You might also like
- Lokesh Patil (22) - Madhura Jagtap (10) - Animesh Amal (01) - Vishal Mehta (16) - Khushbu MascarenhasDocument44 pagesLokesh Patil (22) - Madhura Jagtap (10) - Animesh Amal (01) - Vishal Mehta (16) - Khushbu MascarenhasWadud Mohammad OviNo ratings yet
- Treatment of TB in Adults: by Dr. Irfhan Ali Hyder AliDocument45 pagesTreatment of TB in Adults: by Dr. Irfhan Ali Hyder AliInspireGutsNo ratings yet
- Lokesh Patil (22) - Madhura Jagtap (10) - Animesh Amal (01) - Vishal Mehta (16) - Khushbu MascarenhasDocument44 pagesLokesh Patil (22) - Madhura Jagtap (10) - Animesh Amal (01) - Vishal Mehta (16) - Khushbu MascarenhasAnonymous 75aETJ8ONo ratings yet
- Childhood Vitiligo: Response To Methylprednisolone Oral Minipulse Therapy and Topical Fluticasone CombinationDocument5 pagesChildhood Vitiligo: Response To Methylprednisolone Oral Minipulse Therapy and Topical Fluticasone CombinationFebniNo ratings yet
- Basic Pharmacology: NTA Level 4 Semester 2Document12 pagesBasic Pharmacology: NTA Level 4 Semester 2MabusiNo ratings yet
- แนวทางการรักษาโรคมะเร็งเต้านมด้วยยาDocument66 pagesแนวทางการรักษาโรคมะเร็งเต้านมด้วยยาMawin VongsaisuwonNo ratings yet
- Strategies To Developing An Institutional Program To Enhance Antimicrobial StewardshipDocument32 pagesStrategies To Developing An Institutional Program To Enhance Antimicrobial StewardshipponekNo ratings yet
- 8-Kefpod 06Document35 pages8-Kefpod 06kurutalaNo ratings yet
- Trimethoprim With Sulfamethoxazole (Co-Trimoxazole) Monograph - PaediatricDocument7 pagesTrimethoprim With Sulfamethoxazole (Co-Trimoxazole) Monograph - PaediatricKnowledge UshambaNo ratings yet
- Contraception Questions and Answers For PharmacistsDocument9 pagesContraception Questions and Answers For PharmacistsMohamed OmerNo ratings yet
- Clinical Pharmacology of Anti-Cancer Chemotherapeutic AgentsDocument29 pagesClinical Pharmacology of Anti-Cancer Chemotherapeutic AgentsZarish IftikharNo ratings yet
- Ema-Co Gy GTDDocument4 pagesEma-Co Gy GTDTowhidulIslamNo ratings yet
- Rational Use of Abx-ICUDocument46 pagesRational Use of Abx-ICUYosef AssefaNo ratings yet
- DrugsDocument1 pageDrugsKamakshi GuptaNo ratings yet
- AmBisome - Package InsertDocument31 pagesAmBisome - Package InsertKatherine Silva MejíaNo ratings yet
- Antibiotic & Antiseptic Use in Periodontal TherapyDocument55 pagesAntibiotic & Antiseptic Use in Periodontal TherapyCristina EneNo ratings yet
- LectureDocument29 pagesLectureRiyazuddin MohammedNo ratings yet
- Medical Management of MucormycosisDocument19 pagesMedical Management of MucormycosisNayan GuptaNo ratings yet
- Leukemia Treatment Regimens 7937Document3 pagesLeukemia Treatment Regimens 7937Irfan FathurrahmanNo ratings yet
- Mu CostaDocument6 pagesMu Costafarracholidia_867630No ratings yet
- Azithromycin Monograph - PaediatricDocument7 pagesAzithromycin Monograph - PaediatrictynNo ratings yet
- MTOR-Inhibitors - Switch From CNI: Commercially Available DrugsDocument3 pagesMTOR-Inhibitors - Switch From CNI: Commercially Available DrugshassanNo ratings yet
- Uji ToksisitasDocument38 pagesUji ToksisitasAlunaficha Melody KiraniaNo ratings yet
- AntibioticsDocument122 pagesAntibioticsdentistry24100% (1)
- Practical Aspects of Antibiotic Selection: Debbie Tristram, MD Professor of Pediatrics Albany Medical CollegeDocument52 pagesPractical Aspects of Antibiotic Selection: Debbie Tristram, MD Professor of Pediatrics Albany Medical Collegest_arjunaNo ratings yet
- Anti-Tuberculosis Treatment: DR Wong VF Sibu GH 27/7/2013Document27 pagesAnti-Tuberculosis Treatment: DR Wong VF Sibu GH 27/7/2013Widy StefannyNo ratings yet
