Professional Documents
Culture Documents
10 1001@jama 2017 14825 PDF
10 1001@jama 2017 14825 PDF
Uploaded by
almandoOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
10 1001@jama 2017 14825 PDF
10 1001@jama 2017 14825 PDF
Uploaded by
almandoCopyright:
Available Formats
Research
JAMA | Original Investigation
Association of Blood Transfusion From Female Donors
With and Without a History of Pregnancy With Mortality
Among Male and Female Transfusion Recipients
Camila Caram-Deelder, MSc; Aukje L. Kreuger, MD; Dorothea Evers, MD; Karen M. K. de Vooght, PhD;
Daan van de Kerkhof, PhD, MD; Otto Visser, PhD, MD; Nathalie C. V. Péquériaux, PhD; Francisca Hudig, PhD, MD;
Jaap Jan Zwaginga, PhD, MD; Johanna G. van der Bom, PhD, MD; Rutger A. Middelburg, PhD
Editorial page 1445
IMPORTANCE Transfusion of red blood cells from female donors has been associated with Animated Video Summary
increased mortality in male recipients.
Supplemental content
OBJECTIVE To quantify the association between red blood cell transfusion from female CME Quiz at
donors with and without a history of pregnancy and mortality of red blood cell recipients. jamanetwork.com/learning
DESIGN, SETTING, AND PARTICIPANTS Retrospective cohort study of first-time transfusion
recipients at 6 major Dutch hospitals enrolled from May 30, 2005, to September 1, 2015; the
final follow-up date was September 1, 2015. The primary analysis was the no-donor-mixture
cohort (ie, either all red blood cell transfusions exclusively from male donors, or all exclusively
from female donors without a history of pregnancy, or all exclusively from female donors with
a history of pregnancy). The association between mortality and exposure to transfusions
from ever-pregnant or never-pregnant female donors was analyzed using life tables and
time-varying Cox proportional hazards models.
EXPOSURES Red blood cell transfusions from ever-pregnant or never-pregnant female
donors, compared with red blood cell transfusions from male donors.
MAIN OUTCOMES AND MEASURES All-cause mortality during follow-up.
RESULTS The cohort for the primary analyses consisted of 31 118 patients (median age, 65
[interquartile range, 42-77] years; 52% female) who received 59 320 red blood cell
transfusions exclusively from 1 of 3 types of donors (88% male; 6% ever-pregnant female;
and 6% never-pregnant female). The number of deaths in this cohort was 3969 (13%
mortality). For male recipients of red blood cell transfusions, all-cause mortality rates after a
red blood cell transfusion from an ever-pregnant female donor vs male donor were 101 vs 80
deaths per 1000 person-years (time-dependent “per transfusion” hazard ratio [HR] for death,
1.13 [95% CI, 1.01-1.26]). For receipt of transfusion from a never-pregnant female donor vs
male donor, mortality rates were 78 vs 80 deaths per 1000 person-years (HR, 0.93 [95% CI,
0.81-1.06]). Among female recipients of red blood cell transfusions, mortality rates for an
ever-pregnant female donor vs male donor were 74 vs 62 per 1000 person-years (HR, 0.99
[95% CI, 0.87 to 1.13]); for a never-pregnant female donor vs male donor, mortality rates were
74 vs 62 per 1000 person-years (HR, 1.01 [95% CI, 0.88-1.15]).
CONCLUSIONS AND RELEVANCE Among patients who received red blood cell transfusions,
receipt of a transfusion from an ever-pregnant female donor, compared with a male donor,
was associated with increased all-cause mortality among male recipients but not among
female recipients. Transfusions from never-pregnant female donors were not associated with
increased mortality among male or female recipients. Further research is needed to replicate
these findings, determine their clinical significance, and identify the underlying mechanism.
Author Affiliations: Author
affiliations are listed at the end of this
article.
Corresponding Author: Rutger A.
Middelburg, PhD, Plesmanlaan 1a,
2333 BZ Leiden, the Netherlands
JAMA. 2017;318(15):1471-1478. doi:10.1001/jama.2017.14825 (r.a.middelburg@lumc.nl).
(Reprinted) 1471
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a University of Florida User on 10/21/2017
Research Original Investigation Association of Female-Donor Blood Transfusion and Recpient Mortality
T
ransfusion of red blood cells is among the most com-
monly performed procedures in hospitals.1 It has been Key Points
reported that mortality was increased after transfu-
Question Is there an association between red blood cell
sion of red blood cells from female donors compared with transfusion from female donors with and without a history of
male donors.2-7 The most common cause of transfusion- pregnancy and recipient mortality?
related mortality is transfusion-related acute lung injury
Findings In this cohort study that included 31 118 patients who
(TRALI), which has also been shown to be associated with
received red blood cell transfusions, receipt of a transfusion from
transfusions from female donors.8-10 Furthermore, TRALI is an ever-pregnant female donor was associated with a statistically
associated specifically with transfusions from female donors significant increase in all-cause mortality among male recipients of
with a history of pregnancy. 11,12 This raises the question red blood cell transfusions (hazard ratio, 1.13) but not among
whether the increased mortality after red blood cell transfu- female recipients (hazard ratio, 0.99).
sions could also depend on a history of pregnancy of the Meaning Receipt of red blood cell transfusion from female donors
donor. However, for TRALI it has been shown that only with a history of pregnancy was associated with increased
plasma-rich products confer a pregnancy-related antibody– mortality among male recipients; further research is needed to
mediated risk, whereas red blood cells do not. 10,11 The replicate these findings, determine their significance, and define
increased mortality in recipients of red blood cells from the underlying mechanism.
female donors may be related to either immunologic phe-
nomena or other mechanisms.
