You might also like
- CDC MMRV Vaccine Data Safety Link SlidesDocument14 pagesCDC MMRV Vaccine Data Safety Link SlidesVaccineInformation100% (6)
- Febrile Seizure Risk After Vaccination in Children 6 To 23 MonthsDocument12 pagesFebrile Seizure Risk After Vaccination in Children 6 To 23 MonthsrfNo ratings yet
- J.22-09-2011 VaricellaDocument3 pagesJ.22-09-2011 VaricellaIndra PolenkNo ratings yet
- Feverinthepediatricpatient: Robyn Wing,, Maya R. Dor,, Patricia A. McquilkinDocument24 pagesFeverinthepediatricpatient: Robyn Wing,, Maya R. Dor,, Patricia A. McquilkinSebastian SalinasNo ratings yet
- CDC 57181 DS1Document17 pagesCDC 57181 DS1She KNo ratings yet
- CDC MMR, MMR+V, MMRV Seizure RatesDocument4 pagesCDC MMR, MMR+V, MMRV Seizure RatesVaccineInformation83% (6)
- Pediatrics 2012 Klein 809 14Document8 pagesPediatrics 2012 Klein 809 14Myrtle SetiawanNo ratings yet
- Feverinthepediatricpatient: Robyn Wing,, Maya R. Dor,, Patricia A. McquilkinDocument24 pagesFeverinthepediatricpatient: Robyn Wing,, Maya R. Dor,, Patricia A. McquilkinAzkiaNo ratings yet
- Human Vaccines & Immunotherapeutics: News: Two Studies On Optimal Timing For Measles VaccinationDocument4 pagesHuman Vaccines & Immunotherapeutics: News: Two Studies On Optimal Timing For Measles VaccinationTri RachmadijantoNo ratings yet
- Fast-Tracked Swine Flu Vaccine Under FireDocument4 pagesFast-Tracked Swine Flu Vaccine Under FireaparnasingNo ratings yet
- Fever in The Pediatric Patient PDFDocument24 pagesFever in The Pediatric Patient PDFSABASA1012No ratings yet
- Accepted ManuscriptDocument19 pagesAccepted Manuscripthilman lesmanaNo ratings yet
- Evaluacion Niño Con FiebreDocument24 pagesEvaluacion Niño Con FiebredanielentuxtlaNo ratings yet
- 2 Review Diphtheria Results April2017 Final Clean PDFDocument20 pages2 Review Diphtheria Results April2017 Final Clean PDFchameleonNo ratings yet
- An Observational Study of Febrile Seizures: The Importance of Viral Infection and ImmunizationDocument6 pagesAn Observational Study of Febrile Seizures: The Importance of Viral Infection and Immunizationnavali rahmaNo ratings yet
- Varicella Post-ProphylaxisDocument2 pagesVaricella Post-ProphylaxisAngelaTrinidadNo ratings yet
- Jurnal 1Document9 pagesJurnal 1Riyan TrequartistaNo ratings yet
- Influenza EditorialDocument3 pagesInfluenza EditorialcasteltenNo ratings yet
- VaccinestudiesDocument21 pagesVaccinestudiesapi-277588360No ratings yet
- Risk of Seizures After Immunization in Children With Epilepsy: A Risk Interval AnalysisDocument7 pagesRisk of Seizures After Immunization in Children With Epilepsy: A Risk Interval AnalysisReziNo ratings yet
- Vaksin VarelaDocument8 pagesVaksin VarelaPutra EkaNo ratings yet
- Schaefer 2017Document6 pagesSchaefer 2017hasemana hasemanaNo ratings yet
- (R) Varicella VirusDocument8 pages(R) Varicella VirusEkkim Al KindiNo ratings yet
- GADARDocument13 pagesGADARsarbia7799No ratings yet
- Fiebre Sin Foco 0-36 MesesDocument28 pagesFiebre Sin Foco 0-36 MesesdanielentuxtlaNo ratings yet
- Immune Responses To Measles and Mumps Vaccination of Infants at 6, 9, and 12 MonthsDocument10 pagesImmune Responses To Measles and Mumps Vaccination of Infants at 6, 9, and 12 MonthsManiru Aliyu GiganeNo ratings yet
- Atagi Recommendations On Pfizer Covid 19 Vaccine Use in Children Aged 5 To 11 YearsDocument11 pagesAtagi Recommendations On Pfizer Covid 19 Vaccine Use in Children Aged 5 To 11 YearsGanesh SahathevanNo ratings yet
- Postvaccination Febrile Seizure Severity and OutcomeDocument11 pagesPostvaccination Febrile Seizure Severity and OutcomeGrace Malinda LimopranotoNo ratings yet