- Name Mucosta Tablets 100 Description PDFDocument7 pagesName Mucosta Tablets 100 Description PDFnanda RaharjaNo ratings yet
- ChemotherapyDocument102 pagesChemotherapyJoseph John K Pothanikat100% (1)
- PK&PD Susceptibility Course 2010Document44 pagesPK&PD Susceptibility Course 2010tanty_ukNo ratings yet
- Tuberculosis Treatment, MDR, XDR, Resistance, Prophylaxis, VaccinationDocument44 pagesTuberculosis Treatment, MDR, XDR, Resistance, Prophylaxis, Vaccinationskeisham11No ratings yet
- M BoelaertDocument20 pagesM BoelaertphilomenebouchonNo ratings yet
- Ferron Glumin XRDocument22 pagesFerron Glumin XRhilmayuniarNo ratings yet
- Antibiotic's Interactions in GynecologyDocument26 pagesAntibiotic's Interactions in Gynecologyمحمد قاسمNo ratings yet
- Drugs Used in Pediatric DentistryDocument33 pagesDrugs Used in Pediatric Dentistryaamee9690% (10)
- Proposal For The Inclusion of Anti-Emetic Medications (For Children) in The Who Model List of Essential MedicinesDocument44 pagesProposal For The Inclusion of Anti-Emetic Medications (For Children) in The Who Model List of Essential MedicinesJennifer FaustinNo ratings yet
- Development of Treatment: How Do We Manage Antimicrobial Resistance?Document22 pagesDevelopment of Treatment: How Do We Manage Antimicrobial Resistance?ellya theresiaNo ratings yet
- Vonoprazan Tablets SMPCDocument24 pagesVonoprazan Tablets SMPCMoussa Amer100% (1)
- Ovarian Germ Cell Tumors: Executive SummaryDocument7 pagesOvarian Germ Cell Tumors: Executive SummaryMuhammad Ferhat E.S.No ratings yet
- Treating TB in AdultsDocument15 pagesTreating TB in AdultsMeenakshianandi KrishnanNo ratings yet
- Adolescentes BFM HyperCVAD Alacacioglu2015Document5 pagesAdolescentes BFM HyperCVAD Alacacioglu2015erickmattosNo ratings yet
- BioconDocument7 pagesBioconsidhanti1993No ratings yet
- CASENGHI, Buruli Ulcer FINAL - WatermarkedDocument1 pageCASENGHI, Buruli Ulcer FINAL - WatermarkedjackstewartbriggsNo ratings yet
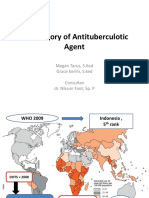
- 1 Category of Antituberculotic Agent: Megan Tarus, S.Ked Grace Kerihi, S.ked Consultan Dr. Nikson Faot, Sp. PDocument10 pages1 Category of Antituberculotic Agent: Megan Tarus, S.Ked Grace Kerihi, S.ked Consultan Dr. Nikson Faot, Sp. PAzrell Albert JonesNo ratings yet
- Anticancer DrugsDocument57 pagesAnticancer Drugsn4pnjfk6rbNo ratings yet
- JR 3 Dr. Danisa Edit - Efficacy and Safety of 250 MG Versus 500 MG Oral Terbinafine in The TreatmeDocument13 pagesJR 3 Dr. Danisa Edit - Efficacy and Safety of 250 MG Versus 500 MG Oral Terbinafine in The Treatmedanisa.dvjuli23No ratings yet
- Biochemistry Reagents - ITA Kits - Promotional Tool 27th - August-2019-2Document23 pagesBiochemistry Reagents - ITA Kits - Promotional Tool 27th - August-2019-2Ajay DataniyaNo ratings yet
- A Novel Breakthrough For BCCDocument16 pagesA Novel Breakthrough For BCC88AKKNo ratings yet
- Pediatric Health Nursing Unit-Iii Pharmacological Care Aspects While Dealing With Pediatric PatientsDocument107 pagesPediatric Health Nursing Unit-Iii Pharmacological Care Aspects While Dealing With Pediatric PatientsPriya bhatti0% (1)
- ADPTBDocument41 pagesADPTBHarlinda myraNo ratings yet
- Nahdi Pharma FileDocument477 pagesNahdi Pharma FileSarah JeanNo ratings yet
- Cetuximab-200mg Per 100ml InjectionDocument17 pagesCetuximab-200mg Per 100ml InjectionMd. Abdur RahmanNo ratings yet
- Antibacterial Therapy of MastitisDocument10 pagesAntibacterial Therapy of MastitisSunil100% (2)
- Aminogycoside AntibioticsDocument31 pagesAminogycoside AntibioticsNurul Febrina100% (2)
- Optimizing Aminoglycosideuse: William A. CraigDocument15 pagesOptimizing Aminoglycosideuse: William A. CraigSurya BhupatirajuNo ratings yet
