24-hour tion and probe cover use for any sonograph- tive policy. Any sterile nonvascular, nonsur-
surveillance period, or presented after 2011, ic procedure that involves nonintact skin gical puncturing procedure that requires an
when the radiologic surveillance program or use of an endocavitary probe, including ultrasound probe requires a minimum of in-
was terminated. These 12 patients with pos- breast interventions [15]. Because of a lack termediate-level disinfection without a probe
sible procedure-related infections presented of clinical studies showing infection risk to a cover. Vascular access puncturing proce-
to the emergency department or contacted patient undergoing ultrasound-guided inter- dures and procedures performed in the oper-
their primary caregiver and were identified ventions, this recommendation appears to be ating theater require high-level disinfection
in the retrospective chart review. based on theoretic risk and nonclinical data. and a probe cover. The decision to continue
Nineteen potential cases were identified Many studies have documented the risk of with intermediate-level disinfection for ul-
in retrospective computer and manual chart nosocomial infection through communal trasound-guided breast procedures resulted
review. Five were eliminated after review use of ultrasound transmission gel [1623]. in cost containment while safe and effective
by an infectious disease physician and two Several studies also have shown the utili- procedural disinfection was maintained.
breast imaging radiologists. The cases in ty of high-level disinfection and the risk of This study also allowed us to evaluate the
which the complication was too far removed perforation of probe covers on endocavitary infection incidence as our policies regard-
from the intervention to ensure causality, probes and during open surgical procedures, ing intermediate-level disinfection changed
cultures were not available, physical exami- which may predispose the patient to noso- from 2005 to 2013. We noted no statistically
nation findings were unsupportive of infec- comial infection [2428]. However, data are significant change in infection rates between
tion, or infection was less likely related to insufficient to show a benefit of high-level cleansing with povidone-iodine in 2005 to
the procedure when the clinical history was disinfection for a minimally invasive pro- the more expensive and time-consuming in-
considered were removed from the final sta- cedure with limited skin violation in which termediate-level protocol we currently use.
tistical incidence calculation. Ultimately, 14 needle size ranges from 8- to 25-gauge. To Current practice guidelines for ultra-
cases of potential infection thought possibly our knowledge, a clinical study specifically sound-guided breast procedures have been
related to an ultrasound-guided procedure showing a statistically significant differing formulated on the basis of theoretic risk,
were included in the statistical calculation. infectious complication rate with different data extrapolated from nonclinical studies,
levels of disinfection or use of probe covers or broadening of the conclusions of modal-
Clinical Outcomes has not been performed. ity-related studies, for example, implemen-
All patients improved with a short-term In an effort to standardize institutional tation of recommendations for ultrasound-
course of oral antibiotics (Table 1). No cas- practices, the IPC committee at our institu- guided biopsy based on risk assessment of
es of abscess formation or sepsis were noted. tion has proposed escalation of ultrasound endocavitary probe examinations. Our data
No additional procedures or hospitalizations probe disinfection for breast interventions validate that the risk of infection is minimal
were required. to a high-level disinfection protocol or use when intermediate-level disinfection is used
of a probe cover. The high-level disinfection during ultrasound-guided breast biopsy and
Discussion protocol proposed would add approximately that high-quality care is maintained, daily
At our institution, the infection rate after 15 minutes of probe disinfection and qual- work flow is improved, and system waste and
an ultrasound-guided procedure performed ity control time to every ultrasound-guided cost are minimized.
