Professional Documents
Culture Documents
Ankylosing Spondylitis Review Journal
Uploaded by
occha_fun08Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Ankylosing Spondylitis Review Journal
Uploaded by
occha_fun08Copyright:
Available Formats
Seminar
Ankylosing spondylitis
Jrgen Braun, Joachim Sieper
Ankylosing spondylitis is a common inammatory rheumatic disease that aects the axial skeleton, causing Lancet 2007; 369: 137990
characteristic inammatory back pain, which can lead to structural and functional impairments and a decrease in Ruhr-Universitt Bochum,
quality of life. New imaging techniques and therapies have substantially changed the management of this disease in Rheumazentrum Ruhrgebiet,
44652 Herne, Germany
the past decade. Whether inhibition of radiographic progression and structural damage can be reached with available
(Prof J Braun MD); Medical
drugs is as yet unclear. Furthermore, treatment with non-steroidal anti-inammatory agents and physiotherapy Department I, Rheumatology,
remains an important approach to long-term management of patients with ankylosing spondylitis. The new treatment Charit, Campus Benjamin
options with tumour necrosis factor blockers seems a breakthrough for patients refractory to conventional treatment. Franklin, Berlin, Germany
(Prof J Sieper MD)
Correspondence to:
Ankylosing spondylitis is the major subtype and a main Functional restrictions in patients with ankylosing
Prof Jrgen Braun
outcome of an inter-related group of rheumatic diseases spondylitis and a disease duration of 20 years are greater in j.braun@rheumazentrum-
now named spondyloarthritides. Clinical features of this those with a history of physically demanding jobs, more ruhrgebiet.de
group include inammatory back pain, asymmetrical comorbid conditions, and in smokers, than in those with
peripheral oligoarthritis (predominantly of the lower higher levels of education and a family history of this
limbs), enthesitis, and specic organ involvement such disease.8 Young age at onset of symptoms is associated
as anterior uveitis, psoriasis, and chronic inammatory with worse functional outcomes.9 In juvenile patients with
bowel disease. Aortic root involvement and conduction spondyloarthritides, clinical symptoms can be dierent
abnormalities are rare complications of ankylosing and include severe tarsitis.10 Male patients have more
spondylitis. Five subgroups are dierentiated clinically: structural changes, including bamboo spine, than do
ankylosing spondylitis, psoriatic spondyloarthritis, female patients.
reactive spondyloarthritis, spondyloarthritis associated
with inammatory bowel disease, and undierentiated Clinical features
spondyloarthritis. The subgroups are genetically Irrespective of the spondyloarthritis subtype, the main
linkedthe strongest known contributing factor is the clinical features of this group are inammatory back pain
MHC class I molecule HLA B27, although others still (panel 1) caused by sacroiliitis and inammation at other
remain to be identied. locations in the axial skeleton, peripheral arthritis,
enthesitis,11 and anterior uveitis,12 whereas manifestations
Epidemiology in other organs, such as the heart, are rare.13 Characteristic
Ankylosing spondylitis is a disease that aects young symptoms of ankylosing spondylitis are spinal stiness
people, who generally present at around 26 years of age. and loss of spinal mobility, which are explained by spinal
Men are more often aected than are women, with a ratio inammation, structural damage, or both.14 Spinal
of roughly 2 to 1.1 About 80% of patients develop the rst inammation can arise as spondylitis, spondylodiscitis,
symptoms at an age younger than 30 years, and less than or spondylarthritis. Structural changes are mainly caused
5% of patients present at older than 45 years.1 There is a by osteoproliferation rather than osteodestruction.
rough correlation between the prevalence of HLA B27 Syndesmophytes and ankylosis are the most characteristic
and the incidence and prevalence of this disease in a features of this disease, which are visible on conventional
specic population.2 HLA B27 is most prevalent in radiographs after some months to many years. Low bone
northern countries and some tribes (with up to 50% of density, osteoporosis,15 and an increased rate of fractures,16
cases), and is highest in Eskimo populations and Haida which may add to the hyperkyphosis predominantly seen
Indians. Overall, the prevalence of ankylosing spondylitis in male patients,17 add to the burden of disease.
is between 01% and 14%, with most of these data The peripheral arthritis is usually monoarticular or
coming from Europe. In mid-Europe a prevalence oligoarticular, and aects mainly but not exclusively the
of 0305% for ankylosing spondylitis3,4 and 12% for lower limbs.18 The hip and shoulder joints become aect-
the whole group of spondyloarthritides seems probable,
which is similar to that for rheumatoid arthritis.5 The
incidence of ankylosing spondylitis is between 05 and Search strategy and selection criteria
14 per 100 000 people per year in studies from dierent The Cochrane Library and Medline were searched from
countries.6,7 Several factors contribute to these dierences. 20002006. The search terms ankylosing spondylitis and
First is the selection of the target populations; second, the spondyloarthritis were used in combination with the terms
selection of screening criteria such as back pain and the epidemiology, pathogenesis, genetics, diagnosis,
choice of diagnostic criteria to conrm the diagnosis; and management, and therapy. Publications from the past
third, the prevalence of HLA B27 and the distribution of 6 years were preferentially selected but important ones from the
its subtypes, which diers in populations with ethnic past millennium were also included according to our judgment.
background.
www.thelancet.com Vol 369 April 21, 2007 1379
Seminar
The possible interaction between bacteria and HLA B27
Panel 1: Modied New York criteria 1984 for ankylosing spondylitis has a crucial role in models of the pathogenesis of
Clinical criteria spondyloarthritides. The fact that reactive arthritis is
Low back pain and stiness for longer than 3 months, which improve with exercise, triggered by genitourinary infections with Chlamydia
but are not relieved by rest trachomatis or by enteritis caused by gram-negative
Restriction of motion of the lumbar spine in both the sagittal and frontal planes enterobacteria, such as Shigella, Salmonella, Yersinia, and
Restriction of chest expansion relative to normal values correlated for age and sex Campylobacter spp28 provides a solid background for this
approach, but the evidence for triggering infections in
Radiological criterion other spondyloarthritides is marginal. The presence of
Sacroiliitis grade 2 bilaterally, or grade 34 unilaterally microbial antigens in the synovium of patients with
Denite ankylosing spondylitis is present if the radiological criterion is associated with at least one clinical criterion.70 reactive arthritis29 has suggested that persistence of
microbial antigens could be essential for continuing joint
inammation. About 1020% of HLA B27-positive patients
ed in about 20% of patients with this disease. Hip involve- with reactive arthritis develop the full clinical picture of
ment is regarded as a bad prognostic sign,19 but there is no ankylosing spondylitis after 1020 years.30 A possibly
agreement on the denition of severe disease. Inammation central role of bacteria in the pathogenesis of
of entheseal sites takes place not only at classic sites such spondyloarthritides is further supported by the relation
as the Achilles tendon and the plantar fascia but at many between Crohns disease, HLA B27 positivity, and
locations, including the spine. Eye inammation in ankylosing spondylitis: 54% of HLA B27-positive patients
spondyloarthritides is largely restricted to the uvea and with Crohns disease develop ankylosing spondylitis, but
takes place usually unilaterally, but can switch from one only 26% of HLA B27-negative patients develop this
side to the other.12 For reactive spondyloarthritis, the eye disease.31 Leakage of the gut mucosa, a result of
can be aected by conjunctivitis. inammation caused by colitis such as found in Crohns
Skin involvement (psoriasis) and colitis associated with disease, leads to an interaction of the immune system with
inammatory bowel disease can be regarded as basic gut bacteria. In about 50% of patients with ankylosing
subtype-dening entities with their own genetic spondylitis but no known Crohns disease, macroscopic or
background, dierent from HLA B27, rather than as microscopic mucosal chronic lesions resembling Crohns
disease manifestations. However, the spondyloarthritides disease have been detected in the gut mucosa.32
have also been regarded as one disease with a common Finally, some evidence of the importance of the
genetic background20 and two major phenotypes.21 B27-bacteria interaction comes from work in animals.
There are no good studies of prognosis in ankylosing HLA B27 transgenic rats develop spondyloarthritis-like
spondylitis. Two retrospective studies22,23 have suggested features, but many transgene copies are needed to transfer
that much radiographic progression happens early in the disease. Environmental factors also have a role since
rst 10 years of disease, and more recent studies have HLA B27 transgenic rats bred in a germ-free environment
shown that structural damage at presentation is the best do not develop disease,33 and gut ora contribute to the
predictor of further damage.24 Amor and colleagues19 colitis.34 However, persistence of microbial antigens in
proposed a list of prognostic items for the whole group of human spondyloarthritis in typically associated locations
spondyloarthritis including hip involvement and early seems unlikely, and no candidate bacteria were detected
onset, which has been conrmed.4 by PCR in biopsies from sacroiliac joints.35
Cartilagenous structurescollagen type II and
Pathogenesis proteoglycanhave been studied as probable targets of an
The cause of ankylosing spondylitis and other autoimmune response in ankylosing spondylitis.11,3639
spondyloarthritides is unknown. The two central features Although the collagen-II-induced arthritis model resembles
that deserve explanation are inammation and new bone rheumatoid arthritis, animals immunised with proteoglycan
formation, especially in the spine. Although inammation show features typical of ankylosing spondylitis.40 In patients
is assumed to trigger new bone formation, there is no with this disease, mononuclear cells invade cartilaginous
close correlation between inammation and osteo- structures of sacroiliac joints and intervertebral discs
proliferation. There is a strong genetic eect in leading to destruction and ankylosis.41 T-cell responses to
spondyloarthritides, especially in ankylosing spondylitis. aggrecan have been seen not only in spondyloarthritides
About a third of this eect is explained by HLA B27; the but also in other arthritides.42 Both CD4+43 and CD8+ T-cell
remainder, as yet largely undened, is associated with responses44 to aggrecan and collagen-derived peptides have
genes in and outside the MHC.25 9095% of patients with been reported in peripheral blood and synovial uid
ankylosing spondylitis are positive for HLA B27,26 and specimens of patients with ankylosing spondylitis.45
the risk of this disease developing is as high as about 5% Immunohistological studies on sacroiliac joint biopsies
in HLA B27-positive individuals, and substantially higher have shown cellular inltrates, including T cells and
in HLA B27-positive relatives of patients.27 However, most macrophages (gure 1).36,46 Immunohistological examin-
HLA B27-positive individuals remain healthy. ation of femoral heads of patients with this disease
1380 www.thelancet.com Vol 369 April 21, 2007
Seminar
undergoing total hip replacement47 showed inltrates of
A
CD4+ and CD8+ T cells at the cartilage-bone interface,
which are possibly dependent on the presence of cartilage.
Immunohistological examination of zygapophysal joints
from patients with this disease undergoing spinal surgery
because of severe kyphosis48 showed persistence of
inammation even in longstanding disease (gure 1).
Both innate and adaptive immune responses could have
a role in spondyloarthritides. The nding that tumour
necrosis factor (TNF)- is overexpressed in sacroiliac joints
(gure 1)46 provided a strong rationale for the use of TNF-
inhibitors, which are very eective in spondyloarthritides.
