You might also like
- Predictors of Chronic Ankle InstabilityDocument6 pagesPredictors of Chronic Ankle InstabilityLeydi LondoñoNo ratings yet
- Sports Hernia and Athletic Pubalgia: Diagnosis and TreatmentFrom EverandSports Hernia and Athletic Pubalgia: Diagnosis and TreatmentDavid R. DiduchNo ratings yet
- Ijspt 08 121 PDFDocument8 pagesIjspt 08 121 PDFRamadhan Wahyu PuteraNo ratings yet
- Difference in Balance Measures Between Patients With Chronic Ankle Instability and Patients After An Acute Ankle Inversion TraumaDocument17 pagesDifference in Balance Measures Between Patients With Chronic Ankle Instability and Patients After An Acute Ankle Inversion TraumaAbu MishalNo ratings yet
- Newton2006 PDFDocument7 pagesNewton2006 PDFAlexandre FerreiraNo ratings yet
- Whatman (2011) Kinematics During Lower Extremity Functional Screening Tests - Are They Reliable and Related To JoggingDocument8 pagesWhatman (2011) Kinematics During Lower Extremity Functional Screening Tests - Are They Reliable and Related To Jogginglinoco1No ratings yet
- Balance-And Strength-Training Protocols To Improve Chronic Ankle Instability Deficits, Part I: Assessing Clinical Outcome MeasuresDocument10 pagesBalance-And Strength-Training Protocols To Improve Chronic Ankle Instability Deficits, Part I: Assessing Clinical Outcome MeasuresGorkaBuesaNo ratings yet
- Validacion Del Plank Lateral Comopo Test de Muscle EndurenceDocument13 pagesValidacion Del Plank Lateral Comopo Test de Muscle EndurenceDaniel WollNo ratings yet
- Paper MAI FootDocument10 pagesPaper MAI Foothareem7bilalNo ratings yet
- Communications,: Free Oral Presentations: Ankle ProphylacticsDocument2 pagesCommunications,: Free Oral Presentations: Ankle ProphylacticsRobinson CrusoNo ratings yet
- A Novel Single-Leg Squat Test With Speed and Accuracy Requirements Reliability and Validity in Anterior Cruciate Ligament Reconstructed IndividualsDocument10 pagesA Novel Single-Leg Squat Test With Speed and Accuracy Requirements Reliability and Validity in Anterior Cruciate Ligament Reconstructed IndividualsAriene RibeiroNo ratings yet
- Differences in Landing and Balance Deficits at The Ankle Joint On Stable and Unstable Surfaces in Inflexible and Flexible Handball PlayersDocument8 pagesDifferences in Landing and Balance Deficits at The Ankle Joint On Stable and Unstable Surfaces in Inflexible and Flexible Handball PlayersAJHSSR JournalNo ratings yet
- Impellizzeri MSSE Asimmetry 1 PDFDocument7 pagesImpellizzeri MSSE Asimmetry 1 PDFMax ArellanoNo ratings yet
- Active Knee Extension Test Excellent Reliability PDFDocument5 pagesActive Knee Extension Test Excellent Reliability PDFSahithya MNo ratings yet
- Refencia de Lanzamiento 3Document4 pagesRefencia de Lanzamiento 3ArnadisTNo ratings yet
- Relationships Between Functional Movement Tests and Performance Tests in Young Elite Male Basketball Players PDFDocument11 pagesRelationships Between Functional Movement Tests and Performance Tests in Young Elite Male Basketball Players PDFOriol Ruiz PujolNo ratings yet
- JSSM 09 431Document8 pagesJSSM 09 431Tadija TrajkovićNo ratings yet
- Jpts 26 629Document3 pagesJpts 26 629Evelin HanaNo ratings yet
- Lower Extremity Muscle Activation During Functional Exercises in Patients With and Without Chronic Ankle InstabilityDocument10 pagesLower Extremity Muscle Activation During Functional Exercises in Patients With and Without Chronic Ankle InstabilityDavid SugiartoNo ratings yet