with intermediate-level disinfection without procedure. Our breast imaging division av- Our study had several limitations. The
a probe cover is 0.11%. This infection rate is erages 10 procedures daily, and the addi- prospective surveillance by the IPC com-
statistically comparable to those of lower-pow- tional disinfection and quality control time mittee was based on microbiology records or
ered studies of variable disinfection protocols would add approximately 150 minutes of in- complications serious enough to precipitate
for ultrasound-guided breast procedures [18]. efficient nonvalue-added work daily. This hospital admission or an operating room vis-
4 AJR:208, May 2017
Ultrasound-Guided Breast Interventions
it. Therefore, minor infections, such as cel- tion, which would have falsely elevated the 5. Verkooijen HM, Peeters PH, Buskens E, et al. Di-
lulitis, might have been appropriately over- incidence of infectious complications. Fur- agnostic accuracy of large-core needle biopsy for
looked by the IPC committee. Along these thermore, the inability to differentiate cases nonpalpable breast disease: a meta-analysis. BrJ
same lines, the decision to order cultures and that included multisite interventions lowered Cancer 2000; 82:10171021
additional clinical management depended on the overall number of independent proce- 6. Zannis VJ, Aliano KM. The evolving practice pat-
Downloaded from www.ajronline.org by Fudan University Library on 02/23/17 from IP address 61.129.42.15. Copyright ARRS. For personal use only; all rights reserved
the caregiver. However, we believe our retro- dures that were performed in the time frame tern of the breast surgeon with disappearance of
spective chart review and radiologic surveil- of this study and used for the denominator of open biopsy for nonpalpable lesions. AmJ Surg
lance database search to identify infections the incidence calculation of infectious com- 1998; 176:525528
were comprehensive and identified low-se- plications. If each procedure site and not 7. Smith DN, Rosenfield Darling ML, Meyer JE, et al.
verity infectious complications. each patient who underwent an ultrasound- The utility of ultrasonographically guided large-
A potential limitation was the 48-hour guided procedure were accounted for, the core needle biopsy: results from 500 consecutive
postprocedural time frame that we used to overall infection incidence rate would have breast biopsies. JUltrasound Med 2001; 20:4349
define procedure-related bacteremia. Our been less than 0.11%. The number of infec- 8. Gisvold JJ, Goellner JR, Grant CS, et al. Breast
institutions experience with other interven- tions detected during the time frame would biopsy: a comparative study of stereotaxically
tions suggests that few procedure-related not have been affected by this limitation on guided core and excisional techniques. AJR 1994;
cases of bacteremia occur after 24 hours. the basis of the methods used for detection 162:815820
The independent retrospective review of in this study. 9. Yeow KM, Lo YF, Wang CS, et al. Ultrasound-
electronic medical records did not identify Only ultrasound-guided procedures were guided core needle biopsy as an initial diagnostic
any cases of bacteremia or of patients who evaluated in this study. Assuming similar in- test for palpable breast masses. JVasc Interv
needed IV antibiotics that were not identified dications, techniques, and durations of in- Radiol 2001; 12:13131317
in the IPC database. terventions, it is conceivable that the results 10. March DE, Coughlin BF, Barham RB, et al. Breast
No data were collected on the incidence or with stereotactic techniques or MRI guid- masses: removal of all US evidence during biopsy
severity of bleeding complications; the sole ance would be similar. by using a handheld vacuum-assisted deviceini-
purpose of this study was to assess for in- In summary, we found that the incidence tial experience. Radiology 2003; 227:549555
fectious complications related to procedural of infection after ultrasound-guided inter- 11. Parker SH, Jobe WE, Dennis MA, et al. US-guid-
technique. Any patient who had a hematoma vention is extremely low with the use of in- ed automated large-core breast biopsy. Radiology
and chart documentation of infection or re- termediate-level disinfection without an 1993; 187:507511
ceived a prescription for an antibiotic would ultrasound probe cover. Furthermore, the in- 12. Harvey JA, Moran RE. US-guided core needle bi-
have been revealed in our chart search. Of fectious complications were low-severity in- opsy of the breast: technique and pitfalls.
the 14 patients with a possible procedure-re- fections that did not require hospitalization RadioGraphics 1998; 18:867877
lated infection, one had documentation of a and resolved with oral antibiotics alone. Phy- 13. OFlynn EA, Wilson AR, Michell MJ. Image-
small hematoma. sicians can use these data to provide accurate guided breast biopsy: state-of-the-art. Clin Radiol
It is possible that additional minor infec- information to patients during the consent 2010; 65:259270
tious complications were unaccounted for discussion before procedures and to reas- 14. Cervini P, Hesley GK, Thompson RL, S ampathkumar
because over the time frame of this study 755 sure patients. These data may also be helpful P, Knudsen JM. Incidence of infectious complica-
patients did not authorize use of their medi- to providers making decisions about appro- tions after an ultrasound-guided intervention. AJR
cal records for retrospective chart review and priate disinfection protocols for ultrasound- 2010; 195:846850
research purposes. No advanced infections guided breast procedures so that they may 15. Rutala WA, Weber DJ; Healthcare Infection Control
or abscesses were detected in the IPC data- factor in the efficacy of intermediate-level Practices Advisory Committee. Guideline for disin-
base. Therefore, no postprocedural compli- disinfection, cost containment, system waste, fection and sterilization in healthcare facilities, 2008.
