You might also like
- Case Study On AsthmaDocument3 pagesCase Study On AsthmaNurudeen Ibrahim100% (1)
- Biochemistry Exam 1 ReviewDocument37 pagesBiochemistry Exam 1 ReviewThomas B.100% (1)
- Nutritional Biochemistry: Vitamins Dr. Bidhan Chandra KonerDocument50 pagesNutritional Biochemistry: Vitamins Dr. Bidhan Chandra KonerElenanana100% (1)
- Vitamins and CoenzymesDocument46 pagesVitamins and CoenzymesPertunia MulatedziNo ratings yet
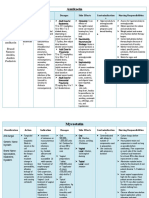
- AmikacinDocument4 pagesAmikacinkristineK100% (1)
- Indian DelegatesDocument156 pagesIndian DelegatesSumit KohliNo ratings yet
- Vitamin C ProductionDocument3 pagesVitamin C ProductionMozhi ArasuNo ratings yet
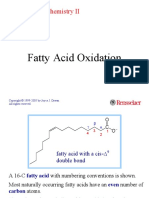
- Fatty Acid Oxidation: Molecular Biochemistry IIDocument39 pagesFatty Acid Oxidation: Molecular Biochemistry IIDozdi100% (1)
- MUPIROCINDocument2 pagesMUPIROCINNathalie kate petallarNo ratings yet
- WarfarinDocument25 pagesWarfarinSHIVAM BHASKARNo ratings yet
- Vitamins and Coenzymes PharmacyDocument55 pagesVitamins and Coenzymes PharmacywithneyNo ratings yet
- Metabolisme Vitamin EDocument23 pagesMetabolisme Vitamin ENietha Nyit-NyitNo ratings yet
- Metabolisme Vitamin EDocument22 pagesMetabolisme Vitamin EYossy HabibiNo ratings yet
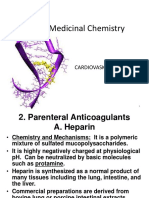
- ANTICOAGULANTSDocument64 pagesANTICOAGULANTSFrancisNo ratings yet
- Vitamins VitaminsDocument43 pagesVitamins VitaminsanaNo ratings yet
- 红苜蓿TpCYP98A44Document10 pages红苜蓿TpCYP98A44周正No ratings yet
- 5 AntihyperlipidemicDocument35 pages5 Antihyperlipidemicabdelrahmanmosleh75No ratings yet
- ANTIOKSIDANDocument25 pagesANTIOKSIDANnisa nisaNo ratings yet
- Cardiovascular Drugs 2Document41 pagesCardiovascular Drugs 2Mayurisman SpdNo ratings yet
- Gebauer 2007Document7 pagesGebauer 2007masssssoudNo ratings yet
- Water Sol Vit CDocument26 pagesWater Sol Vit CShujaNo ratings yet
- DiureticsDocument75 pagesDiureticsSilpa Jayakumar100% (5)
- Metabolic Pathways For Protein and Amino Acids: Dr. Lilia Dewiyanti, Spa, MsimedDocument37 pagesMetabolic Pathways For Protein and Amino Acids: Dr. Lilia Dewiyanti, Spa, MsimedLa Ode RinaldiNo ratings yet
- GivocalDocument25 pagesGivocalnadea100% (1)
- Metabolisme Xenobiotik Metabolisme Xenobiotik: Toxicants BiotrasformationDocument42 pagesMetabolisme Xenobiotik Metabolisme Xenobiotik: Toxicants BiotrasformationTRIA SAPUTRA100% (1)
- Malaria MyDocument15 pagesMalaria Myshortsmotivation87No ratings yet
- Effects of Liver Disease On PharmacokineticsDocument50 pagesEffects of Liver Disease On PharmacokineticsAlex_LiveInDCNo ratings yet
- Lecture 15a-CatalysisDocument52 pagesLecture 15a-CatalysisNagarjuna VuchuruNo ratings yet
- Fatty Acid OxidationDocument43 pagesFatty Acid OxidationAmalia DarwisNo ratings yet
- Anti-Hypercholesterolemic Agents: Biosynthesis and Metabolism of CholesterolDocument20 pagesAnti-Hypercholesterolemic Agents: Biosynthesis and Metabolism of CholesterolAmarilys MoralesNo ratings yet
- Vitamins & LipidsDocument64 pagesVitamins & LipidsShimmering MoonNo ratings yet
- Drug Metabolism: Presenter:-Dr Swaroop H S Moderator: - DR Ananya ChakrabortyDocument38 pagesDrug Metabolism: Presenter:-Dr Swaroop H S Moderator: - DR Ananya Chakrabortyadinda keanayaNo ratings yet
- 1993 Bookmatter TheTechnologyOfVitaminsInFood PDFDocument24 pages1993 Bookmatter TheTechnologyOfVitaminsInFood PDFAndres GuzmanNo ratings yet
- Lipid MetabolismDocument32 pagesLipid MetabolismSaher YasinNo ratings yet