The remodelling of bone that explains squaring of
vertebral bodies in ankylosing spondylitis is histologically
based on acute and chronic spondylitis with destruction
and simultaneous rebuilding of the cortex and spongiosa
of the vertebral bodies. The development of square B
vertebral bodies is based on a combination of a destructive
osteitis and repair.49 The process of joint ankylosis partly
recapitulates embryonic endochondral bone formation in
a spontaneous model of arthritis in DBA-1 mice. Bone
growth factors such as bone morphogenetic protein
signalling are key molecular pathways associated with
pathological changes.50 Systemic gene transfer of noggin,
an antagonist of bone morphogenetic protein, is eective
both as a preventive and therapeutic strategy in this
mouse model, since noggin interferes with enthesial
progenitor cell proliferation. Immunohistochemical
staining for phosphorylated smad1/5 in entheseal biopsies
of patients with spondyloarthritides shows active bone
morphogenetic protein signalling in similar target cells,51
which suggests a role for these proteins in the pathogenesis
of ankylosing spondylitis. In psoriatic arthritis52 and anky-
C
losing spondylitis,47 an increased osteoclast activity has
been reported. Osteoclasts are key in inammation-
associated bone loss in rheumatic diseases.53
Patients with ankylosing spondylitis are frequently given
non-steroidal anti-inammatory drugs (NSAIDs), includ-
ing cyclo-oxygenase (COX)-2-selective inhibitors. COX-2 is
an inducible enzyme that converts arachidonic acid to
prostaglandin E2, a modulator of bone metabolism.54 The
inhibition of radiographic progression by continuous
intake of NSAIDs55 could be explained by the inhibition of
prostaglandins by these drugs. However, this nding
needs to be conrmed. Several in-vitro studies and work
in animals showed impaired bone healing in the presence
of NSAIDs.56 The steps associated with bone healing
include an inammatory response, bone resorption, and Figure 1: Immunohistology in ankylosing spondylitis
new bone formation. Prostaglandins have been shown to (A) T-cell inltrate in a biopsy specimen obtained from the sacroiliac joint of a
patient with ankylosing spondylitis. Reproduced from Bollow et al36 with
elicit and participate in inammatory responses, increase permission from BMJ Publishing Group. (B) Immunohistology of bone marrow
osteoclast activity and subsequent bone resorption, and close to a zygapophyseal joint of a patient with ankylosing spondylitis who
raise osteoblast activity and new bone formation. Through underwent spinal surgery for correction of rigid hyperkyphosis. The presence
inhibition of COX and subsequently prostaglandins, of CD3+ T cell aggregates indicates ongoing inammation in longstanding
disease. Reproduced from Appel et al48 with permission from Wiley-Liss, a
NSAIDs could inhibit new bone formation. This inhibition subsidiary of John Wiley & Sons. (C) TNFa mRNA (in-situ hybridisation) in a
is clinically used to prevent ossication after surgery, and biopsy specimen obtained from the sacroiliac joint of a patient with ankylosing
there may be dierences related to the degree of COX-1 spondylitis. Reproduced from Braun et al37 with permission from Wiley-Liss, a
and COX-2 inhibition.57 subsidiary of John Wiley & Sons.
www.thelancet.com Vol 369 April 21, 2007 1381
Seminar
A Genetics
Although HLA B27 itself is the most important gene
predisposing to ankylosing spondylitis, there is clear
evidence of association of other genes with susceptibility
to this disease. Studies (in twins)25 suggest a contribution
of HLA B27 of only about 2030% of the total genetic risk
in this disease, whereas the whole MHC contributes
about 4050%. The concordance rate is 63% for B27-
positive monozygotic twin pairs, and 23% for dizygotic
twin pairs. Furthermore, HLA B27-positive individuals
with a rst-degree relative having ankylosing spondylitis
have a six to 16 times greater risk of developing the disease
themselves than do B27-positive individuals with no
family history.25,58 All these data suggest that non-B27
B familial factors have a strong eect on the risk of
developing this disease.
Besides HLA B27, other MHC genes such as HLA B60
and HLA DR1 seem to be associated with ankylosing
spondylitis but they are of minor importance. The TNF
gene is another candidate gene located within the MHC,
but a major role of TNF polymorphisms in patients with
this disease is unlikely.59 Genome-wide linkage screens
have suggested several additional genetic markers
distributed on dierent chromosomes,60,61 none of which is
conclusive. There is some evidence for the presence of a
non-MHC susceptibility locus for spondyloarthritides
mapping to 9q31-34.62 No linkage of the X chromosome
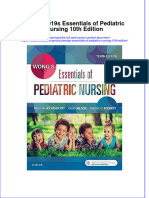
Figure 2: Pelvic radiograph and MRI of the sacroiliac joint in two
dierent patients with spondyloarthritis
(suspected to be a candidate gene because of the sex bias of
Radiograph showing chronic changes in the sacroiliac joints in a patient with ankylosing spondylitis), has been reported.63 Suggestive
ankylosing spondylitis (A) and MRI (STIR technique) showing active changes gene markers include genes associated with diseases that
(sacroiliitis) in a patient with undierentiated spondyloarthritis (B). predispose to spondyloarthritides such as psoriasis and
Possible combination of clinical, laboratory, or imaging SpA features Post-test probability
inammatory bowel disease, or markers that could
encompass genes relevant for immune responses, such as
IBP plus family history 51%
antigen processing and presentation or cytokine responses.
IBP plus heel pain 35%
For example, occurrence of acute anterior uveitis might be
IBP plus uveitis 54%
associated with a gene region located on chromosome 9.64
IBP plus synovitis 39%
The interleukin-1 gene cluster located on chromosome 2 is
IBP plus dactylitis 42%
involved in ankylosing spondylitis,65 but which exact genes
IBP plus family history plus heel pain 78%
are causatively involved is as yet unclear. NOD 2
IBP plus uveitis plus NSAID* 85%
(nucleotide-binding oligomerisation domain protein 2,
IBP plus heel pain plus synovitis plus alternating buttock pain 89%
CARD15) genotypes located on chromosome 16 are
IBP plus family history plus heel pain plus NSAID* 95%
IBP plus heel pain plus HLA-B27 83%
associated with Crohns disease but not with primary
IBP plus NSAIDs* plus HLA-B27 88%
ankylosing spondylitis.66 Other candidate gene analyses in
IBP plus heel pain without HLA-B27 6%
this disease, such as on TGF (transforming growth factor
IBP plus NSAIDs* without HLA-B27 8%
) and interleukin-6 polymorphisms, were negative. Thus,
IBP plus dactylitis plus ESR/CRP 62% there is a denite contribution of genes other than
IBP plus HLA-B27 plus ESR/CRP 78% HLA B27. Most genetic studies are on susceptibility but
IBP plus HLA-B27 without ESR/CRP 47% there are also some on severity that also suggest a strong
IBP plus HLA-B27 plus MRI 93% genetic rather than an environmental eect.67
IBP plus HLA-B27 without MRI 14%
IBP plus heel pain plus HLA-B27 without MRI 35% Diagnosis and classication
Radiography
The pretest probability of low back pain is assumed to be 5%. IBP-inammatory back pain. SpA=axial spondylarthritis.
CRP=C-reactive protein. *A good response to NSAIDs is needed. Adapted from Radwaleit et al76 with permission of
Sacroiliitis is a hallmark of ankylosing spondylitis, especially
BMJ Publishing Group. in earlier disease stages. It has become a major means for
the development of classication criteria because of its very
Table: Probability of axial spondylitis with or without various combinaions of features in patients with
high prevalence in patients with ankylosing spondylitis.
low back pain
The rst criteria set for classication, developed in 1961 in
1382 www.thelancet.com Vol 369 April 21, 2007
Seminar
Rome, Italy,68 did not need radiographs of the sacroiliac
joints to make a diagnosis, but in the 1966 New York (USA) Panel 2: New criteria for inammatory back pain in young to middle-aged adults
criteria radiographic evidence of sacroiliac joint changes (<50 years) with chronic back pain.
were included.69 The proposed grading system scored a Morning stiness >30 minutes
healthy radiograph of the sacroiliac joints as 0, suspicious Improvement in back pain with exercise but not with rest
changes as 1, minor changes as 2, moderate changes Awakening because of back pain during the second half of the night only
as 3 (gure 2), and ankylosis as 4. The last modication of Alternating buttock pain
the New York criteria70 introduced the clinical parameter of
The criteria are fullled if at least two of four of the parameters are present (sensitivity 703%, specicity 812%).
inammatory back pain, and changed the criterion
Adapted from Rudwaleit et al80 with permission from Wiley-Liss, a subsidiary of John Wiley & Sons.
restriction of chest expansion by age and sex adjustment of
the normal values (panel 1). These 1984 criteria are used not
only for classication, but also for diagnosis of patients likelihood of a diagnosis of spondyloarthritis is best if at
with ankylosing spondylitis. least three clinical, laboratory, or imaging indices are
Since radiographs of the sacroiliac joints could appear positive (table).72,76 The pretest probability could be
normal in the early phase of disease, structural changes dierent in other settings.
might become apparent only after some years, which is The clinical symptom of inammatory back pain is
relevant for a rather large proportion of patients with this important for the diagnosis of spondyloarthritis and
disease.71,72 With the introduction of MRI the fact that ankylosing spondylitis,79 including early and late stages,
radiography of the sacroiliac joints detects the structural and also classication.18,70,74 However, because of restricted
results of inammation (cartilage and bone damage) sensitivity and specicity of inammatory back pain, a
rather than inammation itself has become obvious. combination with other indices suggestive of spondylo-
Accordingly, the MRI technique allows for the detection arthritis is needed. A novel set of classication criteria for
of inammation in the sacroiliac joints in patients early inammatory back pain has been developed on the basis
in the course of their disease when no chronic changes of a controlled study showing a specicity of 81% and a
are detectable.37 This latency in the radiographic detection sensitivity of 70% if two of four indices are positive.80
of chronic changes in the sacroiliac joints contributes to However, the diagnostic yield is better than this result
the diagnostic delay in ankylosing spondylitis.1,73 when three of four indices are fullled (panel 2).
The development of criteria allowing for an early
Clinical criteria diagnosis of ankylosing spondylitis is important to alert
To allow for an earlier diagnosis of spondyloarthritides for primary care physicians to consider spondyloarthritis in
patients with predominant axial or peripheral mani- patients with chronic back pain. To establish when to refer
festations of disease, two sets of criteria were developed patients to a rheumatologist for diagnosis is of similar
about 15 years ago which are more clinically basedthe relevance. Screening indices for early referral of patients
European Spondyloarthropathy Study Group18 and the with ankylosing spondylitis by primary care physicians
Amor criteria.74 Radiographic evidence of sacroiliitis was have been proposed.81 A diagnosis of spondyloarthritis
included in both criteria sets as an optional item but not was predicted in every third to fth patient with chronic
as a prerequsite for diagnosis. Both sets work well as (>3 months) low back pain that started at an age younger
classication criteriavalidation studies in various popu- than 45 years who either has the clinical symptom of
lations showed a sensitivity and specicity of about 85%.75 inammatory back pain, carries HLA B27, or has
However, even though these criteria sets have also been sacroiliitis shown by imaging. How such criteria perform
used to make a diagnosis in clinical practice because of in daily clinical practice remains to be seen.
few alternatives, all sets for ankylosing spondylitis and
spondyloarthritis were developed for classication but not Laboratory tests
for diagnostic purposes. The process of classication There are two main laboratory indices that are potentially
implies a diagnostic selection beforehand, and, by contrast relevant for a diagnosis of spondyloarthritisHLA B27 and
with diagnostic criteria, knowledge of the pretest C-reactive protein.76 However, the role of the erythrocyte
probability of having the disease is not necessary.72 The sedimentation rate is less clear. HLA B27 is an important
use of classication criteria for diagnosis could result in factor for diagnosis of early spondyloarthritis. The
an overestimation or underestimation of the frequency of performance of the HLA-B27 test depends on the population
the disease. prevalence of HLA B27, which varies for dierent races.