cation required IV antibiotics, blood or tis- and longer turnover time requirements for www.cdc.gov/hicpac/pdf/guidelines/Disinfection_
sue cultures, admission, or surgical drainage, higher-level disinfection protocols. Nov_2008.pdf. 2008. Accessed September 15, 2015
in this population of 755 patients. 16. Olshtain-Pops K, Block C, Temper V, et al. An
Another limitation was the inability to References outbreak of Achromobacter xylosoxidans associ-
differentiate cases that included multisite in- 1. Parker SH, Burbank F, Jackman RJ, et al. Percuta- ated with ultrasound gel used during transrectal
terventions during the same procedure ses- neous large-core breast biopsy: a multi-institu- ultrasound guided prostate biopsy. JUrol 2011;
sion, needle gauge size, use of an introducer, tional study. Radiology 1994; 193:359364 185:144147
and number of passes based on our institu- 2. Meyer JE, Smith DN, Lester SC, et al. Large-core 17. Keizur JJ, Lavin B, Leidich RB. Iatrogenic uri-
tions reporting and archiving systems. Spe- needle biopsy of nonpalpable breast lesions. nary tract infection with Pseudomonas cepacia
cifically regarding multisite interventions, JAMA 1999; 281:16381641 after transrectal ultrasound guided needle biopsy
a minority of the procedures performed in- 3. Parker SH, Lovin JD, Jobe WE, et al. Stereotactic of the prostate. JUrol 1993; 149:523526
cluded multiple biopsies of the same breast breast biopsy with a biopsy gun. Radiology 1990; 18. Hutchinson J, Runge W, Mulvey M, et al. Burk-
for synchronous suspicious lesions. Of the 176:741747 holderia cepacia infections associated with in-
14 cases attributed to procedure-related in- 4. Sauer G, Deissler H, Strunz K, et al. Ultrasound- trinsically contaminated ultrasound gel: the role
fections, five cases were multisite biop- guided large-core needle biopsies of breast le- of microbial degradation of parabens. Infect Con-
sies. Some of these patients may have had sions: analysis of 962 cases to determine the num- trol Hosp Epidemiol 2004; 25:291296
increased pain and erythema related to the ber of samples for reliable tumour classification. 19. Weist K, Wendt C, Petersen L, Versmold H, Ruden
procedures rather than to an actual infec- BrJ Cancer 2005; 92:231235 H. An outbreak of pyodermas among neonates
AJR:208, May 2017 5
Reisenauer et al.