- Actualidades en InfectologíaDocument47 pagesActualidades en InfectologíaDamián López RangelNo ratings yet
- Febrile Seizures: Risks, Evaluation, and PrognosisDocument6 pagesFebrile Seizures: Risks, Evaluation, and PrognosisMaudonlodNo ratings yet
- First Line FluDocument6 pagesFirst Line Flu419022 MELA ANANDA PUTRIANANo ratings yet
- Research Paper On Childhood VaccinationsDocument8 pagesResearch Paper On Childhood Vaccinationsefjr9yx3100% (1)
- Pediatrics 2010 Klein E1 8Document10 pagesPediatrics 2010 Klein E1 8MeidikaWulandariNo ratings yet
- Acellular Pertussis Vaccine Effectiveness Over Time: ObjectivesDocument11 pagesAcellular Pertussis Vaccine Effectiveness Over Time: Objectives[JC]No ratings yet
- The Safety of Influenza Vaccines in Children An Institute For Vaccine Safety White PaperDocument67 pagesThe Safety of Influenza Vaccines in Children An Institute For Vaccine Safety White Papermaheshmuralinair6No ratings yet
- Measles-Mumps-Rubella-Varicella CombinationDocument11 pagesMeasles-Mumps-Rubella-Varicella CombinationSiluet SenjaNo ratings yet
- MainDocument4 pagesMainarini ayukNo ratings yet
- Protecting Infants From Pertussis: Child Health UpdateDocument3 pagesProtecting Infants From Pertussis: Child Health UpdateFadjrin Muhammad BazliNo ratings yet
- Nejm VaricellaDocument9 pagesNejm VaricellaadityailhamNo ratings yet
- Jurnal 1Document6 pagesJurnal 1Rey M FakhruryNo ratings yet
- Research Paper On Childhood VaccinesDocument7 pagesResearch Paper On Childhood Vaccinesafnkjdhxlewftq100% (1)
- Prevention and Treatment of Seasonal Influenza: Clinical PracticeDocument7 pagesPrevention and Treatment of Seasonal Influenza: Clinical PracticeDias PradikaNo ratings yet
- Evaluation of Combination Measles-Mumps-Rubella-Varicella Vaccine Introduction in AustraliaDocument7 pagesEvaluation of Combination Measles-Mumps-Rubella-Varicella Vaccine Introduction in AustraliazainabNo ratings yet
- Running Head: Immunization Case-StudyDocument6 pagesRunning Head: Immunization Case-StudyOLEMGBE GODSWILLNo ratings yet
- Acellular Pertussis Vaccine Effectiveness Over Time: ObjectivesDocument11 pagesAcellular Pertussis Vaccine Effectiveness Over Time: ObjectivesLee제노No ratings yet
- Journal 1Document8 pagesJournal 1DICKY DEWANTORONo ratings yet
- Estimation of Vaccine Efficacy and Critical Vaccination Coverage in Partially Observed OutbreaksDocument9 pagesEstimation of Vaccine Efficacy and Critical Vaccination Coverage in Partially Observed OutbreaksAri SiswadiNo ratings yet
- Measles Q&A: Causes, Symptoms, VaccineDocument4 pagesMeasles Q&A: Causes, Symptoms, VaccineAustine OsaweNo ratings yet
- 2010 Fiebre Sin FocoDocument29 pages2010 Fiebre Sin FocoHerminia CastilloNo ratings yet
- WHO PP Varicella Herpes Zoster June2014 PresentationDocument29 pagesWHO PP Varicella Herpes Zoster June2014 PresentationMicki TaryanNo ratings yet
- Journal of Infectious DiseaseDocument6 pagesJournal of Infectious DiseaseSoham SarangiNo ratings yet
- Selected References: Mumps Vaccines Studies On Immune Responses, Efficacy and EffectivenessDocument11 pagesSelected References: Mumps Vaccines Studies On Immune Responses, Efficacy and EffectivenessekowahyudiNo ratings yet
- Fiebre Sin Foco Aparente 3 A 36 Meses DynaMedDocument41 pagesFiebre Sin Foco Aparente 3 A 36 Meses DynaMedAna Maria Guerron CabreraNo ratings yet
- Piyasirisilp 2002Document6 pagesPiyasirisilp 2002Vedith KumarNo ratings yet
- Annotated BibliographyDocument19 pagesAnnotated Bibliographyapi-455648185No ratings yet
- Research Paper On Child VaccinationsDocument7 pagesResearch Paper On Child Vaccinationspwvgqccnd100% (1)
