You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- 10 FBS Q2M3 Tle10 - He - Food - Beverageservices - q2 - Mod3 - Takingfoodandbeverageorders - v3 (27 Pages)Document28 pages10 FBS Q2M3 Tle10 - He - Food - Beverageservices - q2 - Mod3 - Takingfoodandbeverageorders - v3 (27 Pages)LISANDRA JOMERO100% (2)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Privacy Persuasive EssayDocument3 pagesPrivacy Persuasive Essayapi-251934738No ratings yet
- English For Csec PAPER 1 (1 Hour 30 Minutes) - 60 Multiple Choice ItemsDocument2 pagesEnglish For Csec PAPER 1 (1 Hour 30 Minutes) - 60 Multiple Choice ItemsAqilah MahabirNo ratings yet
- Work-Related Musculoskeletal Disorders Among Health Care Professionals - A Cross-Sectional Assessment of Risk Factors in A Tertiary Hospital, IndiaDocument14 pagesWork-Related Musculoskeletal Disorders Among Health Care Professionals - A Cross-Sectional Assessment of Risk Factors in A Tertiary Hospital, IndiaAqilah MahabirNo ratings yet
- Supplementary Information: Table S1. The Basic Hygiene Information of 13 Factories Participated in This StudyDocument5 pagesSupplementary Information: Table S1. The Basic Hygiene Information of 13 Factories Participated in This StudyAqilah MahabirNo ratings yet
- HPLC LCMS Lab ReportDocument3 pagesHPLC LCMS Lab ReportAqilah Mahabir100% (1)
- Chemistry of Transition MetalsDocument44 pagesChemistry of Transition MetalsAqilah MahabirNo ratings yet
- Symmetry and Group TheoryDocument129 pagesSymmetry and Group TheoryMatthew HansenNo ratings yet
- Specifications For Commonly Used Fertilizers: 1. N, P and K FertilizersDocument9 pagesSpecifications For Commonly Used Fertilizers: 1. N, P and K FertilizersAqilah MahabirNo ratings yet
- Control ChartsDocument36 pagesControl ChartsGulshan KandaNo ratings yet
- An ADocument1 pageAn AAqilah MahabirNo ratings yet
- Introduction/Theory:: EXPERIMENT 3: The Determination of Calcium in Milk by EDTA TitrationDocument5 pagesIntroduction/Theory:: EXPERIMENT 3: The Determination of Calcium in Milk by EDTA TitrationAqilah Mahabir100% (1)
- The Determination of Calcium in Milk by EDTA TitrationDocument6 pagesThe Determination of Calcium in Milk by EDTA TitrationAqilah MahabirNo ratings yet
- Spaces One Liners in The BodyDocument16 pagesSpaces One Liners in The BodyRatan YadavNo ratings yet
- WORKSHEETS With RUBRICSDocument5 pagesWORKSHEETS With RUBRICSMichael MalvarNo ratings yet
- Tugas Mike P5-3ADocument6 pagesTugas Mike P5-3Awinda dwi lestariNo ratings yet
- First Periodical Test in Science 6Document8 pagesFirst Periodical Test in Science 6Mayette Pamilara Payaban100% (4)
- Environmetal Science Ste 7 Quarter 1 Module 1 2Document7 pagesEnvironmetal Science Ste 7 Quarter 1 Module 1 2LA SamonteNo ratings yet
- Diseases of The Uveal Tract 09Document24 pagesDiseases of The Uveal Tract 09somebody_ma100% (7)
- 1 Part Kali Linux Questions-3Document6 pages1 Part Kali Linux Questions-3muzammalsafdarNo ratings yet
- Carbonyl Compounds NotesDocument10 pagesCarbonyl Compounds NotesCBIT CIVIL A1No ratings yet
- Customer Segmentation ProfilingDocument9 pagesCustomer Segmentation ProfilingKrishnan SampathNo ratings yet
- FP Plus™: Enhanced' Fire Resistant Cable 300/500 VDocument7 pagesFP Plus™: Enhanced' Fire Resistant Cable 300/500 VBhagoo HatheyNo ratings yet
- Vinay Bharadwaj DS (2147326)Document4 pagesVinay Bharadwaj DS (2147326)VINAY BHARADWAJ DS 2147326No ratings yet
- Mother by Grace PaleyDocument9 pagesMother by Grace Paleylourdes.pereirorodriguezNo ratings yet
- DBR Winning ApproachDocument9 pagesDBR Winning ApproachDiego Andrés Triana RodríguezNo ratings yet
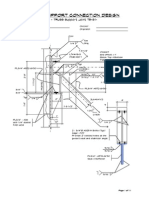
- Truss Support Connection Design T5-S1Document11 pagesTruss Support Connection Design T5-S1rajedmaglinteNo ratings yet
- Learning Objectives: Meeting 7 Checking Vital SignsDocument4 pagesLearning Objectives: Meeting 7 Checking Vital SignsWhy Sung LoongNo ratings yet
- Bandra Worli Sea LinkDocument40 pagesBandra Worli Sea LinkNishit Shah100% (2)
- Cell As A Unit of Life (Science Form 1 - Short Notes)Document2 pagesCell As A Unit of Life (Science Form 1 - Short Notes)jrpyroNo ratings yet
- Virtual CockpitDocument10 pagesVirtual CockpitNavaneeth Krishnan BNo ratings yet
- DisertacijaDocument157 pagesDisertacijakontiki500No ratings yet
- Grade 7-Exploratory-Agri-Cookery-Carpentry-Css - PretestDocument4 pagesGrade 7-Exploratory-Agri-Cookery-Carpentry-Css - PretestNANCY BADINGNo ratings yet
- Chapter 1 OutlineDocument3 pagesChapter 1 OutlineConi ChanNo ratings yet
- Offering Letter Aston BNR Bogor Hotel 2024Document3 pagesOffering Letter Aston BNR Bogor Hotel 2024rc.simbaraNo ratings yet
- Science Education - 2000 - She - The Development of A Questionnaire To Describe Science Teacher Communication Behavior inDocument21 pagesScience Education - 2000 - She - The Development of A Questionnaire To Describe Science Teacher Communication Behavior inAshraf OmarNo ratings yet
- Resume Sonu WMSDocument4 pagesResume Sonu WMSsomyaNo ratings yet
- L-5 Hypothesis TestsDocument22 pagesL-5 Hypothesis TestsAbdo RawiNo ratings yet
- Unpivot Columns - BasicsDocument7 pagesUnpivot Columns - BasicsLeonardo GeovanniNo ratings yet
- Price Discrimination Under Monopoly: Types, Degrees and Other DetailsDocument18 pagesPrice Discrimination Under Monopoly: Types, Degrees and Other DetailsSanchit BabbarNo ratings yet
- Sectors of The Indian EconomyDocument36 pagesSectors of The Indian EconomyJJS PackagingNo ratings yet