You might also like
- Doping in SportDocument13 pagesDoping in SportFaizeen RazakNo ratings yet
- Doping in SportsDocument9 pagesDoping in Sportsursvenki4ever3793No ratings yet
- Wyoming Outfitter DirectoryDocument56 pagesWyoming Outfitter Directorynordkapp3No ratings yet
- Doping, Performance-Enhancing Drugs, and Hormones in Sport: Mechanisms of Action and Methods of DetectionFrom EverandDoping, Performance-Enhancing Drugs, and Hormones in Sport: Mechanisms of Action and Methods of DetectionRating: 5 out of 5 stars5/5 (1)
- Material Inventory ListingDocument147 pagesMaterial Inventory ListingFelipe Gamboa GálvezNo ratings yet
- Dynamics of Rigid Bodies (4th Year)Document2 pagesDynamics of Rigid Bodies (4th Year)Jaypee CalambaNo ratings yet
- Doping in Sport: A HistoryDocument4 pagesDoping in Sport: A Historyiilm002No ratings yet
- Hormonal Doping and Androgenization of Athletes: A Secret Program of The German Democratic Republic GovernmentDocument18 pagesHormonal Doping and Androgenization of Athletes: A Secret Program of The German Democratic Republic GovernmentAdrian Moreno100% (2)
- SEM636 Parts Manual OverviewDocument185 pagesSEM636 Parts Manual OverviewRicardo Barreto100% (1)
- Doping PDFDocument10 pagesDoping PDFYulisbet HutapeaNo ratings yet
- Three Little PigsDocument29 pagesThree Little PigsSalman Valerio Delfin100% (1)
- Vazao Bicos TcnomotorDocument5 pagesVazao Bicos TcnomotorLuis Otavio GuimaraesNo ratings yet
- DopingDocument5 pagesDopingTamara ArsicNo ratings yet
- Doping in SportsDocument3 pagesDoping in SportsDanica Marie RegaladoNo ratings yet
- Research Paper Sports Law Tia SachdevaDocument8 pagesResearch Paper Sports Law Tia SachdevaTia SachdevaNo ratings yet
- Enha Ncement Drugs Andtheathlete: Francesco Botr E, Antonio PavanDocument16 pagesEnha Ncement Drugs Andtheathlete: Francesco Botr E, Antonio PavanDanijel DamnjanovicNo ratings yet
- Debate Is Drugs Testing in Athletes JustifiedDocument2 pagesDebate Is Drugs Testing in Athletes JustifiedCristianNo ratings yet
- Uhv ReportDocument25 pagesUhv ReportBiancaa RNo ratings yet
- Doping Short VersionDocument3 pagesDoping Short VersionSaber NouiraNo ratings yet
- Pharmacy: Exploring Knowledge, Attitudes and Abuse Concerning Doping in Sport Among Syrian Pharmacy StudentsDocument13 pagesPharmacy: Exploring Knowledge, Attitudes and Abuse Concerning Doping in Sport Among Syrian Pharmacy Studentssome buddyyNo ratings yet
- Torts Project MasudaDocument18 pagesTorts Project MasudaPratham MohantyNo ratings yet
- The Sports Doping ShenaniganDocument5 pagesThe Sports Doping ShenaniganYash BhatnagarNo ratings yet
- Doping in SportsDocument6 pagesDoping in SportsAli ApaydınNo ratings yet
- Trabajo de Fin de Grado sobre el dopajeDocument28 pagesTrabajo de Fin de Grado sobre el dopajeMarta AntunezNo ratings yet
- Anabolic Steroids-BDocument5 pagesAnabolic Steroids-BGideon MurathaNo ratings yet
- Sports Doping Review ArticleDocument11 pagesSports Doping Review ArticleRITESH MADRECHANo ratings yet
- Drugs in SportDocument14 pagesDrugs in Sportnor_nadiah_4No ratings yet
- Anti-Doping and Sports LawDocument14 pagesAnti-Doping and Sports LawNamisha ChoudharyNo ratings yet
- Critical Thinking Paper FinalDocument8 pagesCritical Thinking Paper Finalabeselomgcap2017No ratings yet
- BR J Sports Med 1975 Articles 58 9Document3 pagesBR J Sports Med 1975 Articles 58 9samawayNo ratings yet
- Top 10 Pros and ConsDocument5 pagesTop 10 Pros and ConsAmirul ShamNo ratings yet
- Development of Doping in Sports: Overview and Analysis: Original ArticleDocument9 pagesDevelopment of Doping in Sports: Overview and Analysis: Original ArticleshendiNo ratings yet
- The Role of The Pharmacist in The Fight Against Doping in SportDocument4 pagesThe Role of The Pharmacist in The Fight Against Doping in SportVanessa SoaresNo ratings yet
- Dopinginsportsop EdDocument2 pagesDopinginsportsop Edapi-356118919No ratings yet
