You might also like
- Neurological Health AssessmentDocument63 pagesNeurological Health AssessmentAhmed ElryahNo ratings yet
- The Neurological Exam: Respect and Kindness. When You Enter TheDocument9 pagesThe Neurological Exam: Respect and Kindness. When You Enter TheRemelou Garchitorena Alfelor100% (1)
- Nervous System Examination SynopsisDocument26 pagesNervous System Examination Synopsisaarti chandeNo ratings yet
- Head To Toe AssessmentDocument22 pagesHead To Toe AssessmentNessa Layos MorilloNo ratings yet
- Neurological Assessment - Romeo RiveraDocument9 pagesNeurological Assessment - Romeo Riveraromeo riveraNo ratings yet
- Neuro 101: Nursing Neuro Assessment: Kristen Ankrom, RN, SCRN, CCCC Stroke Coordinator Coliseum Medical CentersDocument29 pagesNeuro 101: Nursing Neuro Assessment: Kristen Ankrom, RN, SCRN, CCCC Stroke Coordinator Coliseum Medical CentersDarvin MathewNo ratings yet
- Methods of ExaminationDocument53 pagesMethods of ExaminationTeodor ŞişianuNo ratings yet
- Assessment of The Nervous System - FinalDocument76 pagesAssessment of The Nervous System - FinalRona Lucido100% (1)
- Neurological Assessment: Alice E. Davis, PH.D., RNDocument6 pagesNeurological Assessment: Alice E. Davis, PH.D., RNdhekuh100% (2)
- Neurology Cram NotesDocument19 pagesNeurology Cram Notesrjh1895No ratings yet
- Neuro OSCE - Student Guide PDFDocument9 pagesNeuro OSCE - Student Guide PDFDAVE RYAN DELA CRUZ100% (1)
- OSCE Marksheet 1Document7 pagesOSCE Marksheet 1Elias PetrouNo ratings yet
- Superficial and Deep ReflexesDocument28 pagesSuperficial and Deep ReflexesShilpa SNo ratings yet
- Neurological Physical ExamDocument3 pagesNeurological Physical Examjyhn24No ratings yet
- Medrano Neuro Notes 2.0Document22 pagesMedrano Neuro Notes 2.0roldan pantojaNo ratings yet
- Wall Neuro 2010Document34 pagesWall Neuro 2010Kath Jacinto100% (1)
- CS Physical Exam ChecklistDocument7 pagesCS Physical Exam Checklistxuni cNo ratings yet
- The Neurological ExaminationDocument28 pagesThe Neurological ExaminationpremaNo ratings yet
- ASSESSMENT OF THE NERVOUS SYSTEM (230 NursDocument72 pagesASSESSMENT OF THE NERVOUS SYSTEM (230 Nursriya priyaNo ratings yet
- Neurological AssessmentDocument64 pagesNeurological AssessmentNEuRoLoGisT CoFFeeCuP95% (20)
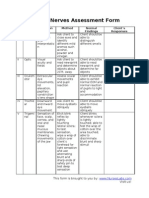
- Cranial Nerves Assessment FormDocument3 pagesCranial Nerves Assessment Formmhel03_chickmagnetNo ratings yet
- Latest Dr. Saleh Facial Nerve Applied 16.5.23Document85 pagesLatest Dr. Saleh Facial Nerve Applied 16.5.23Saleh Mohammad ShoaibNo ratings yet
- Muscle Tone and Reflex AssessmentDocument31 pagesMuscle Tone and Reflex Assessmentenrico_aguila100% (3)
- SeizureDocument3 pagesSeizureAJ Teoh50% (2)
- Neurological ExaminationDocument55 pagesNeurological ExaminationWasemBhatNo ratings yet
- Musculoskeletal Assessment: (10 Digit Number)Document5 pagesMusculoskeletal Assessment: (10 Digit Number)David Gomes0% (1)
- Cranial Nerves: General CharacteristicsDocument17 pagesCranial Nerves: General CharacteristicsRiki AntoNo ratings yet
- Use The Following Criteria in Evaluating The Skill PerformanceDocument4 pagesUse The Following Criteria in Evaluating The Skill Performancekookie100% (1)
- Neurological AssessmentDocument50 pagesNeurological Assessmentprabakaran9100% (3)
- Neuro Exam Checklist 2008Document2 pagesNeuro Exam Checklist 2008sara ashari100% (2)
- Neurological Examination of The Limbs TextDocument8 pagesNeurological Examination of The Limbs Textvidur_talrejaNo ratings yet
- Neurological Examination - BashaDocument8 pagesNeurological Examination - Bashakhaderbasha2020No ratings yet
- Neurological Exam Lecture NotesDocument26 pagesNeurological Exam Lecture NotesNaveen KovalNo ratings yet