- J Gaitpost 2012 03 008Document5 pagesJ Gaitpost 2012 03 008sina dabiriNo ratings yet
- Hes Sari 2012Document6 pagesHes Sari 2012bbvnrsh279No ratings yet
- Changes in Postural Stability With Fatigue of Lower Extremity Frontal and Sagittal Plane MoversDocument5 pagesChanges in Postural Stability With Fatigue of Lower Extremity Frontal and Sagittal Plane MoversKhaled AbuzayanNo ratings yet
- Fraser 2020Document11 pagesFraser 2020Najla IrbahNo ratings yet
- Relationship Between Subtalar Joint Stiffness andDocument10 pagesRelationship Between Subtalar Joint Stiffness andrishi rajgudeNo ratings yet
- Alterations in Mechanical Properties of The Patellar Tendon Is Associated With Pain in Athletes With Patellar TendinopathyDocument7 pagesAlterations in Mechanical Properties of The Patellar Tendon Is Associated With Pain in Athletes With Patellar TendinopathyIsrael Oña CisnerosNo ratings yet
- AbstractDocument99 pagesAbstracthakishankzNo ratings yet
- Amp Rhab6Document7 pagesAmp Rhab6Ale XaNo ratings yet
- 05meshkati JSR 20090094 CeDocument15 pages05meshkati JSR 20090094 Cericcardo6grassiNo ratings yet
- A Single-Blind, Cross-Over Trial of Hip Abductor Strength Training To Improve Timed Up Go Performance in Patients With Unilateral, Transfemoral AmputationDocument7 pagesA Single-Blind, Cross-Over Trial of Hip Abductor Strength Training To Improve Timed Up Go Performance in Patients With Unilateral, Transfemoral AmputationJhony GonzalezNo ratings yet
- Wil Ken 2012Document6 pagesWil Ken 2012Putu Reza Sandhya PratamaNo ratings yet
- Reliability of BiodexDocument13 pagesReliability of BiodexMattNo ratings yet
- Which Trunk Inclination Directions Best Predict Multidirectional-Seated Limits of Stability Among Individuals With Spinal Cord Injury?Document8 pagesWhich Trunk Inclination Directions Best Predict Multidirectional-Seated Limits of Stability Among Individuals With Spinal Cord Injury?Chanapass DenduangNo ratings yet
- JoelhoDocument7 pagesJoelhoÉrica SilvaNo ratings yet
- Simplifying The SEBT Analyses of Subjects With and Without Chronic Ankle InstabilityDocument7 pagesSimplifying The SEBT Analyses of Subjects With and Without Chronic Ankle InstabilityFebryLasantiNo ratings yet
- Musculoskeletal Screening To Detect Asymmetry in SwimmingDocument6 pagesMusculoskeletal Screening To Detect Asymmetry in SwimmingYoh ChenNo ratings yet
- Differences in Postural Control During Single-Leg Stance Among Healthy Individuals With Different Foot TypesDocument4 pagesDifferences in Postural Control During Single-Leg Stance Among Healthy Individuals With Different Foot TypesTadija TrajkovićNo ratings yet
- Postural Ability Reflects The Athletic Skill Level of SurfersDocument5 pagesPostural Ability Reflects The Athletic Skill Level of SurfersCharles MitchellNo ratings yet
- Intra-Rater Reliability of The Multiple Single-Leg Hop-Stabilization Test and Relationships With Age, Leg Dominance and TrainingDocument9 pagesIntra-Rater Reliability of The Multiple Single-Leg Hop-Stabilization Test and Relationships With Age, Leg Dominance and TrainingSamuelNo ratings yet
- November1995 RS GreenbergerDocument5 pagesNovember1995 RS GreenbergerEnsar AbazovicNo ratings yet
- Effect of Foot Strengthening Exercises in Osteoarthritis KneeDocument5 pagesEffect of Foot Strengthening Exercises in Osteoarthritis KneefiaNo ratings yet
