You might also like
- Annex C RR 11-2018Document1 pageAnnex C RR 11-2018Rheneir MoraNo ratings yet
- Certificate of AttendanceDocument7 pagesCertificate of Attendancemedelyn trinidad100% (1)
- Dasmariñas Lending Services: Loan Application FormDocument3 pagesDasmariñas Lending Services: Loan Application FormMark RyeNo ratings yet
- Transfer Commitment FormDocument1 pageTransfer Commitment Formromarcambri100% (5)
- Completete SET OF HR FORMSDocument9 pagesCompletete SET OF HR FORMSALEXANDER DIMAFELIX JR.No ratings yet
- Salesperson's Letter of EngagementDocument1 pageSalesperson's Letter of Engagementacelaerden67% (3)
- Certificate of Appearance 1Document3 pagesCertificate of Appearance 1Barangay PalabotanNo ratings yet
- ID Application FormsDocument5 pagesID Application Formskez leigh Amber100% (1)
- Annex C RR 11 2018 PDFDocument1 pageAnnex C RR 11 2018 PDFMahko albert RslesNo ratings yet
- Malware: CC101 - Introduction To ComputingDocument11 pagesMalware: CC101 - Introduction To ComputingMelx UbaldeNo ratings yet
- HRF-2021-001 Change Day-Off and Change Shift FormDocument1 pageHRF-2021-001 Change Day-Off and Change Shift FormEmy Salvador100% (1)
- RR 11 2018 - Annex C - Withholding Agent Sworn DeclarationDocument1 pageRR 11 2018 - Annex C - Withholding Agent Sworn DeclarationJames Salviejo Pineda100% (1)
- RR 11-2018 Income Payor Sworn DeclarationDocument1 pageRR 11-2018 Income Payor Sworn DeclarationMaricel Valerio CanlasNo ratings yet
- Quitclaim and Waiver of ClaimsDocument2 pagesQuitclaim and Waiver of ClaimsJosh Ko PoNo ratings yet
- Certificate of AppearanceDocument2 pagesCertificate of AppearanceConselvien Juno Limson AsoyNo ratings yet
- APPEARANCEDocument8 pagesAPPEARANCERenzelNo ratings yet
- Certificate of Appearance: Prudencia Du-De Sagun Dentist Ii MHODocument1 pageCertificate of Appearance: Prudencia Du-De Sagun Dentist Ii MHOangel_sagun_1No ratings yet
- Wei Yuan Quitclaim and ReleaseDocument1 pageWei Yuan Quitclaim and ReleaseMark Anthony RojoNo ratings yet
- Clearance FormDocument3 pagesClearance FormArvin BegasoNo ratings yet
- Co Signers Statement2Document2 pagesCo Signers Statement2Pharmastar Int'l Trading Corp.No ratings yet
- Co Signers Statement2Document2 pagesCo Signers Statement2Pharmastar Int'l Trading Corp.No ratings yet
- Blank CADocument2 pagesBlank CAJaypee ApitNo ratings yet
- Barangay Health Worker Registration FormDocument1 pageBarangay Health Worker Registration FormJairah MarieNo ratings yet
- Extension of StayDocument1 pageExtension of StayAlex GatsulaoNo ratings yet
- Notice of Client RegistrationDocument1 pageNotice of Client RegistrationShadow BearNo ratings yet
- Pensioner-Update-Form 2Document1 pagePensioner-Update-Form 2JENET JAENANo ratings yet
- ANNEX - Life Cert, Non Emploment & Non MarriageDocument1 pageANNEX - Life Cert, Non Emploment & Non Marriagealbertsuhaib13No ratings yet
- Certificate of AppearanceDocument1 pageCertificate of AppearanceErnest AbiertasNo ratings yet
- Annex C RR 11-2018Document1 pageAnnex C RR 11-2018Yreced Gabison ResmaNo ratings yet
- Annex C RR 11-2018Document1 pageAnnex C RR 11-2018Yreced Gabison ResmaNo ratings yet
- Annex C RR 11-2018Document1 pageAnnex C RR 11-2018zetajrrogelioNo ratings yet
- Landero Clinic and Hospital: Notice of ChargeDocument1 pageLandero Clinic and Hospital: Notice of ChargeQuennie Marie Moreno VillanuevaNo ratings yet
- Annex C RR 11 2018Document1 pageAnnex C RR 11 2018Rico SengcoNo ratings yet
- Cert of Appearance UploadDocument2 pagesCert of Appearance UploadVMNo ratings yet
- Annex C RR 11-2018Document1 pageAnnex C RR 11-2018JeZkYNo ratings yet
- Annex C RR 11-2018Document1 pageAnnex C RR 11-2018jayNo ratings yet
- RR 11 2018 - Annex C - Withholding Agent Sworn DeclarationDocument1 pageRR 11 2018 - Annex C - Withholding Agent Sworn DeclarationJames Salviejo PinedaNo ratings yet
- Annex C RR NEW FORMDocument1 pageAnnex C RR NEW FORMEdward Dwayne BringasNo ratings yet
- Annex C RR 11-2018Document1 pageAnnex C RR 11-2018Rheneir MoraNo ratings yet
- Annex C RR 11-2018Document1 pageAnnex C RR 11-2018KB WorldNo ratings yet
- Annex C RR 11-2018Document1 pageAnnex C RR 11-2018grecelyn bianesNo ratings yet
- RR 11 2018 - Annex C - Withholding Agent Sworn DeclarationDocument1 pageRR 11 2018 - Annex C - Withholding Agent Sworn DeclarationLizabeth PeñaNo ratings yet
- Annex C RR 11-2018Document1 pageAnnex C RR 11-2018Alyk CalionNo ratings yet
- RR 11 2018 - Annex C - Withholding Agent Sworn DeclarationDocument1 pageRR 11 2018 - Annex C - Withholding Agent Sworn DeclarationPatOcampoNo ratings yet