- Neurological Assessment and Examination-1Document35 pagesNeurological Assessment and Examination-1Sarath KumarNo ratings yet
- Neurologic HistoryDocument68 pagesNeurologic HistoryMerahit AberaNo ratings yet
- Neurological ExaminationDocument240 pagesNeurological Examinationramadan0% (1)
- Neurological ExaminationDocument8 pagesNeurological Examinationg8048658No ratings yet
- YEAR 1 and 2 OSCE Revision: Author: DR Thomas PayneDocument30 pagesYEAR 1 and 2 OSCE Revision: Author: DR Thomas Payneminayoki100% (1)
- The Detailed Neurological Examination in Adults PDFDocument30 pagesThe Detailed Neurological Examination in Adults PDFOkenabirhieNo ratings yet
- Cranial Nerve AssessmentDocument4 pagesCranial Nerve AssessmentAnonymous h2EnKyDbNo ratings yet
- Pediatric Neurological ExaminationDocument5 pagesPediatric Neurological ExaminationbunnyronieNo ratings yet
- PNS Examination 15Document17 pagesPNS Examination 15NolanNo ratings yet
- Neuro Assessment: The Single Most Important AssessmentDocument10 pagesNeuro Assessment: The Single Most Important AssessmentpapadaadNo ratings yet
- Assessing The Thorax and LungsDocument3 pagesAssessing The Thorax and LungsZJ GarcianoNo ratings yet
- History Taking and Physical Examination - An Overview PDFDocument31 pagesHistory Taking and Physical Examination - An Overview PDFMarc Imhotep Cray, M.D.No ratings yet
- HemiplegiaDocument30 pagesHemiplegiasarguss14100% (1)
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Case Based Pediatrics CEREBRAL PALSYDocument5 pagesCase Based Pediatrics CEREBRAL PALSYNabighah ZukriNo ratings yet
- OSCE Cerebellar Examination PDFDocument6 pagesOSCE Cerebellar Examination PDFriczen vilaNo ratings yet
- Cerebellar DisordersDocument29 pagesCerebellar DisordersArslan Aslam100% (1)
- Focused Neurological AssessmentDocument23 pagesFocused Neurological AssessmentNabil Abd El-tawab100% (1)
- Ascending TractsDocument42 pagesAscending TractsJustine Nyangaresi100% (2)
- Neurology ARCP Decision Aid 2014Document1 pageNeurology ARCP Decision Aid 2014LingNo ratings yet
- Upper Motor Neuron Vs Lower Motor Neuron AtfDocument4 pagesUpper Motor Neuron Vs Lower Motor Neuron AtfRishi VermaNo ratings yet
- Neurology Exam Checklist1Document6 pagesNeurology Exam Checklist1Syed AfzalNo ratings yet
- Examination of The Peripheral Neurological SystemDocument2 pagesExamination of The Peripheral Neurological Systemkenners100% (12)
- 2017 Neuromuscular Pimp SheetDocument30 pages2017 Neuromuscular Pimp SheetAng LiNo ratings yet
- Neurology Shifting Exam: CnvandcnviiDocument9 pagesNeurology Shifting Exam: CnvandcnviicarlosNo ratings yet
- Cranial Nerve Examination Part IDocument91 pagesCranial Nerve Examination Part IAARYA100% (1)
- Sub - Medical Surgical Nursing: Assignment On Neurological AssessmentDocument11 pagesSub - Medical Surgical Nursing: Assignment On Neurological Assessmentkamini Choudhary100% (1)
- Comparison of The Clinical Effectiveness of PFNADocument8 pagesComparison of The Clinical Effectiveness of PFNAApolinar González HernándezNo ratings yet
- Principles of Fracture FixationDocument12 pagesPrinciples of Fracture FixationApolinar González HernándezNo ratings yet
- Small Incision Total Hip Replacement by The Lateral Approach Using Standard InstrumentsDocument5 pagesSmall Incision Total Hip Replacement by The Lateral Approach Using Standard InstrumentsApolinar González HernándezNo ratings yet
- Forearm Fractures FinalDocument8 pagesForearm Fractures FinalApolinar González HernándezNo ratings yet
- Abortive HIV Infection Mediates CD4 T-Cell Depletion and Inflammation in Human Lymphoid TissueDocument23 pagesAbortive HIV Infection Mediates CD4 T-Cell Depletion and Inflammation in Human Lymphoid TissueApolinar González HernándezNo ratings yet
