You might also like
- Version 10.1 and Later - Arcgis For Desktop Student Trial Software InstructionsDocument2 pagesVersion 10.1 and Later - Arcgis For Desktop Student Trial Software InstructionsRisqi FadlyNo ratings yet
- Variation and Trend of Sea Level Derived From Altimetry Satellite and Tide Gauge in Cilacap and Benoa Coastal AreasDocument8 pagesVariation and Trend of Sea Level Derived From Altimetry Satellite and Tide Gauge in Cilacap and Benoa Coastal AreasRisqi FadlyNo ratings yet
- Accepted Manuscript: 10.1016/j.ypmed.2017.08.003Document29 pagesAccepted Manuscript: 10.1016/j.ypmed.2017.08.003Risqi FadlyNo ratings yet
- Hurricane Isaac Storm Surges Off Florida Observed by Jason-1 and Jason-2 Satellite AltimetersDocument10 pagesHurricane Isaac Storm Surges Off Florida Observed by Jason-1 and Jason-2 Satellite AltimetersRisqi FadlyNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Differences Between OHS Management System StandardsDocument27 pagesThe Differences Between OHS Management System StandardsRommel100% (2)
- Accomplishment Report: Gubat National High SchoolDocument2 pagesAccomplishment Report: Gubat National High SchoolSheila Divinagracia - EscobedoNo ratings yet
- Bash SHELL Script in LinuxDocument6 pagesBash SHELL Script in LinuxHesti WidyaNo ratings yet
- PH G12 S1Document9 pagesPH G12 S1mahmoudNo ratings yet
- Deiparine, Jr. vs. Court of Appeals, 221 SCRA 503, G.R. No. 96643 April 23, 1993Document9 pagesDeiparine, Jr. vs. Court of Appeals, 221 SCRA 503, G.R. No. 96643 April 23, 1993CherNo ratings yet
- Automobile Engineering NotesDocument120 pagesAutomobile Engineering Notesakshay2992No ratings yet
- Hot-Rolled Steel Beam Calculation To AISC 360-16Document2 pagesHot-Rolled Steel Beam Calculation To AISC 360-16vanda_686788867No ratings yet
- Purple Futuristic Pitch Deck PresentationDocument10 pagesPurple Futuristic Pitch Deck PresentationRidzki F.RNo ratings yet
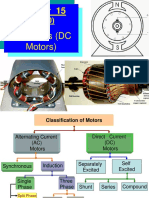
- Chapter 15.1.2.3 DC Drives PPT II Spring 2012Document56 pagesChapter 15.1.2.3 DC Drives PPT II Spring 2012Muhammad Saqib Noor Ul IslamNo ratings yet
- Geosynthetics and Geosynthetics and Reinforced Soil StructuresDocument22 pagesGeosynthetics and Geosynthetics and Reinforced Soil StructuresOscar FoxNo ratings yet
- Omni Bas Outdoor Product CatalogDocument70 pagesOmni Bas Outdoor Product CatalogVladislav GordeevNo ratings yet
- RBI Assistant Prelims 14 Feb 2020 Memory Based Paper (English)Document27 pagesRBI Assistant Prelims 14 Feb 2020 Memory Based Paper (English)AbhiNo ratings yet
- 1570-Article Text-4693-1-10-20190709Document18 pages1570-Article Text-4693-1-10-20190709Innocent PhiriNo ratings yet
- Lesson Plan PRKADocument2 pagesLesson Plan PRKAAmieer Abdul RahimNo ratings yet
- Transportation Research Part C: Xiaojie Luan, Francesco Corman, Lingyun MengDocument27 pagesTransportation Research Part C: Xiaojie Luan, Francesco Corman, Lingyun MengImags GamiNo ratings yet
- Last Boat Not Least - An Unofficial Adventure For Fallout 2d20Document14 pagesLast Boat Not Least - An Unofficial Adventure For Fallout 2d20Veritas Veritati100% (3)
- Please Get Rid of That SmellDocument4 pagesPlease Get Rid of That Smellmcant1980No ratings yet
- C Band Polarimetric Doppler Weather Radar Observations During An Extreme Precipitation Event and Associated Dynamics Over Peninsular IndiaDocument16 pagesC Band Polarimetric Doppler Weather Radar Observations During An Extreme Precipitation Event and Associated Dynamics Over Peninsular Indiamann singh100% (1)
- Rwanda National Examinations Council Organisational Chart DeputyDocument1 pageRwanda National Examinations Council Organisational Chart DeputymugobokaNo ratings yet
- Staff Perception of Respect For Human Rights of Users and Organizational Well-Being: A Study in Four Different Countries of The Mediterranean AreaDocument7 pagesStaff Perception of Respect For Human Rights of Users and Organizational Well-Being: A Study in Four Different Countries of The Mediterranean Areakhouloud razkiNo ratings yet
- Tanner EDA Tools v16.3 Release NotesDocument60 pagesTanner EDA Tools v16.3 Release NotesMohiuddin Mohammad100% (1)
- Moxa Eds 2005 El Series Datasheet v1.3 PDFDocument3 pagesMoxa Eds 2005 El Series Datasheet v1.3 PDFPatrick RNo ratings yet
- RSLogix 5000 Report(s) 120511Document74 pagesRSLogix 5000 Report(s) 120511Renji JacobNo ratings yet
- Thesis SoilDocument91 pagesThesis SoilmadhanNo ratings yet
- SSP700ADocument4 pagesSSP700AKanwar Bir SinghNo ratings yet
- Group 1 ResearchDocument16 pagesGroup 1 ResearchSaedamenNo ratings yet
- Ooip Volume MbeDocument19 pagesOoip Volume Mbefoxnew11No ratings yet
- SAES-L-610 PDF Download - Nonmetallic Piping in Oily Water Services - PDFYARDocument6 pagesSAES-L-610 PDF Download - Nonmetallic Piping in Oily Water Services - PDFYARZahidRafiqueNo ratings yet
- HRM Chapt 4 With AnswersDocument3 pagesHRM Chapt 4 With Answersjoebloggs1888No ratings yet
- Contoh Implementasi QMSDocument8 pagesContoh Implementasi QMSIINNo ratings yet