- Captura de Tela 2023-09-09 À(s) 06.38.44Document7 pagesCaptura de Tela 2023-09-09 À(s) 06.38.44jotta de lima BragaNo ratings yet
- Relationship Between Ankle Range of Motion and Biodex Balance System in Females and MalesDocument5 pagesRelationship Between Ankle Range of Motion and Biodex Balance System in Females and MalesLisnaWatiNo ratings yet
- Impact-Related Ground Reaction Forces Are More Strongly Associated With Some Running Injuries Than OthersDocument9 pagesImpact-Related Ground Reaction Forces Are More Strongly Associated With Some Running Injuries Than OthersAriene RibeiroNo ratings yet
- The Relationship Between The Fms and Modified Beep Test Scores in Underwater Rugby PlayersDocument5 pagesThe Relationship Between The Fms and Modified Beep Test Scores in Underwater Rugby PlayersWong ,BryanNo ratings yet
- Indicators of Throwing Arm Fatigue in Elite.5Document6 pagesIndicators of Throwing Arm Fatigue in Elite.5Jayne PereiraNo ratings yet
- Kinetics, Kinematics, and Knee Muscle Activation During Sit To Stand Transition in Unilateral and Bilateral Knee OsteoarthritisDocument7 pagesKinetics, Kinematics, and Knee Muscle Activation During Sit To Stand Transition in Unilateral and Bilateral Knee OsteoarthritisSiriratNo ratings yet
- A Comparison of Outcomes in Osteoarthritis Patients Undergoing Total Hip and Knee Replacement SurgeryDocument10 pagesA Comparison of Outcomes in Osteoarthritis Patients Undergoing Total Hip and Knee Replacement SurgeryRini MaghfirahNo ratings yet
- Hielcontact Bij PfpsDocument6 pagesHielcontact Bij PfpsEllen&Koen WalravensNo ratings yet
- Bohannon2010 Performance PDFDocument6 pagesBohannon2010 Performance PDFmariasol63No ratings yet
- Foot and Ankle Surgery: Byung-Ki Cho, Ji-Kang Park, Seung-Myung Choi, Sang-Woo Kang, Nelson F. SoohooDocument6 pagesFoot and Ankle Surgery: Byung-Ki Cho, Ji-Kang Park, Seung-Myung Choi, Sang-Woo Kang, Nelson F. SoohooAry RitmmaNo ratings yet
- 2021 Influence of Invertor and Evertor Muscle Fatigue On Functional Jump Tests andDocument4 pages2021 Influence of Invertor and Evertor Muscle Fatigue On Functional Jump Tests andktan.lboroNo ratings yet
- Effect of Lower Extremity Muscular Fatigue On Motor Control PerformanceDocument21 pagesEffect of Lower Extremity Muscular Fatigue On Motor Control PerformancePabloT81No ratings yet
- Sumber Fisis FisioterapiDocument9 pagesSumber Fisis FisioterapiAndi detty UtamiNo ratings yet
- Ha2018 PDFDocument5 pagesHa2018 PDFHusnannisa ArifNo ratings yet
- Physical Therapy in Sport: Suzi Edwards, Hiram C. Brooke, Jill L. CookDocument9 pagesPhysical Therapy in Sport: Suzi Edwards, Hiram C. Brooke, Jill L. CookLing Pong HungNo ratings yet
- Ground and In-Shoe Reaction Forces During WalkingDocument1 pageGround and In-Shoe Reaction Forces During WalkingCesar EspinosaNo ratings yet
- International Society For Technology in Arthroplasty - Indicação de ArtigosDocument77 pagesInternational Society For Technology in Arthroplasty - Indicação de ArtigosJosé santanaNo ratings yet
- Características Radiográficas, Artroscópicas y Biomecánicas de Perros Con Ruptura Del Ligamento Cruzado AnteriorDocument6 pagesCaracterísticas Radiográficas, Artroscópicas y Biomecánicas de Perros Con Ruptura Del Ligamento Cruzado AnteriorPaola Serrano DazaNo ratings yet
- Ffect of Plyometric Versus Ankle Stability ExercisesDocument10 pagesFfect of Plyometric Versus Ankle Stability ExercisesMoin RashidNo ratings yet
- PGS 504 Notes Part IIDocument3 pagesPGS 504 Notes Part IISejal PriyaNo ratings yet
