You might also like
- A Real-Time Gyroscopic System For Three-DimensionaDocument9 pagesA Real-Time Gyroscopic System For Three-DimensionaErna TamiziNo ratings yet
- Sensors-13-14466 (Published Article)Document18 pagesSensors-13-14466 (Published Article)Erna TamiziNo ratings yet
- Automatic Tracking Measurement System On Human Lumbar Vertebral MotionDocument4 pagesAutomatic Tracking Measurement System On Human Lumbar Vertebral MotionebrahimpanNo ratings yet
- Kinematics of Rotational Mobilisation of The Lumbar SpineDocument8 pagesKinematics of Rotational Mobilisation of The Lumbar SpinePablo RdzNo ratings yet
- Medical Engineering & PhysicsDocument7 pagesMedical Engineering & PhysicsebrahimpanNo ratings yet
- Wearable Sensors For Gait AnalysisDocument5 pagesWearable Sensors For Gait AnalysissanahujalidiaNo ratings yet
- Journal of Biomechanics: J. Favre, R. Aissaoui, B.M. Jolles, J.A. de Guise, K. AminianDocument6 pagesJournal of Biomechanics: J. Favre, R. Aissaoui, B.M. Jolles, J.A. de Guise, K. Aminianconstantinescuana200No ratings yet
- Measuring Limb Length Discrepancy Using Pelvic Radiographs: The Most Reproducible MethodDocument5 pagesMeasuring Limb Length Discrepancy Using Pelvic Radiographs: The Most Reproducible MethodBudhiNo ratings yet
- Medical Engineering and PhysicsDocument7 pagesMedical Engineering and Physicsdaniel QuinteroNo ratings yet
- Foot2hip: A Deep Neural Network Model For Predicting Lower Limb Kinematics From Foot MeasurementsDocument11 pagesFoot2hip: A Deep Neural Network Model For Predicting Lower Limb Kinematics From Foot Measurementsbhavesh agrawalNo ratings yet
- Development of A Flexible System For Measuring Muscle Area Using UltrasonographyDocument9 pagesDevelopment of A Flexible System For Measuring Muscle Area Using UltrasonographyGihan MendisNo ratings yet
- Reliability and Validity of A Clinical Assessment Tool For Measuring Scapular Motion in All 3 Anatomical PlanesDocument8 pagesReliability and Validity of A Clinical Assessment Tool For Measuring Scapular Motion in All 3 Anatomical PlanesAronNo ratings yet
- Movement Biomechanics Goes Upwards-From The Leg To The ArmDocument10 pagesMovement Biomechanics Goes Upwards-From The Leg To The ArmMuhammad FahmyNo ratings yet
- Sensors 22 03859Document15 pagesSensors 22 0385954m8mj5qn9No ratings yet
- Wearable Optical Sensor For Low Back Pain Monitoring: Erna B. Tamizi M. A. Zawawi Corresponding Author Roszitaida ADocument7 pagesWearable Optical Sensor For Low Back Pain Monitoring: Erna B. Tamizi M. A. Zawawi Corresponding Author Roszitaida AErna TamiziNo ratings yet
- Low Cost Portable Sensor For Real-Time Monitoring of Lower Back BendingDocument4 pagesLow Cost Portable Sensor For Real-Time Monitoring of Lower Back BendingebrahimpanNo ratings yet
- Asaeda 2018Document5 pagesAsaeda 2018alonsoNo ratings yet
- DeformitiesDocument10 pagesDeformitiesNitya KrishnaNo ratings yet
- Gait & Posture: Full Length ArticleDocument7 pagesGait & Posture: Full Length ArticleMKNo ratings yet
- Three-Dimensional Dynamic in Vivo Motion of The Cervical Spine: Assessment of Measurement Accuracy and Preliminary FindingsDocument8 pagesThree-Dimensional Dynamic in Vivo Motion of The Cervical Spine: Assessment of Measurement Accuracy and Preliminary FindingsFayza RihastaraNo ratings yet
- Accuracy and Longitudinal Reproducibility of QuantDocument18 pagesAccuracy and Longitudinal Reproducibility of QuantChristian Huapaya ContrerasNo ratings yet
- Measuring Knee Motion DigitallyDocument5 pagesMeasuring Knee Motion DigitallyAna-Maria ȘtefanNo ratings yet