- Drugs and Athletes Thesis StatementDocument7 pagesDrugs and Athletes Thesis Statementcassandrasirateantioch100% (2)
- Doping 1Document4 pagesDoping 1Martin RozsaNo ratings yet
- Research Paper Drug Abuse in AthletesDocument17 pagesResearch Paper Drug Abuse in Athletesnjerunick3060No ratings yet
- Sport and Human Rights and WrongsDocument3 pagesSport and Human Rights and WrongsMark AnidNo ratings yet
- Persuasive Essay Final DraftDocument13 pagesPersuasive Essay Final Draftapi-3003748650% (1)
- Mwa 2Document15 pagesMwa 2api-645226608No ratings yet
- This House Would Permit The Use of Performance Enhancing Drugs in Professional SportsDocument7 pagesThis House Would Permit The Use of Performance Enhancing Drugs in Professional Sportssamimi binti abdul rahmanNo ratings yet
- Drugs in Sport Info BriefDocument6 pagesDrugs in Sport Info BriefAbdul Razak MansorNo ratings yet
- Performance Enhancing Drugs in Sport PDFDocument15 pagesPerformance Enhancing Drugs in Sport PDFZishan DrNo ratings yet
- Anti-Doping Laws for CricketersDocument12 pagesAnti-Doping Laws for Cricketerssaurav singhNo ratings yet
- Doping in Sports: Current Review: April 2013Document5 pagesDoping in Sports: Current Review: April 2013RITESH MADRECHANo ratings yet
- 10 DopinginsportsIJCRRDocument5 pages10 DopinginsportsIJCRRZunaira YasinNo ratings yet
- Literature Review Drugs in SportDocument7 pagesLiterature Review Drugs in Sportc5nr2r46100% (1)
- A Review of Anti-Doping Policies Prior To The Formation of The World Anti-Doping AgencyDocument7 pagesA Review of Anti-Doping Policies Prior To The Formation of The World Anti-Doping AgencyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Sluggett - Creating The Pure AthleteDocument61 pagesSluggett - Creating The Pure AthleteKen YuNo ratings yet
- Substances that harm athletes-DopingDocument4 pagesSubstances that harm athletes-DopingkugaugafNo ratings yet
- Test PDFDocument2 pagesTest PDFAmir FazelNo ratings yet
- History of Drug Use in SportDocument7 pagesHistory of Drug Use in SportJose Páez MaldonadoNo ratings yet
- How Performance Enhancing Drugs Are Affecting Sport Individual InvestigationDocument6 pagesHow Performance Enhancing Drugs Are Affecting Sport Individual InvestigationChristina ThomasNo ratings yet
- Persuasive Essay: Performance-Enhancing Drugs Should Not Be Allowed in SportsDocument6 pagesPersuasive Essay: Performance-Enhancing Drugs Should Not Be Allowed in Sportsjulius wambuiNo ratings yet
- AdamasDocument46 pagesAdamasMuhammad AriffuddinNo ratings yet
- Over A Very Long Period of TimeDocument2 pagesOver A Very Long Period of TimeLorenz GonzaloNo ratings yet
- DopingDocument3 pagesDopingumesh pradhanNo ratings yet
- Original Article Development of Doping in Sports: Overview and AnalysisDocument12 pagesOriginal Article Development of Doping in Sports: Overview and AnalysisChristine StevanyNo ratings yet
- Anabolic SteroidsDocument5 pagesAnabolic SteroidsGideon MurathaNo ratings yet
- Research Paper On Drug Abuse in SportsDocument6 pagesResearch Paper On Drug Abuse in Sportsgw0gbrwe100% (1)
- Unit - 2 - Dope TestingDocument25 pagesUnit - 2 - Dope TestingMuskaan BindalNo ratings yet
- 05 18.03 WoS Doping PDFDocument4 pages05 18.03 WoS Doping PDFfesamacsNo ratings yet
- Sports Medicine & Doping Studies: Exercise, Science and Designer Doping: Traditional and Emerging TrendsDocument9 pagesSports Medicine & Doping Studies: Exercise, Science and Designer Doping: Traditional and Emerging TrendsDanijel DamnjanovicNo ratings yet
- Should Doping Be Prohibated in SportsDocument6 pagesShould Doping Be Prohibated in SportsMurtaza IbrahimiNo ratings yet
- Thesis On Drugs in SportsDocument4 pagesThesis On Drugs in SportsLori Head100% (2)
- Download Fitness Doping Trajectories Gender Bodies And Health 1St Ed Edition Jesper Andreasson full chapterDocument67 pagesDownload Fitness Doping Trajectories Gender Bodies And Health 1St Ed Edition Jesper Andreasson full chapterlina.philpott914100% (7)
- CH 02Document65 pagesCH 02elizabetaNo ratings yet