A systematic approach to diagnose patients presenting There is no need to measure HLA-B27 subtypes in white
with early predominantly axial spondyloarthritis has been patients, but subtyping might be needed for Chinese
developed.72,76 The rst step is an estimation of the pretest patients, in whom some subtypes (eg, HLA-B*2706) are not
probability of the disease.77 In a cohort of patients with associated with ankylosing spondylitis. The correlation of
chronic low back pain in a primary care physician setting, disease activity with laboratory indices of inammation is
spondyloarthritis was diagnosed in 5% of cases, which is restricted. Only half of patients with this disease have raised
the assumed pretest probability of this disease.78 The C-reactive protein concentrations.82
www.thelancet.com Vol 369 April 21, 2007 1383
Seminar
Imaging
Imaging is crucial for the diagnosis and classication of NSAIDs
spondyloarthritides, especially ankylosing spondylitis,
Education,
because conventional radiography is suciently sensitive exercise, Peripheral A
Axial disease
in established disease since more than 95% of patients physical disease n
therapy, a
have structural changes in the sacroiliac joints (gure 2).83 rehabilitation, l S
Furthermore, the detection of typical syndesmophytes patient Sulfasalazine g u
associations,
(gure 3) could be useful for diagnosis in individual self help
e r
s g
patients. These possible osteoproliferative changes, groups Local corticosteroids
i e
however, do not tend to take place early in the course of c r
the disease. Therefore, MRI, with its capacity to visualise TNF blockers s y
active inammation, has been of much additional
diagnostic benet in early disease when a eld strength of Figure 4: Flow chart of the ASsessment of Ankylosing Spondylitis (ASAS) and
T2 for fat saturated and short T1 inversion recovery (STIR) European League Against Rheumatism (EULAR) recommendations for the
management of ankylosing spondylitis.
or a eld strength of T1 after application of contrast agents Adpated from Zochling et al98 with permission from BMJ Publishing Group.
such as gadolinium-diethylenetriamine penta-acetic acid NSAIDs=non-steroidal anti-inammatory drugs.
are used. For screening purposes, contrast agents are not
necessary since the STIR technique is sucient.84 peripheral joints and entheses,93 which are also well
MRI has proved especially useful for identication of assessed by ultrasonography.94
early sacroiliitis (gure 2)37 and spondylitis (gure 3),85 The cost-eectiveness of these imaging techniques in
including patients with undierentiated spondyloarthritis.86 early disease has not yet been assessed. Nevertheless, from
MRI of the sacroiliac joints can predict the development of a clinical point of view there seems little doubt that MRI
structural radiographic changes in these joints with a should be included in future classication and diagnostic
positive predictive value of 60% 3 years before they occur.87 criteria for early spondyloarthritides. In the assessment of
MRI measurements of the spine (gure 3)88 as assessed by patients with possible spondyloarthritides and low back
a new scoring system are sensitive to change in patients pain, dierentiation between the search for active and acute
with ankylosing spondylitis and inammatory back pain changes from chronic changes is important. For active and
on antiTNF therapy.89,90 The assessment of chronic changes acute changes, MRI with appropriate sequences such as
by MRI91 is still under investigation, but conventional STIR are useful, and in centres of excellence scintigraphy is
radiography is more sensitive to detect structural changes also of use, especially when the indication includes
than is MRI.92 Therefore, a radiograph of the sacroiliac screening for other aected sites. For the detection of
joints is always needed, especially at early disease stages chronic changes in the sacroiliac joints CT is most useful;95
because 2030% of patients within the rst 2 years of however, the technique should not be used routinely because
inammatory back pain will already have developed of a high exposure to radiation. Conventional radiography is
structural changes. MRI is not only useful for detection of still the gold standard for the detection of chronic structural
enthesitis and synovitis in the axial skeleton but also in changes in the sacroiliac joints and spine. The modied
Stoke ankylosing spondylitis spinal score is the most useful
A B scoring method for assessment of spinal damage in clinical
studies.96 In this system, syndesmophytes are most
important. Radiographic damage at baseline is the strongest
predictor of future structural changes.97
Management
Ten main recommendations for the management of
ankylosing spondylitis have been proposed by a combined
ASsessment in Ankylosing Spondylitis working group
(ASAS) and European League Against Rheumatism
(EULAR) task force (gure 4).98 Briey, the treatment of
ankylosing spondylitis should be tailored according to the
manifestations of the disease at presentation, severity of
symptoms, and several other features that include the
wishes and expectations of the patient. The disease
monitoring of patients should include history, clinical
features, laboratory tests, and imaging. The frequency of
Figure 3: Chronic and active changes in the lumbar spine of a patient with
monitoring should be decided on an individual basis
ankylosing spondylitis
Syndesmophytes shown on radiograph (A) and spondylitis and spondylodiscitis depending on symptoms, severity, and drugs. The best
shown by T2 weighted MRI (B). treatment needs a combination of non-pharmacological
1384 www.thelancet.com Vol 369 April 21, 2007
Seminar
and pharmacological treatment methods, including edu- pain.105,106 However, there are dierences between the trials
cation and physical therapy. AntiTNF therapy should be related to disease duration and the proportion of patients
given according to ASAS recommendations.99 Joint with peripheral arthritis. Thus, the eectiveness of
replacement has to be considered in patients with radio- sulfasalazine in earlier disease stages might dier from
graphic evidence of advanced hip involvement who have that at later stages. Indeed, in a controlled trial107 of
refractory pain and disability. Spinal surgery is useful in sulfasalazine in undierentiated spondyloarthritis and
selected patients with symptoms and disability because of early ankylosing spondylitis, some improvement of spinal
disabilitating posture or instable spine. pain was noted since patients with inammatory back
pain but no peripheral arthritis had substantially more
Basic principles of treatment improvement in disease activity than did the placebo
The standard treatment of spinal symptoms for patients group despite use of fewer NSAIDs.107 However, all patients
with ankylosing spondylitis has consisted of NSAIDs100and improved, and denite conclusions are dicult to draw.
structured exercise programmes101 for decades. Whether Methotrexate is generally used in patients with
and to what extent physical therapy and exercise are rheumatoid arthritis to improve symptoms and slow
benecial in every stage of the disease (eg, in very active progression of erosive disease. However, such improve-
disease) is unknown. Disease activity, especially the degree ment is not seen in ankylosing spondylitis, suggesting
of spinal inammation, function, and damage, probably
aects the outcome of physical therapy and regular exercise. Panel 3: Updated assessment in ankylosing spondylitis (ASAS) criteria for antiTNF
Non-pharmacological therapy consists of spa treatment,102 therapy in ankylosing spondylitis
education, and self-help groups, as well as physical therapy.
Diagnosis
A Cochrane review103 showed that there is little evidence for
Patients who usually full modied New York criteria (panel 1) for denitive AS
eectiveness of non-pharmacological intervention, but
there is strongly positive expert opinion. Although the Active disease
general eect size is believed to be rather small, it is clear Active disease for at least 4 weeks
from clinical experience that individual patients with BASDAI 4 (range 010) and an expert opinion*
ankylosing spondylitis may have denite benet from Treatment failure
intensive physiotherapy. Intensive spa therapy has proved All patients should have had adequate therapeutic trials of at least two NSAIDs. An
more eective than standard prescriptions of exercises in adequate therapeutic trial is dened as:
an outpatient setting, especially after several months.102 Treatment for at least 3 months at maximum recommended or tolerated anti-
inammatory dose unless contraindicated
NSAIDs Treatment for <3 months where treatment was withdrawn because of intolerance,
In general, NSAIDs work rather well in patients with toxicity, or contraindications
ankylosing spondylitis. A good response to NSAIDs has Patients with pure axial features do not have to take DMARDs before antiTNF therapy can
even been identied as a diagnostic sign for spondylo- be started
arthritides,74 although a state of non-responsiveness to Patients with symptomatic peripheral arthritis should have undergone at least one local
these drugs might identify those with a poor prognosis.19 corticosteroid injection if appropriate and should have responded insuciently
Clinical experience suggests that patients with active Patients with persistent peripheral arthritis must have had a therapeutic trial of sulfasalazine
disease should be continuously given NSAIDs in a dose Patients with symptomatic enthesitis must have failed appropriate local treatment
sucient to control pain and stiness. Some researchers55 All three of the above points have to be fullled before treatment with TNF blockers is started.
have even suggested that continuous dosing with NSAIDs
Contraindication
rather than the usual on-demand prescription decelerates
Women who are pregnant or breastfeeding; eective contraception must be practised
radiographic progression over 2 years. However, NSAIDs,
Active infection
including COX-2 inhibitors, are known to have
Patients at high risk of infection including:
gastrointestinal and possible cardiovascular toxic eects,104
Chronic leg ulcer
which could restrict their use. Furthermore, about half of
Previous tuberculosis
patients with this disease report insucient control of
Septic arthritis of a native joint within the past 12 months
their symptoms by NSAIDs alone.98 Sepsis of a prosthetic joint within the past 12 months, or indenitely if the joint remains
in situ
Disease-modifying antirheumatic drugs Persistent or recurrent chest infections
The use of disease-modifying antirheumatic drugs for the Indwelling urinary catheter
treatment of axial disease in spondyloarthritides has been History of lupus or multiple sclerosis
rather disappointing. Treatments that are eective in Malignant disease or premalignant states excluding:
suppression of disease activity and slowing of progression Basal cell carcinoma
in rheumatoid arthritis have notably failed to aect Malignant diseases diagnosed and treated more than 10 years previously (where the
patients with spondyloarthritides, especially those with probability of total cure is very high)
spinal disease.90,98 Sulfasalazine improves peripheral (Continues on next page)
arthritis associated with spondyloarthritis, but not spinal
www.thelancet.com Vol 369 April 21, 2007 1385
Seminar
arthritis. In ankylosing spondylitis, leunomide was not
(Continued from previous page) eective for axial manifestations,111,112 but patients with
Assessment of disease peripheral arthritis had some benet.111 However, this drug
ASsessment of Ankylosing Spondylitis (ASAS) core set for daily practice is eective in patients with psoriatic arthritis.113
Physical function (BASFI or Dougados functional index) Maksymowych and co-workers114 suggested that bis-
Pain (VAS, last week, pain at night and spine pain in general) phosphonates could be useful for spinal symptoms for
Spinal mobility (chest expansion and modied Schober and occiput to wall distance patients with ankylosing spondylitis. However, other
and lateral lumbar exion) studies with pamidronate failed to show a similar eect.115
Patients general assessment (VAS, last week) Thalidomide was also used with some success116 but is
Stiness (duration of morning stiness, spine, last week) regarded as too toxic for widespread use.