- A Pervasive Sensing Approach To Automatic Assessment of Trunk Coordination Using Mobile DevicesDocument18 pagesA Pervasive Sensing Approach To Automatic Assessment of Trunk Coordination Using Mobile DevicesZilu LiangNo ratings yet
- Scanner For Trac: Student Member, Senior Member, ZEEE, Senior Member, ZEEEDocument2 pagesScanner For Trac: Student Member, Senior Member, ZEEE, Senior Member, ZEEEKavitha ShenoyNo ratings yet
- A Preclinical Method For Evaluating The Kinematics - 2019 - Medical EngineeringDocument7 pagesA Preclinical Method For Evaluating The Kinematics - 2019 - Medical EngineeringEzgi PelitNo ratings yet
- Virtual Artificial Sensor Technique For Functional Electrical StimulationDocument11 pagesVirtual Artificial Sensor Technique For Functional Electrical StimulationCarlos Alexandre FerriNo ratings yet
- Wrist Movement Marker Placement for Daily Living ActivitiesDocument7 pagesWrist Movement Marker Placement for Daily Living ActivitiesAntarakata AmeilaningrumNo ratings yet
- 0.6 mm的最小分辨率滑动栅格Document11 pages0.6 mm的最小分辨率滑动栅格123No ratings yet
- The Teach'Wear - Healthcare Wearable DeviceDocument6 pagesThe Teach'Wear - Healthcare Wearable Devicedjole07No ratings yet
- 02.2.13 - Lealjunior2017 - HistereseDocument10 pages02.2.13 - Lealjunior2017 - HistereseRenan Costa LazaroNo ratings yet
- Cavallo - CAPESB 2021Document2 pagesCavallo - CAPESB 2021tanvir anwarNo ratings yet
- (Rehab Eng) Week #10 Assesment - Dina Andini - 5023201062Document4 pages(Rehab Eng) Week #10 Assesment - Dina Andini - 5023201062bringback happinesNo ratings yet
- Magalhes2013 Three DimensionalkinematicDocument3 pagesMagalhes2013 Three DimensionalkinematicAnkit1402No ratings yet
- Chia Bejarano Et Al. - 2014 - A Novel Adaptive, Real-Time Algorithm To Detect Gait Events From Wearable SensorsDocument10 pagesChia Bejarano Et Al. - 2014 - A Novel Adaptive, Real-Time Algorithm To Detect Gait Events From Wearable SensorsQxqNo ratings yet
- Range of Motion and Lordosis of The Lumbar SpineDocument8 pagesRange of Motion and Lordosis of The Lumbar SpinekhaledNo ratings yet
- Mathematics 11 00970Document17 pagesMathematics 11 00970TONY HII CHANG SOONNo ratings yet
- Automated Analysis Method For Screening Knee Osteoarthritis Using Medical Infrared ThermographyDocument7 pagesAutomated Analysis Method For Screening Knee Osteoarthritis Using Medical Infrared ThermographyRoman PopescuNo ratings yet
- Article in Press: Orthopaedics & Traumatology: Surgery & ResearchDocument6 pagesArticle in Press: Orthopaedics & Traumatology: Surgery & ResearchAren BizdikianNo ratings yet
- KINOVEA - Reliability of Kinovea® Software and AgreementDocument12 pagesKINOVEA - Reliability of Kinovea® Software and AgreementTiago MarcheseNo ratings yet
- (10920684 - Neurosurgical Focus) Percutaneous Pedicle Screw Fixation of The Lumbar SpineDocument9 pages(10920684 - Neurosurgical Focus) Percutaneous Pedicle Screw Fixation of The Lumbar Spineefancoolhand09No ratings yet
- Drift-Free Inertial Sensor-Based Joint Kinematics For Long-Trem Arbitrary MovementsDocument11 pagesDrift-Free Inertial Sensor-Based Joint Kinematics For Long-Trem Arbitrary MovementsXiaohan TangNo ratings yet
- Haig Is 2000Document9 pagesHaig Is 2000leviathan_brNo ratings yet
- Accuracy of EOS Imagining Technology in Comparison.94031Document18 pagesAccuracy of EOS Imagining Technology in Comparison.94031Mohammad KaramNo ratings yet
- 3D Human Gait Reconstruction and Monitoring Using Body-Worn Inertial Sensors and Kinematic ModelingDocument9 pages3D Human Gait Reconstruction and Monitoring Using Body-Worn Inertial Sensors and Kinematic ModelingCristian HoyNo ratings yet