- Material Data Sheet Durapro Asa: DescriptionDocument1 pageMaterial Data Sheet Durapro Asa: DescriptionAlexandru NeacsuNo ratings yet
- 2018 Wassce Integrated Science 1Document6 pages2018 Wassce Integrated Science 1Theophilus Asante-TannorNo ratings yet
- Manufacturing ProcessesDocument6 pagesManufacturing ProcessesSudalai MadanNo ratings yet
- Med Mantra Hospital Management Solution 0813 1Document4 pagesMed Mantra Hospital Management Solution 0813 1vvr_9No ratings yet
- Access To JusticeDocument9 pagesAccess To JusticeprimeNo ratings yet
- Hitec 8888Z Atf C4 & To4 - TDSDocument2 pagesHitec 8888Z Atf C4 & To4 - TDSPranit More Arabian Petroleum LimitedNo ratings yet
- Antiemetics - AMBOSSDocument4 pagesAntiemetics - AMBOSSOpio IsaacNo ratings yet
- First Quarter Examination For AP 10Document4 pagesFirst Quarter Examination For AP 10Reynan Orillos HorohoroNo ratings yet
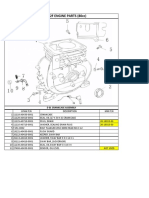
- Lifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblyDocument13 pagesLifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblySean MurrayNo ratings yet
- Finalllllll BPDocument46 pagesFinalllllll BPSheypia Agustin JacintoNo ratings yet
- PERDEV FIRST Periodical Test (2022)Document5 pagesPERDEV FIRST Periodical Test (2022)jeadryl LinatocNo ratings yet
- E 23 Fuel System Schaffer 4350ZDocument3 pagesE 23 Fuel System Schaffer 4350ZSergeyNo ratings yet
- Climate Responsive ArchitectureDocument32 pagesClimate Responsive ArchitectureNikhila CherughattuNo ratings yet
- Cognizin CDPCholine Caps 60vcaps by Life ExtensionnvyzqvhqimDocument2 pagesCognizin CDPCholine Caps 60vcaps by Life Extensionnvyzqvhqimcarollip2No ratings yet
- Excellent Achievers Learning, Center, IncDocument5 pagesExcellent Achievers Learning, Center, IncJoyR.Alota100% (1)
- Ccii Proposal EssayDocument4 pagesCcii Proposal Essayapi-456307983No ratings yet
- Offshore Drilling Operation in East Indonesia Oil and Gas FieldsDocument3 pagesOffshore Drilling Operation in East Indonesia Oil and Gas FieldsMuhammad Galih Eko SaputroNo ratings yet
- MMFSLDocument9 pagesMMFSLsachin11hahaNo ratings yet
- PFI Freediver ManualDocument69 pagesPFI Freediver ManualLuca MariniNo ratings yet
- To: Head of Sea Training Department PT Gemilang Bina Lintas Tirta Ship ManagementDocument1 pageTo: Head of Sea Training Department PT Gemilang Bina Lintas Tirta Ship ManagementtarNo ratings yet
- DS 1 CatDocument38 pagesDS 1 CatMuhammad Bilal Khattak100% (1)
- Ark of The Covenant Montessori Chamber of Learning PoblacionDocument3 pagesArk of The Covenant Montessori Chamber of Learning PoblacionMaiAce Sean Shawn SynneNo ratings yet
- Up & Up LyricDocument2 pagesUp & Up LyricMuhammad Ali MahdiNo ratings yet
- ADPKDDocument75 pagesADPKDVenkataramanan KrishnamoorthyNo ratings yet
- Annual Report (2013) Combined With Site Visit Report of Lok Biradari PrakalpDocument9 pagesAnnual Report (2013) Combined With Site Visit Report of Lok Biradari PrakalpAsha ZurichNo ratings yet
- Personal and Social AdjustmentDocument10 pagesPersonal and Social AdjustmentMobin AlamNo ratings yet
- Separation of Plant Pigments PDFDocument3 pagesSeparation of Plant Pigments PDFneelNo ratings yet
- Bio 2Document3 pagesBio 2ganchimeg gankhuuNo ratings yet
- Jeremiah's Law, Introduced by Assemblywoman Rodneyse BichotteDocument2 pagesJeremiah's Law, Introduced by Assemblywoman Rodneyse BichotteCity & State NYNo ratings yet