- Blog MMTDocument4 pagesBlog MMTapi-336259983No ratings yet
- 4443-Multiple Choice Questions in Orthopaedics and TraumaDocument32 pages4443-Multiple Choice Questions in Orthopaedics and TraumaAhmed ALi100% (1)
- Time Travel Hypnosis Hi This Is Author Himani VashishtaDocument30 pagesTime Travel Hypnosis Hi This Is Author Himani VashishtaManoj Gaur50% (2)
- TanginaDocument25 pagesTanginaJasmin CobillaNo ratings yet
- Ushtrime Per BarkunDocument10 pagesUshtrime Per BarkunLuis SweetNo ratings yet
- Boxing by Philadelphia Jack OBrienDocument260 pagesBoxing by Philadelphia Jack OBrienSilver Sentinel100% (1)
- Unit 7 Ex 5-12Document5 pagesUnit 7 Ex 5-12Cosmina CorbeanuNo ratings yet
- Anatomy For 3D Artists - Scott EatonDocument4 pagesAnatomy For 3D Artists - Scott EatonDang AntheaNo ratings yet
- Orthopaedic Intruments and Surgeries: DR Tejasvi Agarwal Senior Resident Dept of OrthopaedicsDocument43 pagesOrthopaedic Intruments and Surgeries: DR Tejasvi Agarwal Senior Resident Dept of OrthopaedicsKapil LakhwaraNo ratings yet
- Peripheral Nerve Injuries - Medical ApplicationsDocument103 pagesPeripheral Nerve Injuries - Medical ApplicationsJune Epe100% (1)
- 2-Address SetupDocument38 pages2-Address SetupTran xuan ThuyNo ratings yet
- Upper Limb-MCQ With AnswersDocument20 pagesUpper Limb-MCQ With AnswersMatt McCannNo ratings yet
- 3D Total's Introduction To Rigging MAYADocument42 pages3D Total's Introduction To Rigging MAYATommy GunnNo ratings yet
- D&D 4e - Combat Essentials 1 - Critical Matters PDFDocument61 pagesD&D 4e - Combat Essentials 1 - Critical Matters PDFbumberto19No ratings yet
- SFMA Shoulder Corrective Exercises PDFDocument9 pagesSFMA Shoulder Corrective Exercises PDFamirreza jmNo ratings yet
- Walking AidsDocument38 pagesWalking AidsMurad KurdiNo ratings yet
- John Meadows - Program 10 - The DevourerDocument96 pagesJohn Meadows - Program 10 - The DevourerFran93% (15)
- Chart Bodyblade Exercise Wall ChartDocument1 pageChart Bodyblade Exercise Wall ChartJ.w. Laster100% (1)
- Fugl-Meyer Assessment Upper Extremity (Fma-Ue) Assessment of Sensorimotor FunctionDocument3 pagesFugl-Meyer Assessment Upper Extremity (Fma-Ue) Assessment of Sensorimotor FunctionFlorin MarinescuNo ratings yet
- The Detailed Neurological Examination in Adults PDFDocument30 pagesThe Detailed Neurological Examination in Adults PDFOkenabirhieNo ratings yet
- Rangkuman by Yulia VionitaDocument21 pagesRangkuman by Yulia VionitaRizqi AkbarNo ratings yet
- Summary Highlights of Yoga Secrets For Extraordinary Health and Long Life by Frank Rudolph YoungDocument62 pagesSummary Highlights of Yoga Secrets For Extraordinary Health and Long Life by Frank Rudolph Youngfmntime100% (7)
- Physiotools SusanDocument4 pagesPhysiotools Susanapi-658308760No ratings yet
- Manual Resistance ExercisesDocument12 pagesManual Resistance ExercisesTes TingNo ratings yet
- Module3 G7-8 Dressmaking ManaoagnhsDocument9 pagesModule3 G7-8 Dressmaking Manaoagnhsmichael segundoNo ratings yet
- The Skeleton: Chapter 7 Part CDocument73 pagesThe Skeleton: Chapter 7 Part CDon KeyNo ratings yet
- Kinetic Chain ArticleDocument9 pagesKinetic Chain Articler.zaczek93No ratings yet
- Current Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiDocument8 pagesCurrent Concepts in Elbow Fracture Dislocation: Adam C Watts, Jagwant Singh, Michael Elvey and Zaid HamoodiJoão Artur BonadimanNo ratings yet
- The Channels of AcupunctureDocument18 pagesThe Channels of AcupunctureFonnie OnesixthreeNo ratings yet
- Biomechanics Important QuestionsDocument11 pagesBiomechanics Important QuestionsHarshiya ChintuNo ratings yet