- Genetics and The Evaluation of The Febrile Child: EditorialDocument2 pagesGenetics and The Evaluation of The Febrile Child: EditorialYRRVNo ratings yet
- Epilepsia - 2011 - Cendes - Vaccinations and Febrile SeizuresDocument3 pagesEpilepsia - 2011 - Cendes - Vaccinations and Febrile SeizurespuhumightNo ratings yet
- Vaccines: Making the Right Choice for Your ChildFrom EverandVaccines: Making the Right Choice for Your ChildRating: 5 out of 5 stars5/5 (2)
- Pediatric Immunology: A Case-Based Collection with MCQs, Volume 2From EverandPediatric Immunology: A Case-Based Collection with MCQs, Volume 2No ratings yet
- EngDocument48 pagesEngnina nurhayatiNo ratings yet
- Analysis of Forest Area Determination CriteriaDocument14 pagesAnalysis of Forest Area Determination CriteriaHarunHasibNo ratings yet
- Pi Is 0091674906013704Document2 pagesPi Is 0091674906013704Eddie WyattNo ratings yet
- 2019 Clinical Guidelines SummaryDocument2 pages2019 Clinical Guidelines SummaryEddie WyattNo ratings yet
- Pi Is 0091674906013704Document2 pagesPi Is 0091674906013704Eddie WyattNo ratings yet
- 59 15-68Document7 pages59 15-68Eddie WyattNo ratings yet
- Baca Sebelum Instal GameDocument1 pageBaca Sebelum Instal GameEddie WyattNo ratings yet
- Guidline TetanusDocument363 pagesGuidline TetanusferianaNo ratings yet
- Jurnal Terapi FaringitisDocument7 pagesJurnal Terapi Faringitisarstantyar0% (1)
- Kumpulan Osce Ukmppd - BimaDocument2 pagesKumpulan Osce Ukmppd - BimaEddie Wyatt0% (1)
- Osteoporosis NOGG Guideline 2017Document36 pagesOsteoporosis NOGG Guideline 2017Claudia Micu100% (1)
- Normal-Pressure Hydrocephalus: Roger SalloumDocument2 pagesNormal-Pressure Hydrocephalus: Roger SalloumEddie WyattNo ratings yet
- Obat BaksosDocument1 pageObat BaksosEddie WyattNo ratings yet
- Baca Sebelum Instal GameDocument1 pageBaca Sebelum Instal GameEddie WyattNo ratings yet
- NILAI PRAKTIKUM BLOK RESPIRASI ANATOMI FK UNSDocument18 pagesNILAI PRAKTIKUM BLOK RESPIRASI ANATOMI FK UNSEddie WyattNo ratings yet
- OPTIMAL INFANT FEEDING PRACTICESDocument46 pagesOPTIMAL INFANT FEEDING PRACTICESEddie WyattNo ratings yet
- NILAI PRAKTIKUM BLOK RESPIRASI ANATOMI FK UNSDocument18 pagesNILAI PRAKTIKUM BLOK RESPIRASI ANATOMI FK UNSEddie WyattNo ratings yet
- Pembahasan Soal UB10 Muskulo 2010Document10 pagesPembahasan Soal UB10 Muskulo 2010Eddie WyattNo ratings yet
- JADWAL JAGA KLINIK BSMIDocument8 pagesJADWAL JAGA KLINIK BSMIEddie WyattNo ratings yet
- Obat BaksosDocument1 pageObat BaksosEddie WyattNo ratings yet
- NIlai 2016Document31 pagesNIlai 2016Eddie WyattNo ratings yet
- Peripheral Nerve DisordersDocument34 pagesPeripheral Nerve DisordersEddie WyattNo ratings yet
- Daftar PustakaDocument5 pagesDaftar PustakaEddie WyattNo ratings yet
- The Fractured Femur: Directed Readings in The ClassroomDocument68 pagesThe Fractured Femur: Directed Readings in The ClassroomEddie Wyatt100% (1)
- Jadwal Laboratorium Anatomi UNS 2017Document1 pageJadwal Laboratorium Anatomi UNS 2017Eddie WyattNo ratings yet
- DMS 2014 - B - Basic of Bone & Joint InfectionDocument28 pagesDMS 2014 - B - Basic of Bone & Joint InfectionEddie WyattNo ratings yet
- Nail Loss: Oleh: Hananto Wildan Habibi (G0014111)Document11 pagesNail Loss: Oleh: Hananto Wildan Habibi (G0014111)Eddie WyattNo ratings yet
- Zam 7116Document6 pagesZam 7116DdCasadoLasterosNo ratings yet
- Should Vaccination Be CompulsoryDocument2 pagesShould Vaccination Be CompulsoryPA ZENo ratings yet
- Peel Public Health Immunization RecordDocument2 pagesPeel Public Health Immunization RecordIA - 07VL 794236 Sunny View MSNo ratings yet
- Urn Uvci 01 Ro W10dmyl82pkjp01x7wgz6or37gev9x#kDocument2 pagesUrn Uvci 01 Ro W10dmyl82pkjp01x7wgz6or37gev9x#kLungu MirelaNo ratings yet