- Blood Thinners: Maher Khdour Clinical Pharmacy, BSC, MSC, PHDDocument68 pagesBlood Thinners: Maher Khdour Clinical Pharmacy, BSC, MSC, PHDYousef JafarNo ratings yet
- Glycosaminoglycans: (Mucopolysaccharides)Document50 pagesGlycosaminoglycans: (Mucopolysaccharides)AvinashNo ratings yet
- 12 Monosaccharide METABOLISMDocument72 pages12 Monosaccharide METABOLISMAnand VeerananNo ratings yet
- Vitamin CDocument38 pagesVitamin CDR JIJIN J UNo ratings yet
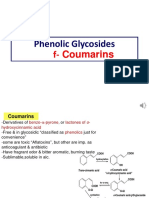
- Phenolic Glycosides: F-CoumarinsDocument6 pagesPhenolic Glycosides: F-CoumarinsNezar AlnasserNo ratings yet
- A Progressive Review On The Synthesis of Atovaquone (An Anti-Malarial Drug), Empowered by The Critical Examination of Prior-Art DisclosuresDocument21 pagesA Progressive Review On The Synthesis of Atovaquone (An Anti-Malarial Drug), Empowered by The Critical Examination of Prior-Art DisclosuresMediterr J Pharm Pharm SciNo ratings yet
- Vitamin CDocument50 pagesVitamin CMaya DasmaselaNo ratings yet
- IvacaftorDocument25 pagesIvacaftorSmart PharmacistNo ratings yet
- Lipid MetabolismDocument53 pagesLipid MetabolismbanyacskijuliusNo ratings yet
- Tony Durst-Diorio 124G, - Currently - Professor Emeritus ChemistryDocument35 pagesTony Durst-Diorio 124G, - Currently - Professor Emeritus ChemistrySumayah Al-SamiNo ratings yet
- Acetic Pathway: Fatty Acids and PolyketidesDocument70 pagesAcetic Pathway: Fatty Acids and PolyketidesChessy Rima MustikaNo ratings yet
- ProstaglandinsDocument43 pagesProstaglandinsRandy BrownNo ratings yet
- Baeyer Villiger Reaction: by Dr. Sabita Nayak Department of Chemistry Ravenshaw University Cuttack 07-11-2020Document15 pagesBaeyer Villiger Reaction: by Dr. Sabita Nayak Department of Chemistry Ravenshaw University Cuttack 07-11-2020suvam saiNo ratings yet
- Vitamin E & K-BdsDocument50 pagesVitamin E & K-BdsIsaiah JohnsonNo ratings yet
- 2020 Vit D IjhcDocument10 pages2020 Vit D IjhcAbdul SamadNo ratings yet
- Vitamin K: FAO/WHO Expert Consultation On Human Vitamin and Mineral RequirementsDocument18 pagesVitamin K: FAO/WHO Expert Consultation On Human Vitamin and Mineral RequirementsPaula Joy GarciaNo ratings yet
- Acid Based Disorders Med07Document28 pagesAcid Based Disorders Med07Salem Ali BawazeerNo ratings yet
- DR - N. Sivaranjani Asst. ProfDocument47 pagesDR - N. Sivaranjani Asst. ProfMaira MahmoodNo ratings yet
- Bioch CL 7. Enzime Utilizate in Diagnostic 20-21 (R+e)Document44 pagesBioch CL 7. Enzime Utilizate in Diagnostic 20-21 (R+e)Andrea ModestieNo ratings yet
- Tetracyclines: Dr. Md. Rageeb Md. Usman Associate Professor Department of PharmacognosyDocument21 pagesTetracyclines: Dr. Md. Rageeb Md. Usman Associate Professor Department of PharmacognosyAnonymous TCbZigVqNo ratings yet
- Lactic Acid Producing OrganismsDocument2 pagesLactic Acid Producing OrganismsUniversidad Prenatal TabarquinoNo ratings yet
- Antimalarial Agents: Department of Pharmaceutical ChemistryDocument52 pagesAntimalarial Agents: Department of Pharmaceutical ChemistryAkram KhanNo ratings yet
- Top Drugs - Clopidogrel BisulfateDocument17 pagesTop Drugs - Clopidogrel BisulfateThu Tra NguyễnNo ratings yet
- HBC 408 18Document34 pagesHBC 408 18Stanley ChikoveNo ratings yet
- Drug Design Metabolism 3Document19 pagesDrug Design Metabolism 3Hanaa HashemNo ratings yet
- Renal Tubular Acidosis - SUNILDocument62 pagesRenal Tubular Acidosis - SUNILSunil KumarNo ratings yet
- CaJacob JBC 1988 18640Document10 pagesCaJacob JBC 1988 18640richardhead1No ratings yet