Peripheral joints and entheses (number of swollen joints [44 joints count], enthesitis
score such as developed in Maastricht, Berlin, or San Francisco) TNF blockers
Acute phase reactants (ESR or CRP) The introduction of TNF blockers has been the most
Fatigue (VAS) substantial development in the treatment of ankylosing
BASDAI spondylitis and other spondyloarthritides in the past few
VAS overall level of fatigue/tiredness past week years.98 Three such agents are now approved for ankylosing
VAS overall level of AS neck, back, or hip pain past week spondylitis: the monoclonal chimeric antibody iniximab,
VAS overall level of pain/swelling in joints other than neck, back, or hips past week which is given intravenously in a dose of 35 mg per kg
VAS overall discomfort from any areas tender to touch or pressure past week every 68 weeks (approved regimen is 5 mg/kg every
VAS overall level of morning stiness from time of awakening past week 68 weeks), the fully humanised monoclonal adalimumab
Duration and intensity (VAS) of morning stiness from time of awakening which is given subcutaneously in a dose of 40 mg every
(up to 120 mins) other week, and the 75 kD TNF receptor fusion protein
Assessment of response etanercept given subcutaneously in a dose of 50 mg once
Responder criteria per week or 25 mg twice per week. The success of antiTNF
BASDAI: 50% relative change or absolute improvement of 20 mm (0100) and expert treatment in spondyloarthritis is probably a class eect.
opinion: continuation yes/no There is some evidence that this treatment works even
Time of assessment better in spondyloarthritis than in rheumatoid arthritis.117
Between 6 and 12 weeks Large randomised, placebo-controlled trials118,119 of
iniximab, etanercept,120,121 and adalimumab122,123 in patients
VAS=visual analogue scale; all VAS can be replaced by a numerical rating scale (NRS). BASDAI=Bath ankylosing spondylitis disease with ankylosing spondylitis have shown impressive
activity index. BASFI=Bath ankylosing spondylitis functional index. AS=ankylosing spondylitis. *A physician, usually a rheumatolo-
gist, with expertise in inammatory back pain and the use of biological substances. Expert should be locally dened. An expert short-term improvements in spinal pain, function, and
opinion consists of both clinical features (history and examination) and either serum acute-phase reactant concentrations or imag- inammatory markers. As experience with these therapies
ing results, such as radiographs showing rapid progression or MRI scans indicating continuing inammation. Treatment for at
least 4 months at standard target dose or maximum tolerated dose unless contraindicated or not tolerated. Treatment for less than
increases to 25-year trials,124,125 eectiveness could persist
4 months, in which treatment was withdrawn because of intolerance or toxicity or contraindicated. Adapted from Braun et al99 with with continuing treatment, and more than a third of
permission from BMJ Publishing Group. patients are in remission. These trials show substantial
improvement of pain, function, and disease activity in
another pathomechanism. A systematic review108 of the patients with active disease compared with placebo.
use of methotrexate in ankylosing spondylitis showed Indeed, all outcome measures including Bath ankylosing
that there was no evidence for an eect on inammatory spondylitis disease activity index (BASDAI), functional
back pain and inconclusive evidence of eectiveness for index (BASFI), and metrology index (BASMI), and the
peripheral joint disease. The only randomised controlled physical component of the SF-36 health survey improved
trial109 of this drug in patients with ankylosing spondylitis greatly after 24 and 102 weeks. The improvement usually
failed to show a signicant eect of oral methotrexate starts within 2 weeks of therapy and C-reactive protein
(75 mg per week) on spondylitis, but there was some concentrations also tend to decrease rapidly.
improvement of peripheral arthritis. A 16-week open Alongside the reported long-term eectiveness and safety
label trial110 of methotrexate, 20 mg subcutaneously, in of TNF blockers in ankylosing spondylitis, the loss of
20 patients with ankylosing spondylitis did not show any response after cessation of continuous therapy with inixi-
eect on axial symptoms and only some improvement in mab for 3 years is important,126 but readministration has
peripheral symptoms. In contrast to these ndings, many been successful and has not caused problems. Treatment
rheumatologists are still using methotrexate for with iniximab decreases active spinal inammation as
ankylosing spondylitis because there used to be no other detected by MRI.89,90 No substantial radiological progression
options. The dierences in response between peripheral of disease as assessed by the modied Stoke ankylosing
and axial symptoms might be explained by predominant spondylitis spine score (SASSS), which scores radiographs
synovitis for peripheral manifestations and predominant in ankylosing spondylitis,127 was seen in a few patients with
enthesitis for axial manifestations. this disease who were given iniximab for 2 years.128
Similarly, leunomide is eective in treatment of The eectiveness of etanercept in this disease was also
symptoms and slowing radiographic change in rheumatoid seen,129 and the higher percentage of assessment of
1386 www.thelancet.com Vol 369 April 21, 2007
Seminar
ankylosing spondylitis responders in the active therapy joints is unclear. Two open studies142,143 of anakinra in
group was conrmed in randomised controlled trials,120,121 ankylosing spondylitis showed partly conicting results.
in which 2030% of patients continued treatment with Other biological compounds have not been tested so far.
disease-modifying antirheumatic drugs and corticosteroids.
After several months without etanercept therapy129,130 all Socioeconomics
patients had had a relapse of disease activity, but Cost-eectiveness is an issue when expensive treatments
reintroduction of the treatment was eective and safe. The are discussed. Despite the high costs, the clinical benets118
clinical eectiveness of etanercept was also conrmed by and improvements in quality of life in patients with
MRI.131 Adalimumab was also proved eective in patients ankylosing spondylitis given iniximab result in lower
with ankylosing spondylitis in a pilot study,122 and this disease-associated costs than does standard care, which
result was conrmed in a randomised controlled trial123 in translates to a short-term cost of about US$70 000
which the pain of some patients with even advanced spinal (GB35 000) per quality-adjusted life year (QALY)
ankylosis also improved. gained144an amount societies might be willing to pay.
The rst pilot studies129,132 of iniximab and etanercept However, the calculated costs were higher than this gure
in undierentiated spondyloarthritis have also been in other analyses.145 When modelling for long-term
successful. Similarly to iniximab, etanercept and therapy, with yearly disease progression of 007 of the
adalimumab are eective for peripheral joint and skin BASFI in the sensitivity analysis, the cost per QALY
symptoms in patients with psoriatic arthritis.133 Etanercept gained is reduced to less than $20 000 (10 000).144 Until
is eective for rheumatic manifestations in inammatory long-term data on disease progression with antiTNF
bowel disease for joint and spine but not gut symptoms.134 therapy in patients with ankylosing spondylitis are
Furthermore, etanercept has no eect on inammatory available, these conclusions remain hypothetical, but the
bowel disease,135 unlike iniximab, which is approved for costs for antiTNF therapy seem to fall well inside what is
Crohns disease136 and ulcerative colitis.137 Thus, etanercept thought of as cost eective. Furthermore, the daily
is not recommended for the small spondyloarthritis productivity of patients with active disease, which was
subgroup with concomitant inammatory bowel disease. substantially associated with functional impairment and
There could also be a dierence in the prevention and disease activity, greatly improved with iniximab, and this
treatment of anterior uveitis.138 was associated with reduced workday loss in employed
Clinical disease activity and spinal inammation as patients.146
detected by MRI are substantially reduced by TNF blockers, Conict of interest statement
as shown after short-term and long-term antiTNF J Braun and J Sieper have received consultancy and speakers fees,
therapy.122,131,139 Whether antiTNF treatment is able to stop honoraria, and research funding from several companies including
Abbott, Amgen, Centocor, MSD, Novartis, Pzer, Roche, Schering-Plough,
radiographic progression has not yet been proven. In a and Wyeth but they had no conict when writing this paper.
disease with pronounced long-term functional disability
References
due to the development of syndesmophytes and spinal 1 Feldtkeller E, Khan MA, van der Heijde D, van der Linden S, Braun J.
ankylosis,14 any treatment that does not only suppress Age at disease onset and diagnosis delay in HLA-B27 negative vs.
disease activity but also prevents or decelerates structural positive patients with ankylosing spondylitis. Rheumatol Int 2003;
23: 6166.
damage and decline of function will be of great importance 2 Khan MA. Epidemiology of HLA-B27 and arthritis. Clin Rheumatol
for patient care. Recommendations on which patients with 1996; 15 (suppl 1): 1012.
ankylosing spondylitis should be given TNF-blockers are 3 Braun J, Bollow M, Remlinger G, et al. Prevalence of
spondylarthropathies in HLA-B27 positive and negative blood donors.
especially needed because of possible side-eects and the Arthritis Rheum 1998; 41: 5867.
high costs of these drugs. Thus, patients with the best risk 4 Braun J, Listing J, Sieper J. Reply. Arthritis Rheum 2005; 52: 404950.
to benet ratio should be treated preferentially. An 5 Saraux A, Guedes C, Allain J, et al. Prevalence of rheumatoid arthritis
international assessment of ankylosing spondylitis and spondyloarthropathy in Brittany, France. Societe de Rhumatologie
de lOuest. J Rheumatol 1999; 26: 262227.
consensus statement for the use of antiTNF agents in 6 Akkoc N, Khan MA. Epidemiology of ankylosing spondylitis and
patients with this disease was reported in 2003140 and related spondyloarthropathies. In: Weisman MH, Reveille JD,
updated in 2006.99 Panel 3 shows a summary of these van der Heijde D, eds. Ankylosing spondylitis and the
spondyloarthropathies. London: Mosby, 2005: 117131.
recommendations for the initiation of antiTNF therapy.
7 Bakland G, Nossent HC, Gran JT. Incidence and prevalence of
Prediction of response is dicult. However, it seems clear ankylosing spondylitis in Northern Norway. Arthritis Rheum 2005; 53:
that patients early in the course of their disease, with raised 85055.
C-reactive protein concentrations,141 positive MRI ndings, 8 Ward MM, Weisman MH, Davis JC, Jr., Reveille JD. Risk factors for
functional limitations in patients with long-standing ankylosing
or less structural damage are more likely to respond than spondylitis. Arthritis Rheum 2005; 53: 71017.
are patients with advanced disease, but overall all patient 9 Stone M, Warren RW, Bruckel J, Cooper D, Cortinovis D, Inman RD.
subgroups could benet from this treatment. Juvenile-onset ankylosing spondylitis is associated with worse
functional outcomes than adult-onset ankylosing spondylitis.
Anakinra is a recombinant human interleukin-1 receptor Arthritis Rheum 2005; 53: 44551.
antagonist, which is directed at a dierent cytokine in the 10 Burgos-Vargas R, Vazquez-Mellado J. The early clinical recognition of
inammatory response than TNF blockers. By contrast juvenile-onset ankylosing spondylitis and its dierentiation from
juvenile rheumatoid arthritis. Arthritis Rheum 1995; 38: 83544.
with TNF, whether interleukin-1 is present in sacroiliac
www.thelancet.com Vol 369 April 21, 2007 1387
Seminar
11 McGonagle D, Gibbon W, Emery P. Classication of inammatory 36 Bollow M, Fischer T, Reisshauer H, et al. Quantitative analyses of
arthritis by enthesitis. Lancet 1998; 352: 113740. sacroiliac biopsies in spondyloarthropathies: T cells and macrophages
12 Martin TM, Smith JR, Rosenbaum JT. Anterior uveitis: current predominate in early and active sacroiliitis-cellularity correlates with
concepts of pathogenesis and interactions with the spondylo- the degree of enhancement detected by magnetic resonance imaging.
arthropathies. Curr Opin Rheumatol 2002; 14: 33741. Ann Rheum Dis 2000; 59: 13540.