caused by ultrasound gel contaminated with (CDC). Outbreak of Pseudomonas aeruginosa 25. Storment JM, Monga M, Blanco JD. Ineffective-
methicillin-susceptible Staphylococcus aureus. respiratory tract infections in cardiovascular sur- ness of latex condoms in preventing contamina-
Infect Control Hosp Epidemiol 2000; 21:761764 gery associated with contaminated ultrasound gel tion of the transvaginal ultrasound transducer
20. Gaillot O, Maruejouls C, Abachin E, et al. Nosoco- used for transesophageal echocardiography: head. South Med J 1997; 90:206208
mial outbreak of Klebsiella pneumoniae produc- Michigan, December 2011January 2012. MMWR 26. Tunstall TD. Infection control in the sonography de-
Downloaded from www.ajronline.org by Fudan University Library on 02/23/17 from IP address 61.129.42.15. Copyright ARRS. For personal use only; all rights reserved
ing SHV-5 extended-spectrum -lactamase, origi- Morb Mortal Wkly Rep 2012; 61:262264 partment. J Diagn Med Sonogr 2010; 26: 190197
nating from a contaminated ultrasonography 23. Oleszkowicz SC, Chittick P, Russo V, Keller P, 27. Hignett M, Claman P. High rates of perforation
coupling gel. JClin Microbiol 1998; 36:13571360 Sims M, Band J. Infections associated with use of are found in endovaginal ultrasound probe covers
21. Jacobson M, Wray R, Kovach D, Henry D, Speert D, ultrasound transmission gel: proposed guidelines before and after oocyte retrieval for in vitro fertil-
Matlow A. Sustained endemicity of Burkholderia to minimize risk. Infect Control Hosp Epidemiol ization-embryo transfer. J Assist Reprod Genet
cepacia complex in a pediatric institution, associat- 2012; 33:12351237 1995; 12:606609
ed with contaminated ultrasound gel. Infect Control 24. Milki AA, Fisch JD. Vaginal ultrasound probe 28. Rooks VJ, et al. Comparison of probe sheaths for
Hosp Epidemiol 2006; 27:362366 cover leakage: implications for patient care. Fertil endovaginal sonography. Obstet Gynecol 1996;
22. Centers for Disease Control and Prevention Steril 1998; 69:409411 87:2729
F O R YO U R I N F O R M AT I O N
This article has been selected for AJR Journal Club activity. The accompanying Journal Club
Study Guide can be found on the following page.
6 AJR:208, May 2017
Ultrasound-Guided Breast Interventions
AJR Journal Club
Study Guide
Ultrasound-Guided Breast Interventions:
Downloaded from www.ajronline.org by Fudan University Library on 02/23/17 from IP address 61.129.42.15. Copyright ARRS. For personal use only; all rights reserved
LowIncidence of Infectious Complications
WithUseof an Uncovered Probe
Alan Mautz1, Margaret Mulligan2 , Joseph J. Budovec2
1The Aroostook Medical Center, Presque Isle, ME.
2 Medical College of Wisconsin, Milwaukee, WI.
amautz@emhs.org, mmulliga@mcw.edu, jbudovec@mcw.edu*
Introduction
1. What was the purpose of the study? Was the rationale for the study adequately discussed?
2. How would you formalize the studys hypothesis?
Methods
3. What study design was used for the study? What limitations are inherent in this type of study design?
4. What were the inclusion criteria for the study? What were the exclusion criteria?
5. What were the limitations of this study? Were these limitations adequately acknowledged and discussed?
6. The article described three mechanisms of follow-up for patients who had undergone biopsy. Describe the mechanisms of follow-up and
how the study attempts to ensure the most conservative estimate of postprocedural infection rate.
Results
7. Was the research question answered? Are the results replicable?
8. What was the rate of infection after ultrasound-guided biopsy?
Hospital Policy
9. How are infection control policies determined and published at your institution? Can you find such policies if necessary? Does your de-
partment have a mechanism in place to proactively identify potential procedural complications?
10. The article included a brief discussion of the need to balance appropriate infection control with a busy biopsy practice and sound medical
practice. Do you think such a study or change in practice as these authors advocate would be possible at your institution? How does your
institution balance cost containment with risk avoidance and management?
Discussion
11. What are the current infection control protocols in your department? What measures do you take during image-guided procedures to re-
duce the risk of infection, both to the operator and to the patient?
12. Do you anticipate making changes to your departmental practice based on this study? Why or why not?
13. How amenable would your partners, departmental administrators, and hospital administration be if you sought to alter biopsy technique
or ultrasound transducer disinfection protocols?
14. The study provides an economic rationale for performing ultrasound-guided biopsies without a probe cover provided the risk of infection
is not increased. What other considerations merit inclusion in a discussion of infection control protocols? Should patient perception be
considered?
Background Reading
1. Cervini P, Hesley GK, Thompson RL, Sampathkumar P, Knudsen JM. Incidence of infectious complications after an ultrasound-guided intervention. AJR 201;
195:846850
2. Tunstall TD. Infection control in the sonography department. J Diagn Med Sonogr 2010; 26:190197
*Please note that the authors of the Study Guide are distinct from those of the companion article.