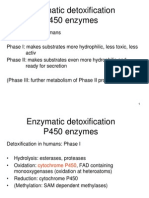
- Enzymatic Detoxification P450 EnzymesDocument22 pagesEnzymatic Detoxification P450 EnzymessayednourNo ratings yet
- Antioxidant Phenolic Metabolites From FRDocument57 pagesAntioxidant Phenolic Metabolites From FRElena MaderaNo ratings yet
- Esmeron and Clinical ExperienceDocument45 pagesEsmeron and Clinical ExperienceYasser Mohammed SharsharNo ratings yet
- So Ok Windi Nov 20Document16 pagesSo Ok Windi Nov 20Ruby BriandaNo ratings yet
- Pharmaceutical Preformulation: Liquid / Semisolid Dosage FormDocument20 pagesPharmaceutical Preformulation: Liquid / Semisolid Dosage FormKhalimatussaadahNo ratings yet
- Pharma NotesDocument69 pagesPharma NotesJawad Ahmad100% (1)
- Protein Binding of Drug: Page - 1 CMR College of Pharmacy, 2013Document18 pagesProtein Binding of Drug: Page - 1 CMR College of Pharmacy, 2013REDDYGAARI ABBAYINo ratings yet
- Daftar Harga Januari 2021Document5 pagesDaftar Harga Januari 2021andhy mallaranganNo ratings yet
- LED Light Therapy Consultation Form 1Document4 pagesLED Light Therapy Consultation Form 1infotandhmedicalNo ratings yet
- AVCN2 Session 1Document9 pagesAVCN2 Session 1Tram BanhNo ratings yet
- RECOVER Guidelines CompressedDocument28 pagesRECOVER Guidelines Compressedkkfyc2020No ratings yet
- Preanaesthetic Medication Anaesthetic Agents PDFDocument35 pagesPreanaesthetic Medication Anaesthetic Agents PDFSubhash BeraNo ratings yet
- Psilocybin Psychotherapy Systematic ReviewDocument14 pagesPsilocybin Psychotherapy Systematic ReviewAshok Kumar KrishnamoorthyNo ratings yet
- Drug Price TNMSCDocument13 pagesDrug Price TNMSCdrtpkNo ratings yet
- Drug Study Vit B ComplexDocument2 pagesDrug Study Vit B ComplexDeborah Mae MondoyNo ratings yet
- Clarification Billing by CGHS Empanelled Hospitals 10 Nov 22Document3 pagesClarification Billing by CGHS Empanelled Hospitals 10 Nov 22Nilesh SethNo ratings yet
- Asthma: Kaps PrepDocument21 pagesAsthma: Kaps PrepImee TingzonNo ratings yet
- Nutrition in SurgeryDocument23 pagesNutrition in SurgeryJayaram PandeyNo ratings yet
- Created by Unlicensed Version: Erd Healthone Medical DatabaseDocument1 pageCreated by Unlicensed Version: Erd Healthone Medical DatabaseGita Diaz Pangesti0% (1)
- Fall 2021 Longitudinal Ippe SyllabusDocument7 pagesFall 2021 Longitudinal Ippe Syllabusapi-602288180No ratings yet
- SRMJResDentSci2296-8008867 221448Document4 pagesSRMJResDentSci2296-8008867 221448Siddharth DhanarajNo ratings yet
- Failed Intubation Drill in The Emergency DepartmentDocument5 pagesFailed Intubation Drill in The Emergency DepartmentSuresh KumarNo ratings yet
- Administering Intradermal InjectionDocument17 pagesAdministering Intradermal InjectionPattNo ratings yet
- Tiotropium Bromide: Spiriva Handihaler, Spiriva RespimatDocument9 pagesTiotropium Bromide: Spiriva Handihaler, Spiriva RespimatAssem Ashraf KhidhrNo ratings yet
- Role of The Pharmacist in Proper Medication DisposalDocument12 pagesRole of The Pharmacist in Proper Medication DisposalDenise Yanci DemiarNo ratings yet
- Adjuvant Local Anestesi PNBDocument23 pagesAdjuvant Local Anestesi PNBBangkit PrimayudhaNo ratings yet
- Drug Name Mechanism of Action Indication Contraindication Advers Effects Nursing Responsibilities Generic Name: SkinDocument1 pageDrug Name Mechanism of Action Indication Contraindication Advers Effects Nursing Responsibilities Generic Name: SkinsalwaNo ratings yet
- 04telkom OkDocument248 pages04telkom OksilvaniNo ratings yet