13 Lautermann D, Braun J. Ankylosing spondylitiscardiac 37 Braun J, Bollow M, Neure L, et al. Use of immunohistologic and in
manifestations. Clin Exp Rheumatol 2002; 20 (suppl 28): S1115. situ hybridization techniques in the examination of sacroiliac joint
14 Wanders A, Landewe R, Dougados M, Mielants H, van der Linden S, biopsy specimens from patients with ankylosing spondylitis. Arthritis
van der Heijde D. Association between radiographic damage of the Rheum 1995; 38: 499505.
spine and spinal mobility for individual patients with ankylosing 38 Poole AR. The histopathology of ankylosing spondylitis: are there
spondylitis: can assessment of spinal mobility be a proxy for unifying hypotheses? Am J Med Sci 1998; 316: 22833.
radiographic evaluation? Ann Rheum Dis 2005; 64: 98894. 39 Maksymowych WP. Ankylosing spondylitisat the interface of bone
15 Karberg K, Zochling J, Sieper J, Felsenberg D, Braun J. Bone loss is and cartilage. J Rheumatol 2000; 27: 2295301.
detected more frequently in patients with ankylosing spondylitis with 40 Zhang Y. Animal models of inammatory spinal and sacroiliac joint
syndesmophytes. J Rheumatol 2005; 32: 129098. diseases. Rheum Dis Clin North Am 2003; 29: 63145.
16 Cooper C, Carbone L, Michet CJ, Atkinson EJ, OFallon WM, 41 Bardos T, Szabo Z, Czipri M, et al. A longitudinal study on an
Melton LJ 3rd. Fracture risk in patients with ankylosing spondylitis: a autoimmune murine model of ankylosing spondylitis. Ann Rheum Dis
population based study. J Rheumatol 1994; 21: 187782. 2005; 64: 98187.
17 Vosse D, van der Heijde D, Landewe R, et al. Determinants of 42 Guerassimov A, Zhang Y, Banerjee S, et al. Cellular immunity to the
hyperkyphosis in patients with ankylosing spondylitis. Ann Rheum Dis G1 domain of cartilage proteoglycan aggrecan is enhanced in patients
2006; 65: 77074. with rheumatoid arthritis but only after removal of keratan sulfate.
18 Dougados M, van der Linden S, Juhlin R, et al. The European Arthritis Rheum 1998; 41: 101925.
Spondylarthropathy Study Group preliminary criteria for the 43 Zou J, Zhang Y, Thiel A, et al. Predominant cellular immune response
classication of spondylarthropathy. Arthritis Rheum 1991; 34: 121827. to the cartilage autoantigenic G1 aggrecan in ankylosing spondylitis
19 Amor B, Santos RS, Nahal R, Listrat V, Dougados M. Predictive factors and rheumatoid arthritis. Rheumatology (Oxford) 2003; 42: 84655.
for the longterm outcome of spondyloarthropathies. J Rheumatol 1994; 44 Zou J, Appel H, Rudwaleit M, Thiel A, Sieper J. Analysis of the CD8+
21: 188387. T cell response to the G1 domain of aggrecan in ankylosing
20 Said-Nahal R, Miceli-Richard C, DAgostino MA, et al. Phenotypic spondylitis. Ann Rheum Dis 2005; 64: 72229.
diversity is not determined by independent genetic factors in familial 45 Atagunduz P, Appel H, Kuon W, et al. HLA-B27-restricted CD8+ T cell
spondylarthropathy. Arthritis Rheum 2001; 45: 47884. response to cartilage-derived self peptides in ankylosing spondylitis.
21 Porcher R, Said-Nahal R, DAgostino MA, Miceli-Richard C, Arthritis Rheum 2005; 52: 892901.
Dougados M, Breban M. Two major spondylarthropathy phenotypes 46 Braun J, Bollow M, Neure L, et al. Use of immunohistologic and in
are distinguished by pattern analysis in multiplex families. situ hybridization techniques in the examination of sacroiliac joint
Arthritis Rheum 2005; 53: 26371. biopsy specimens from patients with ankylosing spondylitis.
22 Carette S, Graham D, Little H, Rubenstein J, Rosen P. The natural Arthritis Rheum 1995; 38: 499505.
disease course of ankylosing spondylitis. Arthritis Rheum 1983; 26: 47 Appel H, Kuhne M, Spiekermann S, et al. Immunohistochemical
18690. analysis of hip arthritis in ankylosing spondylitis: evaluation of the
23 Gran JT, Skomsvoll JF. The outcome of ankylosing spondylitis: a study bone-cartilage interface and subchondral bone marrow.
of 100 patients. Br J Rheumatol 1997; 36: 76671. Arthritis Rheum 2006; 54: 180513.
24 van der Heijde D. Radiographic progression in ankylosing spondylitis. 48 Appel H, Kuhne M, Spiekermann S, et al. Immunohistological
Ann Rheum Dis 2004; 63 (suppl 1): 98. analysis of zygapophyseal joints in patients with ankylosing
25 Brown MA, Kennedy LG, MacGregor AJ, et al. Susceptibility to spondylitis. Arthritis Rheum 2006; 54: 284551.
ankylosing spondylitis in twins: the role of genes, HLA, and the 49 Aufdermaur M. Pathogenesis of square bodies in ankylosing
environment. Arthritis Rheum 1997; 40: 182328. spondylitis. Ann Rheum Dis 1989; 48: 62831.
26 Brewerton DA, Hart FD, Nicholls A, Carey M, James DC, 50 Reddi AH. Cartilage morphogenetic proteins: role in joint
Sturrock RD. Ankylosing spondylitis and HL-A 27. Lancet 1973; 301: development, homoeostasis, and regeneration. Ann Rheum Dis 2003;
90407. 62 (suppl 2): 7378.
27 van der Linden SM, Valkenburg HA, de Jongh BM, Cats A. The risk of 51 Lories RJ, Derese I, Luyten FP. Modulation of bone morphogenetic
developing ankylosing spondylitis in HLA-B27 positive individuals. A protein signaling inhibits the onset and progression of ankylosing
comparison of relatives of spondylitis patients with the general enthesitis. J Clin Invest 2005; 115: 157179.
population. Arthritis Rheum 1984; 27: 24119. 52 Ritchlin CT, Haas-Smith SA, Li P, Hicks DG, Schwarz EM.
28 Sieper J, Braun J, Kingsley GH. Report on the fourth international Mechanisms of TNF-alpha- and RANKL-mediated osteoclastogenesis
workshop on reactive arthritis. Arthritis Rheum 2000; 43: 72034. and bone resorption in psoriatic arthritis. J Clin Invest 2003; 111: 82131.
29 Granfors K, Jalkanen S, von Essen R, et al. Yersinia antigens in 53 Walsh NC, Crotti TN, Goldring SR, Gravallese EM. Rheumatic diseases:
synovial-uid cells from patients with reactive arthritis. N Engl J Med the eects of inammation on bone. Immunol Rev 2005; 208: 22851.
1989; 320: 21621. 54 Radi ZA, Khan NK. Eects of cyclooxygenase inhibition on bone,
30 Leirisalo-Repo M, Helenius P, Hannu T, et al. Long-term prognosis of tendon, and ligament healing. Inamm Res 2005; 54: 35866.
reactive salmonella arthritis. Ann Rheum Dis 1997; 56: 51620. 55 Wanders A, Heijde D, Landewe R, et al. Nonsteroidal
31 Purrmann J, Zeidler H, Bertrams J, et al. HLA antigens in ankylosing antiinammatory drugs reduce radiographic progression in patients
spondylitis associated with Crohns disease. Increased frequency of the with ankylosing spondylitis: a randomized clinical trial.
HLA phenotype B27,B44. J Rheumatol 1988; 15: 165861. Arthritis Rheum 2005; 52: 175665.
32 De Vos M, Cuvelier C, Mielants H, Veys E, Barbier F, Elewaut A. 56 Einhorn TA. Cox-2: where are we in 2003? - The role of
Ileocolonoscopy in seronegative spondylarthropathy. Gastroenterology cyclooxygenase-2 in bone repair. Arthritis Res Ther 2003; 5: 57.
1989; 96: 33944. 57 Barthel T, Baumann B, Noth U, Eulert J. Prophylaxis of heterotopic
33 Taurog JD, Richardson JA, Croft JT, et al. The germfree state prevents ossication after total hip arthroplasty: a prospective randomized study
development of gut and joint inammatory disease in HLA-B27 comparing indomethacin and meloxicam. Acta Orthop Scand 2002; 73:
transgenic rats. J Exp Med 1994; 180: 235964. 61114.
34 Onderdonk AB, Richardson JA, Hammer RE, Taurog JD. Correlation 58 van der Linden S, Valkenburg H, Cats A. The risk of developing
of cecal microora of HLA-B27 transgenic rats with inammatory ankylosing spondylitis in HLA-B27 positive individuals: a family and
bowel disease. Infect Immun 1998; 66: 602223. population study. Br J Rheumatol 1983; 22 (suppl 2): 1819.
35 Braun J, Tuszewski M, Ehlers S, et al. Nested polymerase chain 59 Rudwaleit M, Hohler T. Cytokine gene polymorphisms relevant for the
reaction strategy simultaneously targeting DNA sequences of multiple spondyloarthropathies. Curr Opin Rheumatol 2001; 13: 25054.
bacterial species in inammatory joint diseases. II. Examination of 60 Laval SH, Timms A, Edwards S, et al. Whole-genome screening in
sacroiliac and knee joint biopsies of patients with spondylo- ankylosing spondylitis: evidence of non-MHC genetic-susceptibility
arthropathies and other arthritides. J Rheumatol 1997; 24: 110105. loci. Am J Hum Genet 2001; 68: 91826.
1388 www.thelancet.com Vol 369 April 21, 2007
Seminar
61 Zhang G, Luo J, Bruckel J, et al. Genetic studies in familial ankylosing 86 Brandt J, Bollow M, Haberle J, et al. Studying patients with
spondylitis susceptibility. Arthritis Rheum 2004; 50: 224654. inammatory back pain and arthritis of the lower limbs clinically and
62 Miceli-Richard C, Zouali H, Said-Nahal R, et al. Signicant linkage by magnetic resonance imaging: many, but not all patients with
to spondyloarthropathy on 9q31-34. Hum Mol Genet 2004; 13: sacroiliitis have spondyloarthropathy. Rheumatology (Oxford) 1999; 38:
164148. 83136.
63 Hoyle E, Laval SH, Calin A, Wordsworth BP, Brown MA. The 87 Oostveen J, Prevo R, den Boer J, van de Laar M. Early detection of
X-chromosome and susceptibility to ankylosing spondylitis. sacroiliitis on magnetic resonance imaging and subsequent
Arthritis Rheum 2000; 43: 135355. development of sacroiliitis on plain radiography. A prospective,
longitudinal study. J Rheumatol 1999; 26: 195358.