AJR:208, May 2017 7
You might also like
- Breast Procedures Ultrasound Only EditedDocument107 pagesBreast Procedures Ultrasound Only EditedDanaNo ratings yet
- Anatomic Pathology Haematology Medical Microbiology Chemical Pathology Forensic Pathology ...Document85 pagesAnatomic Pathology Haematology Medical Microbiology Chemical Pathology Forensic Pathology ...Kunal NakkanaNo ratings yet
- 1 Introduction To General PathologyDocument91 pages1 Introduction To General PathologyCoy NuñezNo ratings yet
- Ruth Drown Laboratories 1960 - Radio-Vision A Scientific MilestoneDocument28 pagesRuth Drown Laboratories 1960 - Radio-Vision A Scientific MilestoneZicky100% (4)
- MCQ Breast Surgery Bordeaux 2010Document9 pagesMCQ Breast Surgery Bordeaux 2010Ismail Evren100% (1)
- Surgical OncologyDocument331 pagesSurgical OncologySara Pereira Libório100% (4)
- 3 Abdominal Ultrasound Imaging AnatomyDocument7 pages3 Abdominal Ultrasound Imaging Anatomyjefaturaimagenologia Hospital NogalarNo ratings yet
- Capitol University College of Nursing RLE 6 List of Supervised Nursing ProceduresDocument9 pagesCapitol University College of Nursing RLE 6 List of Supervised Nursing Proceduresjizea05100% (3)
- Ultrasound in Gynecology and ObstetricsDocument197 pagesUltrasound in Gynecology and ObstetricsAli Murtaza AbbasNo ratings yet
- Invasive Cytopathology UltreasoundDocument476 pagesInvasive Cytopathology UltreasoundAlexander KovalenkoNo ratings yet
- Role of Automated Breast Ultrasound in Diagnostic and Early Detection 5-1Document47 pagesRole of Automated Breast Ultrasound in Diagnostic and Early Detection 5-1Dokdem AjaNo ratings yet
- Bone Marrow InterpretationDocument32 pagesBone Marrow InterpretationHimanshu Bansal100% (3)
- Common and Uncommon Applications of Bowel Ultrasound With Pathologic Correlation in ChildrenDocument14 pagesCommon and Uncommon Applications of Bowel Ultrasound With Pathologic Correlation in Childrengrahapuspa17No ratings yet
- Initial Radiographic Features As Outcome Predictor of Adult Respiratory Syncytial Virus Respiratory Tract InfectionDocument7 pagesInitial Radiographic Features As Outcome Predictor of Adult Respiratory Syncytial Virus Respiratory Tract Infectionaristya_tyaNo ratings yet
- Ultrasound Imaging of Bowel Pathology - Technique and Keys To Diagnosis in The Acute Abdomen, 2011Document9 pagesUltrasound Imaging of Bowel Pathology - Technique and Keys To Diagnosis in The Acute Abdomen, 2011Сергей СадовниковNo ratings yet
- Analisis Jurnal Tentang Faktor-Faktor Yang Mempengaruhi Deteksi Dini Kanker Serviks Dengan Analia PicotDocument9 pagesAnalisis Jurnal Tentang Faktor-Faktor Yang Mempengaruhi Deteksi Dini Kanker Serviks Dengan Analia PicotVelinia WijayantiNo ratings yet
- Diagnostic Procedures in Gynecology (2023)Document3 pagesDiagnostic Procedures in Gynecology (2023)RONALDO CUANo ratings yet
- Ultrasonography Report PDFDocument3 pagesUltrasonography Report PDFKruthi M LNo ratings yet
- Complete Seminar by Rad Rabiu S YunusaDocument26 pagesComplete Seminar by Rad Rabiu S YunusaRabiu Salisu yunusaNo ratings yet
- Manual Compared With Electric Vacuum Aspiration For Treatment of Molar PregnancyDocument8 pagesManual Compared With Electric Vacuum Aspiration For Treatment of Molar PregnancyTưởng Minh QuốcNo ratings yet
- Lin 2017Document11 pagesLin 2017Ibnu CaesarNo ratings yet
