You might also like
- Drug Metabolism: Presenter:-Dr Swaroop H S Moderator: - DR Ananya ChakrabortyDocument38 pagesDrug Metabolism: Presenter:-Dr Swaroop H S Moderator: - DR Ananya Chakrabortyadinda keanayaNo ratings yet
- Xenobiotic Metabolism PDFDocument50 pagesXenobiotic Metabolism PDFroxy8marie8chanNo ratings yet
- Unit-2 BPDocument80 pagesUnit-2 BPsrinusmart192No ratings yet
- XENOBi OTIKDocument70 pagesXENOBi OTIKLie FelixNo ratings yet
- 1113453047_10073683Document34 pages1113453047_10073683arquam464No ratings yet
- The liver's role in drug metabolismDocument45 pagesThe liver's role in drug metabolismkittyNo ratings yet
- Metabolic Changes of DrugsDocument103 pagesMetabolic Changes of DrugsDaniel Wang100% (2)
- B.pharm. Class NotesDocument817 pagesB.pharm. Class NotesMukesh TiwariNo ratings yet
- Metabolism of Xenobiotics: Cytochrome P450Document70 pagesMetabolism of Xenobiotics: Cytochrome P450hartomas bumiharjoNo ratings yet
- Xenobiotics Metabolism and Cytochrome P450 EnzymesDocument4 pagesXenobiotics Metabolism and Cytochrome P450 EnzymesAsad IslamNo ratings yet
- Kuliah Farmakokinetik Metabolisme Obat 10 Mei 2010Document78 pagesKuliah Farmakokinetik Metabolisme Obat 10 Mei 2010SALSABILA RAHMA REFFANANANo ratings yet
- MedchemIII PHSC5100 2018 .PostDocument43 pagesMedchemIII PHSC5100 2018 .PostMamta ShindeNo ratings yet
- Biotrnsformation of Xenobiotics-I: Mumtaz Iscan, PH.D., ERT Professor of ToxicologyDocument61 pagesBiotrnsformation of Xenobiotics-I: Mumtaz Iscan, PH.D., ERT Professor of ToxicologyAmirabbas SaffariNo ratings yet
- Drug MetabolismDocument47 pagesDrug MetabolismDaniel WangNo ratings yet
- Drug Metabolism: Phase I and Phase II Metabolism: Principal Organs For BiotransformationDocument9 pagesDrug Metabolism: Phase I and Phase II Metabolism: Principal Organs For Biotransformationdavid5king-3119No ratings yet
- Drug Metabolism: Medicinal Chemistry IDocument34 pagesDrug Metabolism: Medicinal Chemistry IMustafa RihanNo ratings yet
- Metabolism of XenobioticsDocument54 pagesMetabolism of XenobioticsAurellia ShafitriNo ratings yet
- Hepatic Elimination: PharmacokineticsDocument34 pagesHepatic Elimination: PharmacokineticsdavarionNo ratings yet
- Drug MetabolismDocument43 pagesDrug MetabolismKelly PatrickNo ratings yet
- Drug InteractionsDocument43 pagesDrug Interactionstry_dinaa100% (1)
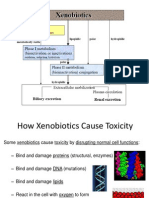
- Xenobiotics Cause Toxicity by Disrupting Cell FunctionsDocument75 pagesXenobiotics Cause Toxicity by Disrupting Cell Functionskritimahajan1989No ratings yet
- Drug Metabolism: S.P. Markey Laboratory of Neurotoxicology Nimh, NihDocument47 pagesDrug Metabolism: S.P. Markey Laboratory of Neurotoxicology Nimh, NihJanette G. RagusNo ratings yet
- Biotransformasi: Fase I, Fase II, Enzim Terlibat, Sitokrom P450, dan Faktor GenetikDocument38 pagesBiotransformasi: Fase I, Fase II, Enzim Terlibat, Sitokrom P450, dan Faktor GenetikTheresia VirginiaNo ratings yet
- Topic 21 Drug MetabolismDocument23 pagesTopic 21 Drug MetabolismjoseNo ratings yet
- Bioch CL 6. Investigarea Biochimica A Metabolismului Proteic 2020-21 (E)Document48 pagesBioch CL 6. Investigarea Biochimica A Metabolismului Proteic 2020-21 (E)Andrea ModestieNo ratings yet
- Phase I II MetabolismDocument21 pagesPhase I II MetabolismIlva Kristiāna LangrateNo ratings yet
- Cytochrome P450 Enzymes: An OverviewDocument20 pagesCytochrome P450 Enzymes: An OverviewAnitha Mary DambaleNo ratings yet