64 Martin TM, Zhang G, Luo J, et al. A locus on chromosome 9p
predisposes to a specic disease manifestation, acute anterior uveitis, 88 Baraliakos X, Hermann KG, Landewe R, et al. Assessment of acute
in ankylosing spondylitis, a genetically complex, multisystem, spinal inammation in patients with ankylosing spondylitis by
inammatory disease. Arthritis Rheum 2005; 52: 26974. magnetic resonance imaging: a comparison between contrast
enhanced T1 and short tau inversion recovery (STIR) sequences.
65 Maksymowych WP, Reeve JP, Reveille JD, et al. High-throughput
Ann Rheum Dis 2005; 64: 114144.
single-nucleotide polymorphism analysis of the IL1RN locus in
patients with ankylosing spondylitis by matrix-assisted laser 89 Braun J, Baraliakos X, Golder W, et al. Magnetic resonance imaging
desorption ionization-time-of-ight mass spectrometry. examinations of the spine in patients with ankylosing spondylitis,
Arthritis Rheum 2003; 48: 201118. before and after successful therapy with iniximab: evaluation of a
new scoring system. Arthritis Rheum 2003; 48: 112636.
66 Crane AM, Bradbury L, van Heel DA, et al. Role of NOD2 variants in
spondylarthritis. Arthritis Rheum 2002; 46: 162933. 90 Braun J, Landewe R, Hermann KG, et al. Major reduction in spinal
inammation in patients with ankylosing spondylitis after treatment
67 Hamersma J, Cardon LR, Bradbury L, et al. Is disease severity in with iniximab: results of a multicenter, randomized, double-blind,
ankylosing spondylitis genetically determined? Arthritis Rheum 2001; placebo-controlled magnetic resonance imaging study. Arthritis Rheum
44: 1396400. 2006; 54: 164652.
68 Kellgren JH. Diagnostic criteria for population studies. 91 Braun J, Baraliakos X, Golder W, et al. Analysing chronic spinal
Bull Rheum Dis 1962; 13: 29192. changes in ankylosing spondylitis: a systematic comparison of
69 Bennett PH, Burch TA. Population studies of the rheumatic diseases. conventional x rays with magnetic resonance imaging using
Amsterdam: Excerpta Medica Foundation, 1968: 45657. established and new scoring systems. Ann Rheum Dis 2004; 63:
70 van der Linden S, Valkenburg HA, Cats A. Evaluation of diagnostic 104655.
criteria for ankylosing spondylitis. A proposal for modication of the 92 Heuft-Dorenbosch L, Landewe R, Weijers R, et al. Combining
New York criteria. Arthritis Rheum 1984; 27: 36168. information obtained from magnetic resonance imaging and
71 Mau W, Zeidler H, Mau R, et al. Clinical features and prognosis of conventional radiographs to detect sacroiliitis in patients with recent
patients with possible ankylosing spondylitis. Results of a 10-year onset inammatory back pain. Ann Rheum Dis 2006; 65: 80408.
followup. J Rheumatol 1988; 15: 110914. 93 McGonagle D, Gibbon W, OConnor P, Green M, Pease C, Emery P.
72 Rudwaleit M, Khan MA, Sieper J. The challenge of diagnosis and Characteristic magnetic resonance imaging entheseal changes of knee
classication in early ankylosing spondylitis: do we need new synovitis in spondylarthropathy. Arthritis Rheum 1998; 41: 694700.
criteria? Arthritis Rheum 2005; 52: 100008. 94 Balint PV, Kane D, Wilson H, McInnes IB, Sturrock RD.
73 van der Linden S, van der Heijde D. Ankylosing spondylitis. Clinical Ultrasonography of entheseal insertions in the lower limb in
features. Rheum Dis Clin North Am 1998; 24: 66376. spondyloarthropathy. Ann Rheum Dis 2002; 61: 90510.
74 Amor B, Dougados M, Listrat V, et al. Are classication criteria for 95 van Tubergen A, Heuft-Dorenbosch L, Schulpen G, et al. Radiographic
spondylarthropathy useful as diagnostic criteria? Rev Rhum Engl Ed assessment of sacroiliitis by radiologists and rheumatologists: does
1995; 62: 1015. training improve quality? Ann Rheum Dis 2003; 62: 51925.
75 Collantes-Estevez E, Cisnal del Mazo A, Munoz-Gomariz E. 96 Wanders AJ, Landewe RB, Spoorenberg A, et al. What is the most
Assessment of 2 systems of spondyloarthropathy diagnostic and appropriate radiologic scoring method for ankylosing spondylitis? A
classication criteria (Amor and ESSG) by a Spanish multicenter comparison of the available methods based on the Outcome Measures
study. European Spondyloarthropathy Study Group. J Rheumatol in Rheumatology Clinical Trials lter. Arthritis Rheum 2004; 50:
1995; 22: 24651. 262232.
76 Rudwaleit M, van der Heijde D, Khan MA, Braun J, Sieper J. How to 97 Baraliakos X, Listing J, Rudwaleit M, et al. Progression of radiographic
diagnose axial spondyloarthritis early. Ann Rheum Dis 2004; 63: damage in patients with ankylosing spondylitisDening the central
53543. role of syndesmophytes. Ann Rheum Dis 2007; published online
Feb 28. DOI:10.1136/ard.2006.066415.
77 Grimes DA, Schulz KF. Rening clinical diagnosis with likelihood
ratios. Lancet 2005; 365: 150005. 98 Zochling J, van der Heijde D, Burgos-Vargas R, et al. ASAS/EULAR
recommendations for the management of ankylosing spondylitis.
78 Underwood MR, Dawes P. Inammatory back pain in primary care.
Ann Rheum Dis 2006; 65: 44252.
Br J Rheumatol 1995; 34: 107477.
99 Braun J, Davis J, Dougados M, Sieper J, van der Linden S,
79 Calin A, Porta J, Fries JF, Schurman DJ. Clinical history as a
van der Heijde D. First update of the international ASAS consensus
screening test for ankylosing spondylitis. JAMA 1977; 237: 261314. statement for the use of anti-TNF agents in patients with ankylosing
80 Rudwaleit M, Metter A, Listing J, Sieper J, Braun J. Inammatory spondylitis. Ann Rheum Dis 2006; 65: 31620.
back pain in ankylosing spondylitis: a reassessment of the clinical 100 Dougados M, Dijkmans B, Khan M, Maksymowych W,
history for application as classication and diagnostic criteria. van der Linden S, Brandt J. Conventional treatments for ankylosing
Arthritis Rheum 2006; 54: 56978. spondylitis. Ann Rheum Dis 2002; 61 (suppl 3): 4050.
81 Sieper J, Rudwaleit M. Early referral recommendations for 101 Kraag G, Stokes B, Groh J, Helewa A, Goldsmith C. The eects of
ankylosing spondylitis (including pre-radiographic and radiographic comprehensive home physiotherapy and supervision on patients with
forms) in primary care. Ann Rheum Dis 2005; 64: 65963. ankylosing spondylitisa randomized controlled trial. J Rheumatol
82 Spoorenberg A, van der Heijde D, de Klerk E, et al. Relative value 1990; 17: 22833.
of erythrocyte sedimentation rate and C-reactive protein in 102 van Tubergen A, Landewe R, van der Heijde D, et al. Combined
assessment of disease activity in ankylosing spondylitis. J Rheumatol spa-exercise therapy is eective in patients with ankylosing spondylitis:
1999; 26: 98084. a randomized controlled trial. Arthritis Rheum 2001; 45: 43038.
83 Krebs W. Das Rntgenbild des Beckens bei der Bechterewschen 103 Dagnrud H, Kvien TK, Hagen KB. The Cochrane review of
Krankheit. Fortschr Rntgenstrahlen 1934; 50: 537. physiotherapy interventions for ankylosing spondylitis. J Rheumatol
84 Hermann KG, Landewe RB, Braun J, van der Heijde DM. Magnetic 2005; 32: 1899906.
resonance imaging of inammatory lesions in the spine in 104 Ward MM, Kuzis S. Medication toxicity among patients with
ankylosing spondylitis clinical trials: is paramagnetic contrast ankylosing spondylitis. Arthritis Rheum 2002; 47: 23441.
medium necessary? J Rheumatol 2005; 32: 205660. 105 Dougados M, vam der Linden S, Leirisalo-Repo M, et al.
85 Braun J, Bollow M, Sieper J. Radiologic diagnosis and pathology of Sulfasalazine in the treatment of spondylarthropathy. A randomized,
the spondyloarthropathies. Rheum Dis Clin North Am 1998; 24: multicenter, double-blind, placebo-controlled study. Arthritis Rheum
697735. 1995; 38: 61827.
www.thelancet.com Vol 369 April 21, 2007 1389
Seminar
106 Chen J, Liu C. Sulfasalazine for ankylosing spondylitis. 127 Creemers MC, Franssen MJ, vant Hof MA, Gribnau FW,
Cochrane Database Syst Rev 2005; 2: CD004800. van de Putte LB, van Riel PL. Assessment of outcome in ankylosing
107 Braun J, Zochling J, Baraliakos X, Alten RH, Burmester GR, spondylitis: an extended radiographic scoring system. Ann Rheum Dis
Grasedyck K, et al. Ecacy of sulfasalazine in patients with 2005; 64: 12729.
inammatory back pain due to undierentiated spondyloarthritis and 128 Baraliakos X, Listing J, Rudwaleit M, Brandt J, Sieper J, Braun J.
early ankylosing spondylitis: a multicentre randomized controlled trial. Radiographic progression in patients with ankylosing spondylitis after
Ann Rheum Dis 2006. 2 years of treatment with the tumour necrosis factor alpha antibody
108 Chen J, Liu C. Methotrexate for ankylosing spondylitis. iniximab. Ann Rheum Dis 2005; 64: 146266.
Cochrane Database Syst Rev 2004; 3: CD004524. 129 Brandt J, Khariouzov A, Listing J, et al. Successful short term
109 Gonzalez-Lopez L, Garcia-Gonzalez A, Vazquez-Del-Mercado M, treatment of patients with severe undierentiated spondyloarthritis
Munoz-Valle JF, Gamez-Nava JI. Ecacy of methotrexate in with the anti-tumor necrosis factor-alpha fusion receptor protein
ankylosing spondylitis: a randomized, double blind, placebo controlled etanercept. J Rheumatol 2004; 31: 53138.
trial. J Rheumatol 2004; 31: 156874. 130 Brandt J, Listing J, Haibel H, et al. Long-term ecacy and safety of
110 Haibel H, Brandt HC, Song IH, et al. No ecacy of subcutaneous etanercept after readministration in patients with active ankylosing
methotrexate in active ankylosing spondylitis: a 16-week open-label spondylitis. Rheumatology (Oxford) 2005; 44: 34248.
trial. Ann Rheum Dis. 2007; 66: 41921. 131 Baraliakos X, Davis J, Tsuji W, Braun J. Magnetic resonance imaging
111 Haibel H, Rudwaleit M, Braun J, Sieper J. Six months open label trial examinations of the spine in patients with ankylosing spondylitis
of leunomide in active ankylosing spondylitis. Ann Rheum Dis 2005; before and after therapy with the tumor necrosis factor alpha receptor
64: 12426. fusion protein etanercept. Arthritis Rheum 2005; 52: 121623.