- Women in Interventional Radiology: How Are We Doing?: Meridith J. Englander Susan K. O'HoroDocument5 pagesWomen in Interventional Radiology: How Are We Doing?: Meridith J. Englander Susan K. O'HoroEsme Q.No ratings yet
- Angle of Progression Measurements of Fetal Head at Term, A Systematic Comparison Between Open Magnetic Resonance Imaging and Transperineal UltrasoundDocument5 pagesAngle of Progression Measurements of Fetal Head at Term, A Systematic Comparison Between Open Magnetic Resonance Imaging and Transperineal UltrasoundNella SolanoNo ratings yet
- Geleta, 2021Document8 pagesGeleta, 2021Chingura LuffyNo ratings yet
- Paediatric Respiratory Reviews: Tanyia Pillay, Savvas Andronikou, Heather J. ZarDocument8 pagesPaediatric Respiratory Reviews: Tanyia Pillay, Savvas Andronikou, Heather J. ZarSatria Bayu PratamaNo ratings yet
- Time Imaging .: Ultrasonography Machine For Veterinary ApplicationDocument22 pagesTime Imaging .: Ultrasonography Machine For Veterinary ApplicationKanhaiyalal RamNo ratings yet
- The Adoption of Ultrasound Guided Radiofrequency.31Document3 pagesThe Adoption of Ultrasound Guided Radiofrequency.31drhusseinfaour3126No ratings yet
- Situs Inversus JClinSci - 2018 - 15 - 3 - 168 - 244747Document4 pagesSitus Inversus JClinSci - 2018 - 15 - 3 - 168 - 244747Anonymous 9QxPDpNo ratings yet
- Stoelinga 2021Document14 pagesStoelinga 2021ShagorNo ratings yet
- Measurement of Ovarian Size and Shape ParametersDocument7 pagesMeasurement of Ovarian Size and Shape ParametersRamisha RaidaNo ratings yet
- Contraceptive Implants Current Perspectives PDFDocument13 pagesContraceptive Implants Current Perspectives PDFCostin VrabieNo ratings yet
- Contraceptive Implants Current Perspectives PDFDocument13 pagesContraceptive Implants Current Perspectives PDFCostin VrabieNo ratings yet
- USrelatedbioeffects Anesthesiology 2011Document17 pagesUSrelatedbioeffects Anesthesiology 2011HhtNo ratings yet
- Translate Medscape REF 02Document2 pagesTranslate Medscape REF 02Pridina SyadirahNo ratings yet
- The Histofy of ObstetrictDocument19 pagesThe Histofy of ObstetrictKathyNogalesNo ratings yet
- Enjelina Siahaan-151221151-Ekstraksi Karya IlmiahDocument1 pageEnjelina Siahaan-151221151-Ekstraksi Karya IlmiahEnjelina SiahaanNo ratings yet
- Diagnostic Studies For Musculoskeletal DisordersDocument16 pagesDiagnostic Studies For Musculoskeletal DisordersClarisse Anne QuinonesNo ratings yet
- US SafetyDocument12 pagesUS SafetyHarley Alejo MNo ratings yet
- Comparison of Clinical Diagnosis With Radiological.5Document5 pagesComparison of Clinical Diagnosis With Radiological.5Lissette RoseroNo ratings yet
- FI JRNLDocument6 pagesFI JRNLradiology koba22No ratings yet
- Ultrasonography Principles Indications and Limitations PDFDocument3 pagesUltrasonography Principles Indications and Limitations PDFMuchtar RezaNo ratings yet
- Ajr 19 21383Document10 pagesAjr 19 21383chachaNo ratings yet
- The Skin-To-Epidural Distance of Parturients by UlDocument5 pagesThe Skin-To-Epidural Distance of Parturients by UlzakyNo ratings yet
- Pediatric Musculoskeletal Ultrasound: Practical Imaging ApproachDocument11 pagesPediatric Musculoskeletal Ultrasound: Practical Imaging ApproachcdatNo ratings yet
- Olinger Et Al 2024 Added Value of Contrast Enhanced Us For Evaluation of Female Pelvic DiseaseDocument15 pagesOlinger Et Al 2024 Added Value of Contrast Enhanced Us For Evaluation of Female Pelvic DiseaseThesisaurus IDNo ratings yet