- Metabolism of XenobioticsDocument30 pagesMetabolism of XenobioticsCzarina RiveraNo ratings yet
- Metabolism of Xenobiotics: A Three Phase ProcessDocument84 pagesMetabolism of Xenobiotics: A Three Phase ProcessJNo ratings yet
- Drug Affecting Metabolism by RinkuDocument23 pagesDrug Affecting Metabolism by RinkuRinku KunduNo ratings yet
- Protein Metabolism and Acids SamyA1Document170 pagesProtein Metabolism and Acids SamyA1Abby RahmanNo ratings yet
- Lecture 2 Drug Metabolism Phase IIDocument27 pagesLecture 2 Drug Metabolism Phase IIfeegame7No ratings yet
- Biochemical Response to XenobioticsDocument52 pagesBiochemical Response to XenobioticsTiaRa JuraidNo ratings yet
- Clinical Pharmacokinetics (Biotransformation)Document49 pagesClinical Pharmacokinetics (Biotransformation)kamalNo ratings yet
- Drug Metabolism - Chapter 8Document44 pagesDrug Metabolism - Chapter 8Shaun李好No ratings yet
- Xenobiotic FKBiotransformationDocument100 pagesXenobiotic FKBiotransformationMuhammad SyaifullahNo ratings yet
- Biotransformation of XenobioticsDocument64 pagesBiotransformation of XenobioticsChristian DanielNo ratings yet
- UNIT 2 ELIMINATION and BIOAVAILABILITY & BIOEQUIVALENCE PDFDocument207 pagesUNIT 2 ELIMINATION and BIOAVAILABILITY & BIOEQUIVALENCE PDFMamta Pant100% (4)
- Metabolism 2017Document96 pagesMetabolism 2017aimaNo ratings yet
- Drug Elimination: Termination of Drug ActionDocument69 pagesDrug Elimination: Termination of Drug ActionDinar RestitiNo ratings yet
- Organic Medicinals: Jelly Mae T. Oviedo, RPHDocument69 pagesOrganic Medicinals: Jelly Mae T. Oviedo, RPHNica ChuaNo ratings yet
- Pharmaceutical Medicinal Organic Chemistry: International School of Asia and The Pacific - KalingaDocument3 pagesPharmaceutical Medicinal Organic Chemistry: International School of Asia and The Pacific - KalingaJunimy GamonganNo ratings yet
- Major Metabolic PathwaysDocument23 pagesMajor Metabolic PathwaysgianelleNo ratings yet
- BIOTRANSFORMATIONDocument42 pagesBIOTRANSFORMATIONMubassir NisarNo ratings yet
- 07 Amino Acid MetabolismDocument108 pages07 Amino Acid MetabolismMuhammad Awais NoorNo ratings yet
- Metabolism of XenobioticsDocument5 pagesMetabolism of XenobioticsJanelle Bondad100% (2)
- Running Head: Biochemistry Assignment 1Document6 pagesRunning Head: Biochemistry Assignment 1Fredrick LiyengaNo ratings yet
- Drug Metabolism and Excretion: An OverviewDocument19 pagesDrug Metabolism and Excretion: An OverviewAsadullah ghalibNo ratings yet
- MetabolismDocument15 pagesMetabolismnadila oktaviaNo ratings yet
- BiotransformationDocument27 pagesBiotransformationDemy ClementeNo ratings yet
- 19 BiochemistryDocument14 pages19 BiochemistryMuhammad Amin BozdarNo ratings yet
- Lecture 4 Metabolism Phase Iv 2Document49 pagesLecture 4 Metabolism Phase Iv 2Umar AzadNo ratings yet
- BIOCHEMICAL PATHWAYSDocument38 pagesBIOCHEMICAL PATHWAYSMarja Shania Galido RañolaNo ratings yet
- Clinical Biochemistry in Toxicology-PGDocument16 pagesClinical Biochemistry in Toxicology-PGaswani69No ratings yet
- 15 GMppt-chapter18-2020 (Ok)Document19 pages15 GMppt-chapter18-2020 (Ok)Kw ChanNo ratings yet
- Drug Metabolism OKDocument34 pagesDrug Metabolism OKSaifuddin AzizNo ratings yet
- 3study Questions-Drug MetabolismDocument5 pages3study Questions-Drug Metabolismapi-3723612No ratings yet
- Biology Unit 4 Part 1 Last Minute Revision ReallyacademicsDocument67 pagesBiology Unit 4 Part 1 Last Minute Revision ReallyacademicsWill AndyNo ratings yet