- Using Convolutional Neural Network To Design and Predict The Forces and Kinematic Performance and External Rotation Moment of The Hip Joint in The PelvisDocument6 pagesUsing Convolutional Neural Network To Design and Predict The Forces and Kinematic Performance and External Rotation Moment of The Hip Joint in The PelvisInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Patterns of Spinal Motion During Walking: Jack Crosbie ", Roongtiwa Vachalathitib, Richard Smith"Document7 pagesPatterns of Spinal Motion During Walking: Jack Crosbie ", Roongtiwa Vachalathitib, Richard Smith"Patrik NazarioNo ratings yet
- Oke Esser2009 PrintDocument4 pagesOke Esser2009 PrintAnisa FauziahNo ratings yet
- Reliability and Validity of Ultrasound Imaging of Features of Knee Osteoarthritis in The CommunityDocument8 pagesReliability and Validity of Ultrasound Imaging of Features of Knee Osteoarthritis in The CommunityCaitlynNo ratings yet
- MEASURING HUMAN GAIT WITH A SIMPLE ELECTROGONIOMETRIC SYSTEMDocument3 pagesMEASURING HUMAN GAIT WITH A SIMPLE ELECTROGONIOMETRIC SYSTEMJosé Antonio Ruiz LópezNo ratings yet
- Reeves 2004Document3 pagesReeves 2004kinehtg6No ratings yet
- Sensors 22 09765Document18 pagesSensors 22 09765Jose Carlos NMNo ratings yet
- Assessment PDFDocument7 pagesAssessment PDFdrprasantNo ratings yet
- Gait Dynamics Sensing Using IMU Sensor Array System: Slavomir KARDOS, Peter BALOG, Stanislav SLOSARCIKDocument6 pagesGait Dynamics Sensing Using IMU Sensor Array System: Slavomir KARDOS, Peter BALOG, Stanislav SLOSARCIKMonikaNo ratings yet
- Wong 2007Document15 pagesWong 2007Somente CoisasNo ratings yet
- A Wearable Motion Capture Device Able To Detect Dynamic Motion of Human LimbsDocument12 pagesA Wearable Motion Capture Device Able To Detect Dynamic Motion of Human LimbsAhmed Gawad ElashryNo ratings yet
- In Vivo Three-Dimensional Kinematics of The Normal Knee DuringDocument9 pagesIn Vivo Three-Dimensional Kinematics of The Normal Knee DuringAngel LiconaNo ratings yet
- Mobile Sensor Application For Kinematic Detection of The KneesDocument10 pagesMobile Sensor Application For Kinematic Detection of The KneesVizaNo ratings yet
- Sensors: Real-Time Estimation of Pathological Tremor Parameters From Gyroscope DataDocument21 pagesSensors: Real-Time Estimation of Pathological Tremor Parameters From Gyroscope DataLuis Eduardo Romero MaldonadoNo ratings yet
- A Simple DeviceDocument6 pagesA Simple DeviceErna TamiziNo ratings yet
- Models For DC MotorsDocument8 pagesModels For DC MotorsebrahimpanNo ratings yet
- DC motor dynamic modeling and control techniquesDocument23 pagesDC motor dynamic modeling and control techniquesKaderNo ratings yet
- Yjmt 23 188Document9 pagesYjmt 23 188ebrahimpanNo ratings yet
- Solution 2Document5 pagesSolution 2Paulina MarquezNo ratings yet
- Sensors: Adaptive PIF Control For Permanent Magnet Synchronous Motors Based On GPCDocument18 pagesSensors: Adaptive PIF Control For Permanent Magnet Synchronous Motors Based On GPCebrahimpanNo ratings yet
- Open Sim Tutorial 1Document10 pagesOpen Sim Tutorial 1Rayanne FlorianoNo ratings yet
- Open Sim Tutorial 1Document10 pagesOpen Sim Tutorial 1Rayanne FlorianoNo ratings yet
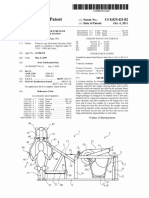
- United States Patent (10) Patent N6 US 8,029,424 B2: Thulin 45 Date of Patent: Oct. 4 2011Document15 pagesUnited States Patent (10) Patent N6 US 8,029,424 B2: Thulin 45 Date of Patent: Oct. 4 2011ebrahimpanNo ratings yet