- 1 2Document5 pages1 2elizabetaNo ratings yet
- THU Obje ParcijaleDocument14 pagesTHU Obje ParcijaleelizabetaNo ratings yet
- Naslov PDFDocument1 pageNaslov PDFelizabetaNo ratings yet
- CH 01Document59 pagesCH 01elizabetaNo ratings yet
- W3 Needs AnalysisDocument11 pagesW3 Needs AnalysiselizabetaNo ratings yet
- W4 Language Systems and Language UsesDocument18 pagesW4 Language Systems and Language UseselizabetaNo ratings yet
- W6 Conditions For LearningDocument12 pagesW6 Conditions For LearningelizabetaNo ratings yet
- W2 Objectives of ESPDocument8 pagesW2 Objectives of ESPelizabetaNo ratings yet
- Katalog - Engleski Jez - OsDocument71 pagesKatalog - Engleski Jez - OsAlmir UstamujićNo ratings yet
- W1 Introduction To ESPDocument8 pagesW1 Introduction To ESPelizabetaNo ratings yet
- 19Document25 pages19elizabetaNo ratings yet
- 16Document25 pages16elizabetaNo ratings yet
- Adjectives ending in 'ing' or 'ed' - describing things, situations and feelingsDocument1 pageAdjectives ending in 'ing' or 'ed' - describing things, situations and feelingselizabetaNo ratings yet
- 1Document1 page1elizabetaNo ratings yet
- Sura Ya - Sin PrijevodDocument4 pagesSura Ya - Sin PrijevodelizabetaNo ratings yet
- HG Lab 7 - FinalDocument5 pagesHG Lab 7 - FinalelizabetaNo ratings yet
- Manual de Despiece Cruiser 250Document43 pagesManual de Despiece Cruiser 250leanroy1130% (1)
- SamiDocument29 pagesSamiSarra ChoucheneNo ratings yet
- Carico PDF 276001 2014 1574161 51 54Document80 pagesCarico PDF 276001 2014 1574161 51 54FLAMENCO COMPANY LTD.No ratings yet
- Section Officer Practice GK Set 2 For NepalDocument7 pagesSection Officer Practice GK Set 2 For NepalSaugat timilsinaNo ratings yet
- WMKK PDFDocument78 pagesWMKK PDFJustin OngNo ratings yet
- Nyssra Sprint Biathlon ChampionshipDocument8 pagesNyssra Sprint Biathlon ChampionshipRyan ScottNo ratings yet
- Da Annex10-04-19Document10 pagesDa Annex10-04-19Some GuyNo ratings yet
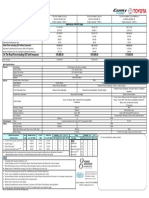
- Camry - PricelistDocument1 pageCamry - PricelistIdris AhmadNo ratings yet
- From The TubeDocument275 pagesFrom The TubePcnhs SalNo ratings yet
- Multiplex Project Proposal: Duo Spar / Gang Spar / Gang TTS / Base BattleDocument9 pagesMultiplex Project Proposal: Duo Spar / Gang Spar / Gang TTS / Base BattlePatrick PhillipsNo ratings yet
- m8 Dirtywave GuideDocument1 pagem8 Dirtywave Guidekqwt2z8qcxNo ratings yet
- WORKOUT Forza e Potenza 8-12 SettimaneDocument5 pagesWORKOUT Forza e Potenza 8-12 SettimaneGiovanni Delli SantiNo ratings yet
- Mercedes 1735 (WT-16)Document2 pagesMercedes 1735 (WT-16)nalanliyanage008No ratings yet
- PC - PRINT - 14-04-33 Engine Cylinder Head UN TR 117Document3 pagesPC - PRINT - 14-04-33 Engine Cylinder Head UN TR 117yugopuspoyoNo ratings yet
- AKSESOUAR - ΚΑΘΗΣΜΑΤΑ GERMANYDocument15 pagesAKSESOUAR - ΚΑΘΗΣΜΑΤΑ GERMANYinfo7879No ratings yet
- 05 - DD Tools1Document27 pages05 - DD Tools1Slim.BNo ratings yet
- Principles of Spine Trauma and Spinal Deformities PDFDocument34 pagesPrinciples of Spine Trauma and Spinal Deformities PDFVirlan Vasile CatalinNo ratings yet
- Muscle Fiber Number in Biceps Brachii in Bodybuilders and Control SubjectsDocument5 pagesMuscle Fiber Number in Biceps Brachii in Bodybuilders and Control SubjectswaelNo ratings yet
- Hydraulic/Hydrostatic Schematic SJC With All Options: LegendDocument2 pagesHydraulic/Hydrostatic Schematic SJC With All Options: LegendEvert Vargas TorrezNo ratings yet
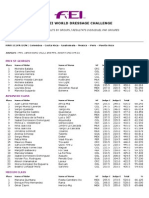
- 2013 WDC General Zone 2 ResultsDocument3 pages2013 WDC General Zone 2 ResultsPuertoRicoEcuestreNo ratings yet
- Jerry MaguireDocument12 pagesJerry Maguire123shashiNo ratings yet
- DX225LCA: Crawler ExcavatorDocument10 pagesDX225LCA: Crawler ExcavatorSajad PkNo ratings yet
- Modifying Your Pistol's Grip: Back To NotesDocument1 pageModifying Your Pistol's Grip: Back To NoteskurakNo ratings yet
- DCUO Weapons & StylesDocument3 pagesDCUO Weapons & StylesOminous DinNo ratings yet