- Inmuno 555Document11 pagesInmuno 555Daniela Fdz CNo ratings yet
- Summer Training BrochureDocument1 pageSummer Training BrochureAbhilashRayaguruNo ratings yet
- The main functions and structure of centrioles in cell divisionDocument2 pagesThe main functions and structure of centrioles in cell divisiontherese lamelaNo ratings yet
- Scope of BiochemistryDocument3 pagesScope of BiochemistryQurrotul A'yun80% (5)
- DNA Scissors Cut DNADocument2 pagesDNA Scissors Cut DNAOktira Roka AjiNo ratings yet
- Chemical BiologyDocument14 pagesChemical BiologyVaibhav MardeNo ratings yet
- Paperclip Activity-Dna ReplicationDocument4 pagesPaperclip Activity-Dna Replicationapi-201291946No ratings yet
- Ch9 2 LipidomicsAnswerDocument5 pagesCh9 2 LipidomicsAnswerReginald GironNo ratings yet
- Chemical Pathology 2 - Plasma ProteinsDocument5 pagesChemical Pathology 2 - Plasma ProteinsaNo ratings yet
- Biology Review Game - Print - QuizizzDocument5 pagesBiology Review Game - Print - QuizizzrubelliteNo ratings yet
- Biological TreatmentDocument25 pagesBiological TreatmentMohammad Khairizal AfendyNo ratings yet
- Anti-Neoplastic Agents 1Document76 pagesAnti-Neoplastic Agents 1Soubia AamirNo ratings yet
- HARPERS - IV Carbohydrates of Physiological SignificanceDocument4 pagesHARPERS - IV Carbohydrates of Physiological SignificancedandiNo ratings yet
- Bio150 Chapter 3 - Part 3Document7 pagesBio150 Chapter 3 - Part 3Adibah Qistina QistinaNo ratings yet
- Monogastric Digestive SystemDocument25 pagesMonogastric Digestive SystemMae Sntg OraNo ratings yet
- Cell Growth Lab Report Final DraftDocument10 pagesCell Growth Lab Report Final DraftKeithen CastNo ratings yet
- VIASURE Flu A, Flu B & RSV Real Time PCR Detection Kit BD REF 444201Document20 pagesVIASURE Flu A, Flu B & RSV Real Time PCR Detection Kit BD REF 444201faridNo ratings yet
- BR574 0915 xMAP Cookbook 3rdedition WR PDFDocument148 pagesBR574 0915 xMAP Cookbook 3rdedition WR PDFNiranjan BhuvanaratnamNo ratings yet
- Experimental Biochemistry PDFDocument2 pagesExperimental Biochemistry PDFJune100% (1)
- Open Source Proteomics SoftwareDocument49 pagesOpen Source Proteomics Softwareken tsaiNo ratings yet
- Urea Cycle and Protein MetabolismDocument39 pagesUrea Cycle and Protein Metabolismikramullahkhan211No ratings yet
- MMLV - RT - Man Invtro ReverseDocument4 pagesMMLV - RT - Man Invtro ReverseJorge Hernandez LopezNo ratings yet
- Prelim Oral ExamDocument3 pagesPrelim Oral ExamJP2001No ratings yet
- Biology NotesDocument16 pagesBiology NotesSarah Jane O Farrell100% (1)
- BT503 Environment Biotechnology (Merget PPT Handouts (1 To 235) Full Mid and Final)Document139 pagesBT503 Environment Biotechnology (Merget PPT Handouts (1 To 235) Full Mid and Final)laibaNo ratings yet
- Enzyme Kinetics: Understanding Reaction RatesDocument12 pagesEnzyme Kinetics: Understanding Reaction RatesNadia NovitaNo ratings yet
- Transverse Urea-Gradient Gel Electrophoresis UNIT 7.4 BASIC PROTOCOLDocument13 pagesTransverse Urea-Gradient Gel Electrophoresis UNIT 7.4 BASIC PROTOCOLNancy Marianna Muñoz ValeraNo ratings yet
- Summary Notes - Topic 7 Respiration, Muscles and The Internal Environment - Edexcel (IAL) Biology A-LevelDocument11 pagesSummary Notes - Topic 7 Respiration, Muscles and The Internal Environment - Edexcel (IAL) Biology A-LevelYashodya WimalagunasekaraNo ratings yet
- How Does Penicillin WorkDocument6 pagesHow Does Penicillin WorkJanista FrankNo ratings yet