112 Van Denderen JC, Van der Paardt M, Nurmohamed MT, De Ryck YM, 132 Brandt J, Haibel H, Reddig J, Sieper J, Braun J. Successful short term
Dijkmans BA, Van der Horst-Bruinsma IE. Double-blind, randomised, treatment of severe undierentiated spondyloarthropathy with the
placebo-controlled study of leunomide in the treatment of active anti-tumor necrosis factor-alpha monoclonal antibody iniximab.
ankylosing spondylitis. Ann Rheum Dis 2005; 64: 176164. J Rheumatol 2002; 29: 11822.
113 Kaltwasser JP, Nash P, Gladman D, et al. Ecacy and safety of 133 Mease PJ, Kivitz AJ, Burch FX, et al. Etanercept treatment of psoriatic
leunomide in the treatment of psoriatic arthritis and psoriasis: a arthritis: safety, ecacy, and eect on disease progression.
multinational, double-blind, randomized, placebo-controlled clinical
Arthritis Rheum 2004; 50: 226472.
trial. Arthritis Rheum 2004; 50: 193950.
134 Marzo-Ortega H, McGonagle D, OConnor P, Emery P. Ecacy of
114 Maksymowych WP, Jhangri GS, Fitzgerald AA, et al. A six-month
etanercept for treatment of Crohns related spondyloarthritis but not
randomized, controlled, double-blind, dose-response comparison of
colitis. Ann Rheum Dis 2003; 62: 7476.
intravenous pamidronate (60 mg versus 10 mg) in the treatment of
nonsteroidal antiinammatory drug-refractory ankylosing spondylitis. 135 Sandborn WJ, Hanauer SB, Katz S, et al. Etanercept for active Crohns
Arthritis Rheum 2002; 46: 76673. disease: a randomized, double-blind, placebo-controlled trial.
115 Haibel H, Brandt J, Rudwaleit M, Soerensen H, Sieper J, Braun J. Gastroenterology 2001; 121: 108894.
Treatment of active ankylosing spondylitis with pamidronate. 136 Hanauer SB, Feagan BG, Lichtenstein GR, et al. Maintenance
Rheumatology (Oxford) 2003; 42: 101820. iniximab for Crohns disease: the ACCENT I randomised trial. Lancet
116 Huang F, Gu J, Zhao W, Zhu J, Zhang J, Yu DT. One-year open-label 2002; 359: 154149.
trial of thalidomide in ankylosing spondylitis. Arthritis Rheum 2002; 137 Rutgeerts P, Sandborn WJ, Feagan BG, et al. Iniximab for induction
47: 24954. and maintenance therapy for ulcerative colitis. N Engl J Med 2005; 353:
117 Heiberg MS, Nordvag BY, Mikkelsen K, et al. The comparative 246276.
eectiveness of tumor necrosis factor-blocking agents in patients with 138 Braun J, Baraliakos X, Listing J, Sieper J. Decreased incidence of
rheumatoid arthritis and patients with ankylosing spondylitis: a anterior uveitis in patients with ankylosing spondylitis treated with the
six-month, longitudinal, observational, multicenter study. anti-tumor necrosis factor agents iniximab and etanercept.
Arthritis Rheum 2005; 52: 250612. Arthritis Rheum 2005; 52: 244751.
118 Braun J, Brandt J, Listing J, et al. Treatment of active ankylosing 139 Sieper J, Baraliakos X, Listing J, et al. Persistent reduction of spinal
spondylitis with iniximab: a randomised controlled multicentre trial. inammation as assessed by magnetic resonance imaging in patients
Lancet 2002; 359: 118793. with ankylosing spondylitis after 2 yrs of treatment with the
119 van der Heijde D, Dijkmans B, Geusens P, et al. Ecacy and safety of anti-tumour necrosis factor agent iniximab. Rheumatology (Oxford)
iniximab in patients with ankylosing spondylitis: results of a 2005; 44: 152530.
randomized, placebo-controlled trial (ASSERT). Arthritis Rheum 2005; 140 Braun J, Pham T, Sieper J, et al. International ASAS consensus
52: 58291. statement for the use of anti-tumour necrosis factor agents in patients
120 Davis JC, Jr., Van Der Heijde D, Braun J, et al. Recombinant human with ankylosing spondylitis. Ann Rheum Dis 2003; 62: 81724.
tumor necrosis factor receptor (etanercept) for treating ankylosing 141 Rudwaleit M, Listing J, Brandt J, Braun J, Sieper J. Prediction of a
spondylitis: a randomized, controlled trial. Arthritis Rheum 2003; 48: major clinical response (BASDAI 50) to tumour necrosis factor alpha
323036. blockers in ankylosing spondylitis. Ann Rheum Dis 2004; 63: 66570.
121 Calin A, Dijkmans BA, Emery P, et al. Outcomes of a multicentre 142 Tan AL, Marzo-Ortega H, OConnor P, Fraser A, Emery P,
randomised clinical trial of etanercept to treat ankylosing spondylitis. McGonagle D. Ecacy of anakinra in active ankylosing spondylitis: a
Ann Rheum Dis 2004; 63: 1594600. clinical and magnetic resonance imaging study. Ann Rheum Dis 2004;
122 Haibel H, Rudwaleit M, Brandt HC, et al. Adalimumab reduces spinal 63: 104145.
symptoms in active ankylosing spondylitis - clinical and magnetic
143 Haibel H, Rudwaleit M, Listing J, Sieper J. Open label trial of anakinra
resonance imaging results of a fty-two week open label trial.
in active ankylosing spondylitis over 24 weeks. Ann Rheum Dis 2005;
Arthritis Rheum 2006; 54: 67881.
64: 29698.
123 van der Heijde D, Kivitz A, Schi M, et al. Adalimumab therapy
144 Kobelt G, Andlin-Sobocki P, Brophy S, Jonsson L, Calin A, Braun J.
results in signicant reduction of signs and symptoms in subjects
with ankylosing spondylitis: the ATLAS trial. Arthritis Rheum 2006; 54: The burden of ankylosing spondylitis and the cost-eectiveness of
213646. treatment with iniximab (Remicade). Rheumatology (Oxford) 2004;
43: 115866.
124 Baraliakos X, Brandt J, Listing J, et al. Outcome of patients with active
anklyosing spondylitis after 2 years of therapy with etanercept 145 Boonen A, van der Heijde D, Severens JL, et al. Markov model into the
clinical and magnetic resonance imaging data. Arthritis Res Ther cost-utility over ve years of etanercept and iniximab compared with
2005; 53: 85663. usual care in patients with active ankylosing spondylitis.
Ann Rheum Dis 2006; 65: 20108.
125 Braun J, Baraliakos X, Brandt J, et al. Persistent clinical response
to the anti-TNF-alpha antibody iniximab in patients with 146 van der Heijde D, Han C, Devlam K, et al. Iniximab improves
ankylosing spondylitis over 3 years. Rheumatology (Oxford) 2005; productivity and reduces workday loss in patients with ankylosing
44: 67076. spondylitis: results from a randomized, placebo-controlled trial.
126 Baraliakos X, Listing J, Brandt J, Rudwaleit M, Sieper J, Braun J. Arthritis Rheum 2006; 55: 56974.
Clinical response to discontinuation of anti-TNF therapy in patients
with ankylosing spondylitis after 3 years of continuous treatment with
iniximab. Arthritis Res Ther 2005; 7: R43944.
1390 www.thelancet.com Vol 369 April 21, 2007
You might also like
- Schizophrenia and Other Psychotic DisordersDocument68 pagesSchizophrenia and Other Psychotic DisordersRushdaNo ratings yet
- Medical History and Evaluation FormDocument22 pagesMedical History and Evaluation FormJobelle Fernandez-SantosNo ratings yet
- ABNORMAL PSYCHOLOGY DRILLS PART IIDocument200 pagesABNORMAL PSYCHOLOGY DRILLS PART IIMARIE ROSE L. FUNTANARNo ratings yet
- Home Study Course-HomeopathDocument155 pagesHome Study Course-HomeopathAzad Ansari67% (6)
- Wongs Essentials of Pediatric Nursing 10th EditionDocument61 pagesWongs Essentials of Pediatric Nursing 10th Editionnorma.fegley884100% (30)
- Clinical Manual of Psychosomatic Medicine A Guide To ConsultatiDocument565 pagesClinical Manual of Psychosomatic Medicine A Guide To ConsultatiDalal HazelNo ratings yet
- Physical Therapy Management of Congenital Muscular.2Document47 pagesPhysical Therapy Management of Congenital Muscular.2Katherine Valeska Sánchez MuñozNo ratings yet
- Axial Psoriatic Arthritis An UpdateDocument10 pagesAxial Psoriatic Arthritis An Updateproject zoroNo ratings yet
- Case Presentation DFDocument13 pagesCase Presentation DFCharanNo ratings yet
- Separation Anxiety in ChildrenDocument5 pagesSeparation Anxiety in Childrenfayswan4232100% (1)
- Seminar: Joachim Sieper, Denis PoddubnyyDocument12 pagesSeminar: Joachim Sieper, Denis PoddubnyyDaniel FernandezNo ratings yet
- IndianJClinAnaesth 9 3 374 378Document5 pagesIndianJClinAnaesth 9 3 374 378bhaskaracharya dontabhaktuniNo ratings yet
- Spondylodiscitis Severity Code: Scoring System For The Classification and Treatment of Non-Specific SpondylodiscitisDocument9 pagesSpondylodiscitis Severity Code: Scoring System For The Classification and Treatment of Non-Specific SpondylodiscitisEduardo RodriguezNo ratings yet
- Ankylosing Spondylitis BMJ RevDocument5 pagesAnkylosing Spondylitis BMJ RevsamarqandiNo ratings yet
- PSB 419Document7 pagesPSB 419Erick PrasetyaNo ratings yet
- Case Report: Tuberculous Spondylitis: A Report of Different Clinical Scenarios and Literature UpdateDocument5 pagesCase Report: Tuberculous Spondylitis: A Report of Different Clinical Scenarios and Literature UpdatepuaanNo ratings yet
- Tuberculous Spondylitis PDFDocument5 pagesTuberculous Spondylitis PDFpuaanNo ratings yet
- Os 15 1454Document14 pagesOs 15 1454tugas rendyNo ratings yet
- Pyogenic Spinal InfectionsDocument16 pagesPyogenic Spinal InfectionsFrancisco Escobar MoralesNo ratings yet
- Zarghooni2012 Article TreatmentOfSpondylodiscitisDocument7 pagesZarghooni2012 Article TreatmentOfSpondylodiscitisRoxana StanciuNo ratings yet
- Ankylosing Spondylitis...Document6 pagesAnkylosing Spondylitis...mfahrizaNo ratings yet
- Pola 2017Document10 pagesPola 2017RobertoNo ratings yet
- 6-Article Text-190-2-10-20200107Document10 pages6-Article Text-190-2-10-20200107bookNo ratings yet
- Bland 1984Document28 pagesBland 1984Hellmann Adrian Escobar CNo ratings yet