- Lecture 2 Ultrasound PrinciplesDocument44 pagesLecture 2 Ultrasound Principlesalfredo gutierrezNo ratings yet
- Wjols 14 98Document5 pagesWjols 14 98Ancuta Raluca TiperciucNo ratings yet
- Mother ArticleDocument6 pagesMother ArticleRakesh JhaNo ratings yet
- Cognitive and System Factors Contributing To Diagnostic Errors in RadiologyDocument7 pagesCognitive and System Factors Contributing To Diagnostic Errors in Radiologydianfahmi63No ratings yet
- 1 s2.0 S0378603X17300037 MainDocument6 pages1 s2.0 S0378603X17300037 MainVicennia SerlyNo ratings yet
- Publicação JPUDocument6 pagesPublicação JPUProdutos IntraviewNo ratings yet
- Prevalence and Predictors of Syphilis in Female Sex Workers in Eastern China, Findings From Six Consecutive Cross-Sectional SurveysDocument8 pagesPrevalence and Predictors of Syphilis in Female Sex Workers in Eastern China, Findings From Six Consecutive Cross-Sectional SurveysFrans LandiNo ratings yet
- Transabdominal Sonography in Assessment of The Bowel in AdultsDocument16 pagesTransabdominal Sonography in Assessment of The Bowel in AdultsСергей СадовниковNo ratings yet
- Uterine Perforation After Pose of IUD, The Place of Abdomen Radiography Without PreparationDocument5 pagesUterine Perforation After Pose of IUD, The Place of Abdomen Radiography Without Preparationvianchasamiera berlianaNo ratings yet
- Sudden Sensorineural Hearing Loss in Children Clinical Characteristic Etiology Treatments Outcomes, and Prognostic FactorsDocument8 pagesSudden Sensorineural Hearing Loss in Children Clinical Characteristic Etiology Treatments Outcomes, and Prognostic FactorsneneNo ratings yet
- Oajc 281504 Determinants of Postpartum Contraception Use Among Teenage MDocument9 pagesOajc 281504 Determinants of Postpartum Contraception Use Among Teenage MIfa al hadiNo ratings yet
- Recommendation of Pre-Operative Screening Intervention Evaluation Nursing Intervention Manpower Resources RequiredDocument7 pagesRecommendation of Pre-Operative Screening Intervention Evaluation Nursing Intervention Manpower Resources RequiredBernice EbbiNo ratings yet
- Single Step Gastric Aspirate Shake Test AsDocument12 pagesSingle Step Gastric Aspirate Shake Test AsFariz HidayatNo ratings yet
- Histeroscopy 4Document4 pagesHisteroscopy 4Silvia IzvoranuNo ratings yet
- EVIEWDocument20 pagesEVIEWmNo ratings yet
- Publicação ICSDocument7 pagesPublicação ICSProdutos IntraviewNo ratings yet
- Ajr 13 12264Document9 pagesAjr 13 12264marizal saputraNo ratings yet
- JCanResTher127138-5663271 154352Document5 pagesJCanResTher127138-5663271 154352Prosanta Kr BhattacharjeeNo ratings yet
- AlemayehuDocument8 pagesAlemayehuasriadiNo ratings yet
- Ultrasound AND Congenital Dislocation OF THE HIP: From Nuffield Orthopaedic Centre, OxfordDocument5 pagesUltrasound AND Congenital Dislocation OF THE HIP: From Nuffield Orthopaedic Centre, OxfordRéka TéglásNo ratings yet
- What The Radiologist Needs To Know About Urolithiasis: Part 1 - Pathogenesis, Types, Assessment, and Variant AnatomyDocument8 pagesWhat The Radiologist Needs To Know About Urolithiasis: Part 1 - Pathogenesis, Types, Assessment, and Variant AnatomyQonita Aizati QomaruddinNo ratings yet
- Thyroid Ultrasound and Ultrasound-Guided FNAFrom EverandThyroid Ultrasound and Ultrasound-Guided FNAH. Jack Baskin, Sr.No ratings yet