- Adaptation of Multijoint Coordination During Standing Balance in Healthy Young and Healthy Old IndividualsDocument14 pagesAdaptation of Multijoint Coordination During Standing Balance in Healthy Young and Healthy Old IndividualsebrahimpanNo ratings yet
- I6 BrochureDocument2 pagesI6 BrochureebrahimpanNo ratings yet
- Spring Over Muscle (SOM) Actuator For Rehabilitation DevicesDocument4 pagesSpring Over Muscle (SOM) Actuator For Rehabilitation DevicesebrahimpanNo ratings yet
- Adaptation of Multijoint Coordination During Standing Balance in Healthy Young and Healthy Old IndividualsDocument14 pagesAdaptation of Multijoint Coordination During Standing Balance in Healthy Young and Healthy Old IndividualsebrahimpanNo ratings yet
- c3d2OpenSim TutorialDocument8 pagesc3d2OpenSim Tutorialebrahimpan100% (1)
- Mechatronics: Haoyong Yu, Sunan Huang, Gong Chen, Nitish ThakorDocument12 pagesMechatronics: Haoyong Yu, Sunan Huang, Gong Chen, Nitish ThakorebrahimpanNo ratings yet
- An Assisted Waist Supporter For Vertebral RehabilitationDocument2 pagesAn Assisted Waist Supporter For Vertebral RehabilitationebrahimpanNo ratings yet
- A Review of The Use of Electro-Motor Stimulation in Human MusclesDocument13 pagesA Review of The Use of Electro-Motor Stimulation in Human MusclesebrahimpanNo ratings yet
- Design and Implementation of A Distributed Variable Impedance Actuator Using Parallel Linear SpringsDocument12 pagesDesign and Implementation of A Distributed Variable Impedance Actuator Using Parallel Linear SpringsebrahimpanNo ratings yet
- Three-Dimensional Joint Reaction Forces and Moments at The Low Ba PDFDocument9 pagesThree-Dimensional Joint Reaction Forces and Moments at The Low Ba PDFebrahimpanNo ratings yet
- 100720141556121410000Document6 pages100720141556121410000ebrahimpanNo ratings yet
- A Review of The Clinical Value of Isolated Lumbar Extension Resistance Training For Chronic Low Back PainDocument19 pagesA Review of The Clinical Value of Isolated Lumbar Extension Resistance Training For Chronic Low Back PainebrahimpanNo ratings yet
- 100720141556121410000Document6 pages100720141556121410000ebrahimpanNo ratings yet
- Supported Contact Mechanics ModelsDocument8 pagesSupported Contact Mechanics ModelsebrahimpanNo ratings yet
- Hasegawa 1985Document6 pagesHasegawa 1985ebrahimpanNo ratings yet
- Viscoelasticity - RheologicalDocument10 pagesViscoelasticity - RheologicalsaltyNo ratings yet
- Strain CylindricalDocument4 pagesStrain CylindricalebrahimpanNo ratings yet
- Mca 21 00016 v2 PDFDocument15 pagesMca 21 00016 v2 PDFebrahimpanNo ratings yet
- Watanabe 2010Document4 pagesWatanabe 2010ebrahimpanNo ratings yet
- Elastic Constitutive EquationsDocument46 pagesElastic Constitutive EquationsAmithkumar R AchariNo ratings yet
- Plane Strain Problems of Transversely Isotropic Thermoelastic MediaDocument15 pagesPlane Strain Problems of Transversely Isotropic Thermoelastic MediaebrahimpanNo ratings yet
- Hasegawa 1985Document6 pagesHasegawa 1985ebrahimpanNo ratings yet
- Doctor's Book of Survival Home RemediesDocument8 pagesDoctor's Book of Survival Home RemediesLouay Dan0% (2)
- The Murmur - October 2014Document9 pagesThe Murmur - October 2014RyanLoveNo ratings yet
- Influence of Anthropometric Parameters On Aerobic Capacity Among DancersDocument7 pagesInfluence of Anthropometric Parameters On Aerobic Capacity Among DancersAnonymous izrFWiQNo ratings yet
- TCM FD 100-FD115-FD120-FD135-FD150s-FD160s HDDocument6 pagesTCM FD 100-FD115-FD120-FD135-FD150s-FD160s HDJoanneTauresia100% (1)