- Certificate of AppearanceDocument1 pageCertificate of AppearanceBarangay DicolocNo ratings yet
- Applicant Application FormDocument6 pagesApplicant Application FormJocelyn Joy ArcegaNo ratings yet
- Certificate of Appearance: Republic of The Philippines Province of Zamboanga Del Sur Provincial Press BureauDocument5 pagesCertificate of Appearance: Republic of The Philippines Province of Zamboanga Del Sur Provincial Press BureauYeshua TuraNo ratings yet
- Application To Purchase A House and Lot Package/Housing Unit Under The Government Employees Housing ProgramDocument3 pagesApplication To Purchase A House and Lot Package/Housing Unit Under The Government Employees Housing ProgramrichardNo ratings yet
- Secretary CertDocument1 pageSecretary CertLegal GroupNo ratings yet
- Certificate of Appearance: National Housing AuthorityDocument1 pageCertificate of Appearance: National Housing AuthorityEdbert Gio SuanNo ratings yet
- AEP Application FormDocument2 pagesAEP Application FormRenadelyn GombaNo ratings yet
- 47a 2 APPLICATION FORMDocument8 pages47a 2 APPLICATION FORMJohn Lawrence de lunaNo ratings yet
- Application FormDocument2 pagesApplication FormJuan LucioNo ratings yet
- 000 Affidavit of No OperationDocument1 page000 Affidavit of No OperationMichelle Lalaine DiazNo ratings yet
- Affidavit of Undertaking Sra ISODocument2 pagesAffidavit of Undertaking Sra ISONLainie OmarNo ratings yet
- Business Permit FormDocument1 pageBusiness Permit FormcharlotteNo ratings yet
- Sec CertDocument1 pageSec CertPhilip Frantz GuerreroNo ratings yet
- EC Grievance Intake FormDocument1 pageEC Grievance Intake FormJelyn BujatinNo ratings yet
- Affidavit of Business RetirementDocument1 pageAffidavit of Business RetirementMaghari Pongyan John RalphNo ratings yet
- The Stress-Free Guide to Parenting a Child With ADHD: Effective and Proven Strategies for Alleviating Anxiety and Forming Strong Bonds Without the HassleFrom EverandThe Stress-Free Guide to Parenting a Child With ADHD: Effective and Proven Strategies for Alleviating Anxiety and Forming Strong Bonds Without the HassleNo ratings yet
- Chapter 3 v1Document9 pagesChapter 3 v1Melx UbaldeNo ratings yet
- Review of Related Literature/SystemsDocument5 pagesReview of Related Literature/SystemsMelx UbaldeNo ratings yet
- Appendices Deliverables and MilestoneDocument3 pagesAppendices Deliverables and MilestoneMelx UbaldeNo ratings yet
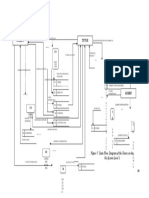
- Parent Tutor: Figure 7. Data Flow Diagram of The Tutors On The Go System Level 1Document1 pageParent Tutor: Figure 7. Data Flow Diagram of The Tutors On The Go System Level 1Melx UbaldeNo ratings yet
- Chapter 3Document16 pagesChapter 3Melx UbaldeNo ratings yet
- Statement of The ProblemDocument4 pagesStatement of The ProblemMelx UbaldeNo ratings yet
- Is304 - PHP - Mysql For Web Application DevelopmentDocument2 pagesIs304 - PHP - Mysql For Web Application DevelopmentMelx UbaldeNo ratings yet
- Catanduanes National High SchoolDocument1 pageCatanduanes National High SchoolMelx Ubalde100% (1)
- Problem. Redundancy of Information, Unmanage Statement of Accounts SolutionDocument7 pagesProblem. Redundancy of Information, Unmanage Statement of Accounts SolutionMelx UbaldeNo ratings yet
- O Title O Executive SummaryDocument11 pagesO Title O Executive SummaryMelx UbaldeNo ratings yet
- Criterion ReferenceDocument4 pagesCriterion ReferenceMelx UbaldeNo ratings yet
- Scientific Plant 2Document10 pagesScientific Plant 2Melx UbaldeNo ratings yet
- Name: - Date: - ScoreDocument3 pagesName: - Date: - ScoreMelx UbaldeNo ratings yet
- Evolution of ComputingDocument21 pagesEvolution of ComputingMelx UbaldeNo ratings yet
- Mangifera Indica (Mango) : DescriptionDocument10 pagesMangifera Indica (Mango) : DescriptionMelx UbaldeNo ratings yet
- What Are The Parts of Respiratory System With FunctionsDocument3 pagesWhat Are The Parts of Respiratory System With FunctionsMelx UbaldeNo ratings yet
- Bangladesh Is Located in South Asia and Bordered by The Bay of Bengal, India, and MyanmarDocument5 pagesBangladesh Is Located in South Asia and Bordered by The Bay of Bengal, India, and MyanmarMelx UbaldeNo ratings yet
- ProcessorDocument1 pageProcessorMelx UbaldeNo ratings yet
- Presentation 1qweqwe1123aDocument6 pagesPresentation 1qweqwe1123aMelx UbaldeNo ratings yet
- Shirley T. Ocray: Viga Central Elementary SchoolDocument1 pageShirley T. Ocray: Viga Central Elementary SchoolMelx Ubalde0% (1)
- Key Components of A Computer SystemDocument18 pagesKey Components of A Computer SystemMelx UbaldeNo ratings yet
- AngelaDocument2 pagesAngelaMelx UbaldeNo ratings yet
- A1Document5 pagesA1Melx UbaldeNo ratings yet