- AMOpportunities Certificate of ImmunizationDocument1 pageAMOpportunities Certificate of ImmunizationАида АрзуманянNo ratings yet
- Learners Vaccination Inventory S.Y 2022 2023Document22 pagesLearners Vaccination Inventory S.Y 2022 2023CELIA T. BOLASTUGNo ratings yet
- FOGSI Current Updates Vol 2Document1 pageFOGSI Current Updates Vol 2Banu NatarajanNo ratings yet
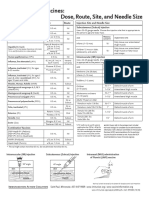
- Injection Site and Needle Size Vaccine Dose RouteDocument1 pageInjection Site and Needle Size Vaccine Dose RouteDr Ambana GowdaNo ratings yet
- Quiz On ImmunizationDocument56 pagesQuiz On ImmunizationFreniNo ratings yet
- Levy Mwanawasa Medical University School of Public Health and Environmental Sciences Department of Public HealthDocument5 pagesLevy Mwanawasa Medical University School of Public Health and Environmental Sciences Department of Public HealthChristían KanyataNo ratings yet
- Contraception HandoutDocument4 pagesContraception HandoutKazia BryantNo ratings yet
- Immunization Monitoring FormDocument4 pagesImmunization Monitoring FormDiler Singh100% (2)
- Moderna COVID-19 Vaccine Distribution Records for Wonosobo District Health OfficeDocument10 pagesModerna COVID-19 Vaccine Distribution Records for Wonosobo District Health OfficePuskesmas Kejajar 2No ratings yet
- COVID vaccination certificateDocument1 pageCOVID vaccination certificateLearn easy By Gajanan topaleNo ratings yet
- Pertussis/Whooping Cough: VACCINE - Pentavalent VaccineDocument13 pagesPertussis/Whooping Cough: VACCINE - Pentavalent VaccineLarmay dcsnNo ratings yet
- Materi DR DR Ari Prayitno SpAK Typhoid Vaccine - Current and New PlatformDocument40 pagesMateri DR DR Ari Prayitno SpAK Typhoid Vaccine - Current and New PlatformMutiara UtiNo ratings yet
- Is Your Child Up-To-Date With VaccinesDocument1 pageIs Your Child Up-To-Date With VaccinesTryinNo ratings yet
- $101 Million Award For Child With MMR Vaccine InjuryDocument1 page$101 Million Award For Child With MMR Vaccine InjuryFrank ReitemeyerNo ratings yet
- 2021 10 13 13-06-47 PMDocument1 page2021 10 13 13-06-47 PMabir AhmedNo ratings yet
- 60 IzovacDocument3 pages60 Izovacuzairch491No ratings yet
- COVID-19 Vaccines For Children and Teens - CDCDocument5 pagesCOVID-19 Vaccines For Children and Teens - CDCFabio PicassoNo ratings yet
- Vaccines, Cold Chain and Logistics Management: Manual of OperationsDocument148 pagesVaccines, Cold Chain and Logistics Management: Manual of Operationscesspintas Cuaresma67% (3)
- Urn Uvci 01 Ro 34g10kovy96n47l0kwnxldr7mepq5w#gDocument2 pagesUrn Uvci 01 Ro 34g10kovy96n47l0kwnxldr7mepq5w#gJohanna LenoraterianNo ratings yet
- COVID vaccination certificate issued in IndiaDocument1 pageCOVID vaccination certificate issued in IndiaYo YoNo ratings yet
- CertificateDocument1 pageCertificatenazmulNo ratings yet
- Dsm-Iv Definition of AdhdDocument2 pagesDsm-Iv Definition of Adhdapi-210243719No ratings yet
- Writing DSM 5 DiagnosisDocument2 pagesWriting DSM 5 Diagnosiscristina83% (6)
- The Deadly Impossibility of Herd Immunity Through Vaccination by DR Russell BlaylockDocument3 pagesThe Deadly Impossibility of Herd Immunity Through Vaccination by DR Russell BlaylockAsimuddin68No ratings yet
- Clinician Tabel Skizofrenia DSM VDocument4 pagesClinician Tabel Skizofrenia DSM VrayendrarenoNo ratings yet
- COVID-19 Guidance For Individuals Vaccinated Outside of OntarioDocument13 pagesCOVID-19 Guidance For Individuals Vaccinated Outside of OntarioAda Belen AlvarezNo ratings yet
- GRK CertificateDocument1 pageGRK CertificateRadha KrishnaNo ratings yet