- Uganda Universities and Courses For Student Loan SupportDocument5 pagesUganda Universities and Courses For Student Loan SupportThe Campus TimesNo ratings yet
- NCP Escaran.Document3 pagesNCP Escaran.Roswell Almodiel EscaranNo ratings yet
- Learning To Manage Health Information: A Theme For Clinical EducationDocument48 pagesLearning To Manage Health Information: A Theme For Clinical EducationPatients Know Best100% (2)
- Understanding Diagnostic Test Accuracy and InterpretationDocument18 pagesUnderstanding Diagnostic Test Accuracy and InterpretationAnna GozaliNo ratings yet
- MTF Surgery KitDocument33 pagesMTF Surgery KitCarolyn Samuels75% (4)
- Annex To The European Commission Guideline On Excipients in The Labelling and Package Leaflet of Medicinal Products For Human Use' (2019)Document21 pagesAnnex To The European Commission Guideline On Excipients in The Labelling and Package Leaflet of Medicinal Products For Human Use' (2019)janoscribdNo ratings yet
- Spoon Project ProposalDocument10 pagesSpoon Project Proposalapi-286709781No ratings yet
- Plasticity in The Visual System - From Genes To Circuits - R. PinaudDocument366 pagesPlasticity in The Visual System - From Genes To Circuits - R. PinaudEliMihaelaNo ratings yet
- Types and Treatment of LeukemiaDocument14 pagesTypes and Treatment of LeukemiaalirezaNo ratings yet
- Case Study On Fluid OverloadDocument37 pagesCase Study On Fluid OverloadradicalmpNo ratings yet
- Understanding the language of our bodyDocument80 pagesUnderstanding the language of our bodyrajuhungudkarNo ratings yet
- Kinetics Problem Solving Set7-11.10.15Document13 pagesKinetics Problem Solving Set7-11.10.15Katrina Chan67% (3)
- MEDI7241 How To Write A Research Protocol TutorialDocument7 pagesMEDI7241 How To Write A Research Protocol TutorialJazradelNo ratings yet
- Henoch Schonlein Purpura (IgA Vasculitis)Document15 pagesHenoch Schonlein Purpura (IgA Vasculitis)Emily Eresuma100% (1)
- Price List All Disc SM - DSM 170622Document1 pagePrice List All Disc SM - DSM 170622Rhesa GuttamaNo ratings yet
- First Appeal Letter To The Pensions Tribunal June 2013Document10 pagesFirst Appeal Letter To The Pensions Tribunal June 2013Chris BusbyNo ratings yet
- Ancient Indian Women Who Shaped HistoryDocument1 pageAncient Indian Women Who Shaped HistoryNaveetha M ANo ratings yet
- Cagnie2013 Physiological Effects of Dry NeedlingDocument8 pagesCagnie2013 Physiological Effects of Dry NeedlingWahyu FathurrachmanNo ratings yet
- Kinds of Diseases: Name: Rebekha Noveria NPM: 18.11.124 PSIK 3.1Document12 pagesKinds of Diseases: Name: Rebekha Noveria NPM: 18.11.124 PSIK 3.1Rebekha Noveria SitumorangNo ratings yet
- Understanding Kundalini Energy and its Role in Spiritual EvolutionDocument190 pagesUnderstanding Kundalini Energy and its Role in Spiritual Evolutionnityanandroy100% (1)
- Syllabus For HAADDocument7 pagesSyllabus For HAADvirasamir100% (2)
- CPG Treatment of Periodontal AbscessDocument26 pagesCPG Treatment of Periodontal AbscessFirda Maulani MawardiNo ratings yet
- The Benefits of Nurse Prescribing Within Specialist Palliative CareDocument26 pagesThe Benefits of Nurse Prescribing Within Specialist Palliative CarejakkenjuNo ratings yet
- Herkin-3000 Skin Care System ManualDocument19 pagesHerkin-3000 Skin Care System ManualEnigma International IncNo ratings yet
- How to Safely Administer Eye Drops and OintmentsDocument3 pagesHow to Safely Administer Eye Drops and OintmentsDionicia Chandrika0% (1)
- Exploratory EssayDocument6 pagesExploratory Essayapi-252875204No ratings yet