- Prophylactic Use of Antibiotics and Immunisations in Patients With SLEDocument2 pagesProphylactic Use of Antibiotics and Immunisations in Patients With SLEPrima AndikacitraNo ratings yet
- Necrotising Fasciitis or Pyoderma Gangrenosum: A Fatal DilemmaDocument8 pagesNecrotising Fasciitis or Pyoderma Gangrenosum: A Fatal DilemmayuktianaNo ratings yet
- EpicondilteDocument7 pagesEpicondilteRicardo fariaNo ratings yet
- Ankylosing Spondylitis: Pathophysiology, Clinical Features, and ManagementDocument10 pagesAnkylosing Spondylitis: Pathophysiology, Clinical Features, and ManagementWie SeptiaNiNo ratings yet
- Spondyloarthritis: by Aishwarya Prasad Roll No 6Document22 pagesSpondyloarthritis: by Aishwarya Prasad Roll No 6irsyadilfikriNo ratings yet
- Discitis and Spinal Infection: Classi Fication and EpidemiologyDocument5 pagesDiscitis and Spinal Infection: Classi Fication and Epidemiologyraul ramboyongNo ratings yet
- AR para ManosDocument22 pagesAR para ManosAndres CasteloNo ratings yet
- Prophylactic Use of Antibiotics and Immunisations in Patients With SLEDocument2 pagesProphylactic Use of Antibiotics and Immunisations in Patients With SLEbhavya sharmaNo ratings yet
- Polymyalgia Rheumatica - Lancet (2023)Document14 pagesPolymyalgia Rheumatica - Lancet (2023)1DMANUEL Suarez MejiaNo ratings yet
- Musculo-Skeletal Disorders - Polymalagia ArthritisDocument22 pagesMusculo-Skeletal Disorders - Polymalagia ArthritisKyle J. NortonNo ratings yet
- 5253 21764 5 PBDocument8 pages5253 21764 5 PBZuraidaNo ratings yet
- An Approach To A Child With ArthritisDocument9 pagesAn Approach To A Child With Arthritispadamati govardhan reddy reddyNo ratings yet
- Jurnal 5Document7 pagesJurnal 5Putri Maghfirah BahriNo ratings yet
- Infectious Spondylodiscitis - A Case Series AnalysisDocument4 pagesInfectious Spondylodiscitis - A Case Series AnalysisCarlos Pacichana AgudeloNo ratings yet
- Revision bertolottiDocument8 pagesRevision bertolottiOscar Cayetano Herrera RodríguezNo ratings yet
- Guillian BarrettDocument12 pagesGuillian BarrettOmar MadrigalNo ratings yet
- Rheumatoid ArthritisDocument23 pagesRheumatoid Arthritisfabunmiopeyemiv23No ratings yet
- 2019 Estado de La Unión. Revisión de Las Indicaciones y Técnicas de Fusión Lumbar para La Enfermedad Degenerativa de La ColumnaDocument14 pages2019 Estado de La Unión. Revisión de Las Indicaciones y Técnicas de Fusión Lumbar para La Enfermedad Degenerativa de La Columnajuan pabloNo ratings yet
- Letters To The Editors: Primary Sjögren's Syndrome As Paraneoplastic Disorder: A Case ReportDocument1 pageLetters To The Editors: Primary Sjögren's Syndrome As Paraneoplastic Disorder: A Case ReportDarian AngNo ratings yet
- Polymyalgia Rheumatica Diagnosis and TreatmentDocument23 pagesPolymyalgia Rheumatica Diagnosis and TreatmentArtika MayandaNo ratings yet
- Ankylosing Spondylitis and Undifferentiated SpondyloarthropathyDocument33 pagesAnkylosing Spondylitis and Undifferentiated Spondyloarthropathylbc-602No ratings yet
- Bydon 2019Document6 pagesBydon 2019julyanetorquatoNo ratings yet
- Koes2006 PDFDocument5 pagesKoes2006 PDFDewi FathmahNo ratings yet
- Polymyalgia Rheumatica 2023Document14 pagesPolymyalgia Rheumatica 2023Carlos Alfredo Vargas Quintero100% (1)
- Behcet's Disease: Authors: Jagdish R NairDocument7 pagesBehcet's Disease: Authors: Jagdish R NairsalclNo ratings yet
- Treatment of Postherpetic Neuralgia With Low Level Laser TherapyDocument7 pagesTreatment of Postherpetic Neuralgia With Low Level Laser TherapyJason GossNo ratings yet
- Psoriatic ArthritisDocument12 pagesPsoriatic ArthritisSelvia RosadiNo ratings yet
- Ankylosing Spondylitis: Causes, Symptoms, and Treatment OptionsDocument3 pagesAnkylosing Spondylitis: Causes, Symptoms, and Treatment OptionsMa OlayaNo ratings yet
- Cronicon: Clinical Case Study Clinical Manifestation, Diagnosis, Treatment and Prevention of Leprosy: An UpdateDocument4 pagesCronicon: Clinical Case Study Clinical Manifestation, Diagnosis, Treatment and Prevention of Leprosy: An Updatetifa adaNo ratings yet
- Journal of Internal Medicine - 2022 - Lundberg - An Update On Polymyalgia RheumaticaDocument16 pagesJournal of Internal Medicine - 2022 - Lundberg - An Update On Polymyalgia RheumaticaDenisa Carmen ColiofNo ratings yet
- Pott 6Document8 pagesPott 6Jeanie WangsaNo ratings yet
- Refractory Chronic Rhinosinusitis: Etiology & Management: November 2011Document15 pagesRefractory Chronic Rhinosinusitis: Etiology & Management: November 2011Christian VieryNo ratings yet
- An Update On Polymyalgia RheumaticaDocument16 pagesAn Update On Polymyalgia RheumaticaGian CarloNo ratings yet
- Nejmcp 2032396Document10 pagesNejmcp 2032396juan carlosNo ratings yet
- Chapter 3. Inflammatory Rheumatic DisorderDocument37 pagesChapter 3. Inflammatory Rheumatic DisorderMika KresnaNo ratings yet
- Banderas RojasDocument5 pagesBanderas RojasLucía TrilloNo ratings yet
- Fundamentals of Rheumatoid Arthritis and Various Homoeopathic Trials in Patients of Rheumatoid Arthritis: An UpdateDocument6 pagesFundamentals of Rheumatoid Arthritis and Various Homoeopathic Trials in Patients of Rheumatoid Arthritis: An UpdateHomoeopathic PulseNo ratings yet
- Vertebral Fractures: Clinical PracticeDocument9 pagesVertebral Fractures: Clinical PracticeIndraYudhiNo ratings yet
- Ischemic Pain in The Extremities and Raynaud's PhenomenonDocument12 pagesIschemic Pain in The Extremities and Raynaud's PhenomenonRaiyanNo ratings yet
- Lumbosacral Radiculopathy - StatPearls - NCBI BookshelfDocument5 pagesLumbosacral Radiculopathy - StatPearls - NCBI BookshelfmusdalifahNo ratings yet
- Patient - Info/doctor/ankylosing Spondylitis ProDocument8 pagesPatient - Info/doctor/ankylosing Spondylitis ProJasleen KaurNo ratings yet
- 4.the Pathogenesis of Psoriatic ArthritisDocument12 pages4.the Pathogenesis of Psoriatic ArthritisstuckinbedNo ratings yet
- Transverse Myelitis: Clinical PracticeDocument9 pagesTransverse Myelitis: Clinical PracticearnabNo ratings yet
- Small Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationFrom EverandSmall Fiber Neuropathy and Related Syndromes: Pain and NeurodegenerationSung-Tsang HsiehNo ratings yet
- Neuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related DiseasesFrom EverandNeuroimmunology: Multiple Sclerosis, Autoimmune Neurology and Related DiseasesAmanda L. PiquetNo ratings yet
- Jadwal Jaga Ruangan Covid 19Document1 pageJadwal Jaga Ruangan Covid 19occha_fun08No ratings yet
- Stability of Intravenous Vitamin C Solutions A Tehnical ReportDocument2 pagesStability of Intravenous Vitamin C Solutions A Tehnical Reportoccha_fun08No ratings yet
- ABSTRACTDocument1 pageABSTRACToccha_fun08No ratings yet
- Chindy Tulyabu Presentasi Bhs - InggrisDocument7 pagesChindy Tulyabu Presentasi Bhs - Inggrisoccha_fun08No ratings yet
- Laporan Kinerja Lab Per Pasien Pemeriksaan 2022-10-14 S - D 2022-10-14Document72 pagesLaporan Kinerja Lab Per Pasien Pemeriksaan 2022-10-14 S - D 2022-10-14LaboratoriumNo ratings yet
- DSM-5 Criteria for PTSDDocument1 pageDSM-5 Criteria for PTSDMarial JavierNo ratings yet
- Sensors 22 06606Document12 pagesSensors 22 06606Barbara Rebeca De Macedo PinheiroNo ratings yet
- 2021-Editorial - Defining The Clinical Boundary of Disruptive Mood Dysregulation Disorder Symptoms in YouthDocument3 pages2021-Editorial - Defining The Clinical Boundary of Disruptive Mood Dysregulation Disorder Symptoms in YouthCaio MayrinkNo ratings yet
- Funda Chapter 10 14Document6 pagesFunda Chapter 10 14Kara Kristine TuanoNo ratings yet
- Diagnostics 13 00220Document20 pagesDiagnostics 13 00220msworkbbhNo ratings yet
- Final Exam RreviewDocument15 pagesFinal Exam Rreviewslg233No ratings yet
- Convergence The Future of Health 2016 ReportDocument80 pagesConvergence The Future of Health 2016 ReportKrishnakumar KattarakunnuNo ratings yet
- Health Insurance Nonlife Commercial Data Analysis Report 201617Document14 pagesHealth Insurance Nonlife Commercial Data Analysis Report 201617Mayank AamseekNo ratings yet
- Obsessive-Compulsive Disorder (OCD)Document16 pagesObsessive-Compulsive Disorder (OCD)Yousef A. MehdawiNo ratings yet
- Fall 1 Professional Development PlanDocument9 pagesFall 1 Professional Development Planapi-681176565No ratings yet
- Pharmacology in Nursing - 3Document4 pagesPharmacology in Nursing - 3Buat UmumNo ratings yet
- Psych Abnormal Child Psychology - 6th Edition (2015) - 1-50-3-10Document8 pagesPsych Abnormal Child Psychology - 6th Edition (2015) - 1-50-3-10tin_ally9059No ratings yet
- Thompson Elder Davis Iii, PH.DDocument30 pagesThompson Elder Davis Iii, PH.DLeonard MpezeniNo ratings yet
- ManiaDocument10 pagesManiaaashvi dalalNo ratings yet
- CHN in House Module 1Document7 pagesCHN in House Module 1Catherine AteradoNo ratings yet
- DSMDocument2 pagesDSMOtilia EmaNo ratings yet
- Aspergillus and Other Respiratory Fungal Infections in The ICU Diagnosis and Management 2018Document7 pagesAspergillus and Other Respiratory Fungal Infections in The ICU Diagnosis and Management 2018ferrevNo ratings yet
- Preceptor Orientation HandbookDocument13 pagesPreceptor Orientation HandbookStarr NewmanNo ratings yet
- FnpresumeDocument5 pagesFnpresumeapi-705700900No ratings yet
- Reflection PaperDocument4 pagesReflection PaperMary Lyn BesmonteNo ratings yet