- Jurnal Rad4Document5 pagesJurnal Rad4Sandy MurtiningtyasNo ratings yet
- Inkompatibilitas 2015Document49 pagesInkompatibilitas 2015Sandy MurtiningtyasNo ratings yet
- DM FK Ums 14Document70 pagesDM FK Ums 14Sandy MurtiningtyasNo ratings yet
- JurnalDocument6 pagesJurnalSandy MurtiningtyasNo ratings yet
- Eni SugiartiDocument12 pagesEni SugiartiSandy MurtiningtyasNo ratings yet
- 2015 Eng TSK AcecutDocument2 pages2015 Eng TSK AcecuttutagNo ratings yet
- Examination of The Female BreastDocument14 pagesExamination of The Female BreastCharles FrankNo ratings yet
- Malignant and Benign Breast Cancer Classification Using Machine Learning AlgorithmsDocument5 pagesMalignant and Benign Breast Cancer Classification Using Machine Learning AlgorithmsRohit SinghNo ratings yet
- Case PresentationDocument138 pagesCase PresentationrinlopenaiNo ratings yet
- Assisting With Aspirations - Bone Marrow Aspiration-Biopsy, Lumbar Puncture, Paracentesis, and ThoracentesisDocument5 pagesAssisting With Aspirations - Bone Marrow Aspiration-Biopsy, Lumbar Puncture, Paracentesis, and Thoracentesisreggiesalcedo111No ratings yet
- NRL Laboratory Collection ManualDocument27 pagesNRL Laboratory Collection ManualZeeshan AhmedNo ratings yet
- (Self-Assessment Color Review) Joyce E. Obradovich - Small Animal Clinical Oncology - Self-Assessment Color review-CRC Press (2017)Document329 pages(Self-Assessment Color Review) Joyce E. Obradovich - Small Animal Clinical Oncology - Self-Assessment Color review-CRC Press (2017)dpcamposhNo ratings yet
- 2023 Aaha Senior Care Guidelines For Dogs and CatsDocument21 pages2023 Aaha Senior Care Guidelines For Dogs and CatsisvpNo ratings yet
- 34 Use of Ultrasound in Breast Surgery.Document16 pages34 Use of Ultrasound in Breast Surgery.waldemar russellNo ratings yet
- Ingles 2Document4 pagesIngles 2Natalia AriasNo ratings yet
- Unilateral Tonsil EnlargementDocument5 pagesUnilateral Tonsil EnlargementBryan Albert LimNo ratings yet
- BiopsiesDocument13 pagesBiopsiesSubbu ManiNo ratings yet
- Breast Cancer (Research Paper)Document12 pagesBreast Cancer (Research Paper)Katrina Arnaiz100% (3)
- 1 s2.0 S1368837518304299 MainDocument8 pages1 s2.0 S1368837518304299 MainIgor VainerNo ratings yet
- Advantage and Disadvantage of FNACDocument13 pagesAdvantage and Disadvantage of FNACDebayan KarmakarNo ratings yet
- In Service Exam For Breast DR Paul BalisiDocument11 pagesIn Service Exam For Breast DR Paul BalisiAmiel Francisco ReyesNo ratings yet
- EndoscopeOverview 2022 105x210 EN-GRZ 07 02 2022Document17 pagesEndoscopeOverview 2022 105x210 EN-GRZ 07 02 2022lied cnNo ratings yet
- Bone Marrow ThesisDocument5 pagesBone Marrow Thesisjennifermowerwestvalleycity100% (2)
- Amedee 2001Document7 pagesAmedee 2001Hakim naufaldiNo ratings yet
- Assisting Bone Marrow Aspiration DraftDocument6 pagesAssisting Bone Marrow Aspiration Draftabcde pwnjabiNo ratings yet
- Cytology and Cytological TechniquesDocument29 pagesCytology and Cytological TechniquessafiNo ratings yet
- Lab Tech Solimullah Phase ADocument30 pagesLab Tech Solimullah Phase AAbdullah Yeamin PeyalNo ratings yet
- The Term Thyroid Nodule Refers To An Abnormal Growth of Thyroid Cells That Forms A Lump Within The Thyroid GlandDocument4 pagesThe Term Thyroid Nodule Refers To An Abnormal Growth of Thyroid Cells That Forms A Lump Within The Thyroid GlandMira MerintanNo ratings yet