- Antimicrobial StewardshipDocument40 pagesAntimicrobial StewardshipChestnutNo ratings yet
- Farmakologi Dan Toksikologi 2 PDFDocument11 pagesFarmakologi Dan Toksikologi 2 PDFDewiScintaNo ratings yet
- Stromectol PiDocument7 pagesStromectol PiZainul AnwarNo ratings yet
- Bcbs Prov Guid ZofranDocument3 pagesBcbs Prov Guid ZofranAlvinHadisaputraNo ratings yet
- Antimicrobial Therapy in Veterinary MedicineFrom EverandAntimicrobial Therapy in Veterinary MedicineSteeve GiguèreRating: 4 out of 5 stars4/5 (1)
- Bird FluDocument5 pagesBird FluNader SmadiNo ratings yet
- Protocols Socra PetrosDocument47 pagesProtocols Socra Petrosthamizh555No ratings yet
- Critical Thinking ExamplesDocument4 pagesCritical Thinking ExamplesStacy WalkerNo ratings yet
- Walgreen Online PharmacyDocument64 pagesWalgreen Online PharmacyWalgreen Online PharmacyNo ratings yet
- Endometritis: R.N. Zainab Neamat JumaahDocument19 pagesEndometritis: R.N. Zainab Neamat JumaahKevin Adrian WijayaNo ratings yet
- Fundamentals of NursingDocument220 pagesFundamentals of NursingdgratyNo ratings yet
- Coronal Microleakage of Various Temporary Fillings in Endodontic AccessçDocument6 pagesCoronal Microleakage of Various Temporary Fillings in Endodontic Accessçjhon HanselNo ratings yet
- Tema: Personal Information: Escuela Profesional de EnfermeríaDocument21 pagesTema: Personal Information: Escuela Profesional de EnfermeríaPamela Ballon SotoNo ratings yet
- Evidence Based MedicineDocument55 pagesEvidence Based MedicineHelen SusantoNo ratings yet
- Badanie MMRDocument8 pagesBadanie MMRAgaryNo ratings yet
- Feline PanleukopeniaDocument15 pagesFeline PanleukopeniaVetlife DvpNo ratings yet
- Evaluacion Ingles Constanza Jarpa Aedo 7mo Basico UlaDocument4 pagesEvaluacion Ingles Constanza Jarpa Aedo 7mo Basico UlaCaterine Aedo BerrocalNo ratings yet
- Nursing GeneralDocument320 pagesNursing GeneralKrishnamoorthy GurumoorthyNo ratings yet
- Litrature & Case StudyDocument74 pagesLitrature & Case Studynaol buloNo ratings yet
- Pneumonia in Children: IAP UG Teaching Slides 2015 16Document28 pagesPneumonia in Children: IAP UG Teaching Slides 2015 16Ananya Anaparthi100% (1)
- DystociaDocument17 pagesDystociaKarinaNo ratings yet
- Acbid 2018Document360 pagesAcbid 2018Nelli YıldırımyanNo ratings yet
- PMDC Indexed JournalsDocument2 pagesPMDC Indexed JournalsMuhammad Asif NaveedNo ratings yet
- Andre SaineDocument4 pagesAndre Sainebuscador0077No ratings yet
- Obstetric Fistula A Preventable TragedyDocument9 pagesObstetric Fistula A Preventable TragedysrterduNo ratings yet
- Polycystic Ovary Syndrome (PCOS) : February 2020Document5 pagesPolycystic Ovary Syndrome (PCOS) : February 2020Lia MeivianeNo ratings yet
- Chapter 41 - Hepatitis VirusesDocument22 pagesChapter 41 - Hepatitis VirusesBibi Rabiah NoorNo ratings yet
- Family Nursing Care PlanDocument5 pagesFamily Nursing Care PlanCharmaine Cajayon69% (16)
- World Osteoporosis Day - 16 October 2022Document2 pagesWorld Osteoporosis Day - 16 October 2022Times MediaNo ratings yet
- Soal KISI-KISI. UAS - NE.II. Smter.V.Jan.'20'Document9 pagesSoal KISI-KISI. UAS - NE.II. Smter.V.Jan.'20'STIKES Yarsi MataramNo ratings yet
- Nursing Education: Rating ScaleDocument5 pagesNursing Education: Rating Scalemerin sunil100% (2)
- Psyc 3151Document6 pagesPsyc 3151essay4all100% (2)
- FIA Meter: Fluorescence Immunoassay Rapid Quantitative TestDocument2 pagesFIA Meter: Fluorescence Immunoassay Rapid Quantitative TestJM Umayam100% (1)
- Implementation of New Rostered Routine Testing (RRT) RegimeDocument5 pagesImplementation of New Rostered Routine Testing (RRT) RegimeSen MuruNo ratings yet
- Inverted Nipples PDFDocument2 pagesInverted Nipples PDFfifahcantikNo ratings yet