Any proposed immunologic mechanism is likely to be zero follow-up time and were not included in the denom-
dependent on a history of pregnancy of the donor. An inator. Similarly, a “single-transfusion” cohort also was
absence of association with pregnancy status of the donor selected, consisting of patients who received only a single
would suggest that other, nonimmunologic, mechanisms transfusion. Additionally, all analyses were repeated in the
are more likely. full cohort, to check whether any observed association
The aim of the current study was therefore to quantify the potentially depended on the selection of the no-donor-
association between red blood cell transfusion from female mixture cohort. The race/ethnicity of recipients and donors
blood donors, with and without a history of pregnancy, and was not recorded.
patient mortality in female and male transfusion recipients.
Recorded Data
Recipent Data
Information on transfusion recipients’ dates of birth, dates of
Methods death, and sex, as well as transfusion dates, product types,
Study Design and identification codes of transfused red blood cells, were
As previously described, a retrospective cohort of first- provided by the hospitals from electronic records of the
ever transfusion recipients, transfused from May 30, 2005, blood transfusion services. All transfusions, given for any
to September 1, 2015, in 6 major Dutch hospitals, was indication, were included. Mortality data were verified by the
established.13,14 All patients included in a previous study of hospitals until the date of data extraction. Mortality data
mortality after transfusion of red blood cells from female do- were considered complete because of the use of a nationally
nors were excluded from the current analyses to create an in- linked computer system and the legal requirement for report-
dependent cohort.2 ing all deaths to this system. The final follow-up date was
Ethical approval for this study was obtained from the in- September 1, 2015.
stitutional review board of the Leiden University Medical Cen-
ter and from local review boards of all participating centers. Donor and Blood Product Data
The review boards waived the need for informed consent, be- Information on donor dates of birth, sex, and pregnancy be-
cause only routinely collected data were processed after cod- fore donation (see the Supplement for details) were provided
ing to remove identifying information. by Sanquin (the national Dutch blood supply) and linked to re-
cipients’ data using the product identification codes of trans-
Population fused red blood cells. All blood products in the Netherlands
Primary analyses were performed in a “no-donor-mixture” are leukocyte-depleted by prestorage filtration, and nearly all
cohort, to avoid dilution of effects from mixing patients products are transfused ABO-RhD identically.
who received red blood cell transfusions from both male and
female donors. This cohort consisted of patients who Pregnancy of Female Blood Donors
received all their red blood cell transfusions exclusively from At their first donation, female blood donors self-reported
male donors, or all exclusively from female donors without any previous pregnancy. At all subsequent donations, they
a history of pregnancy (never-pregnant donors), or all exclu- reported whether they had been pregnant since the previ-
sively from female donors with a history of pregnancy ous donation. However, since some female donors had their
(ever-pregnant donors). Follow-up time was censored at the first-ever donation prior to the establishment of the current
time these inclusion criteria were violated. This censoring electronic recording system at the Sanquin blood bank, the
could occur at time 0, in which case recipients contributed answer to the question at first donation could be missing.
1472 JAMA October 17, 2017 Volume 318, Number 15 (Reprinted) jama.com
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a University of Florida User on 10/21/2017
Association of Female-Donor Blood Transfusion and Recpient Mortality Original Investigation Research
When the first donation was registered and the question were calculated according to standard formulas (additional
answered as never-pregnant, the pregnancy status was con- details reported in the Supplement).
sidered never-pregnant until the first subsequent donation
at which a pregnancy was reported. If the first donation was Time-Varying Cox Proportional Hazards Models
missing, the pregnancy status was considered unknown Cox proportional hazards models, including both time-
until the first subsequent donation at which a pregnancy varying and fixed variables, were fit to correct for potential
was reported. confounding. All confounding variables (ie, center [fixed],
recipients’ ABO-RhD blood group [fixed], age of the donor
Missing Data [time-varying], cumulative number of transfusions [time-
Information about donors’ pregnancy history was not varying], calendar year [time-varying], and an interaction
specifically recorded and was therefore missing for 44% term for center and number of transfusions [time-varying])
of donations from female donors (eTable 2 in the Supple- were included in the models as categorical variables, with as
ment). However, missingness depended solely on logistic many categories as there were exposure levels (details on
factors (ie, changes in the electronic recording of donor infor- potential confounders are reported in the Supplement).
mation over the years). These data were therefore expected For the time-varying analyses, values of variables could
to be “missing completely at random” (as also shown in change on each day with red blood cell transfusion. At
eTable 3 in the Supplement), allowing a valid “complete each day with red blood cell transfusion, the cumulative
case” analysis.15 We therefore selected only cases with com- number of red blood cell transfusions and of red blood
plete data available. cell transfusions from male, female never-pregnant, and
female ever-pregnant donors, up to and including that day,
Statistical Analyses were determined.
All statistical analyses were performed in Stata version 14.1.16 Exposures (ie, cumulative number of transfusions from
The only outcome assessed was all-cause mortality at any time never-pregnant or ever-pregnant female donors [time-
during follow-up, as specified per participating center (eTable varying]) were included in the models as continuous vari-
1 in the Supplement). ables. Consequently, hazard ratios (HRs) should be inter-
Survival analyses were performed with follow-up preted on a multiplicative scale. However, since the model
starting on the day of the first red blood cell transfusion. estimates the HR based on observed numbers of transfusions
Follow-up ended at death or on the reference day, only, the HRs should not be extrapolated beyond the ob-
determined for each hospital separately (eTable 1 in the served mean number of transfusions in each cohort (see eTable
Supplement). The reference 3 in the Supplement for an illustration of this interpretation).
day was the last day for The proportional hazards assumption was checked for all mod-
JAMA.COM + w h i c h t h e h o s p it a l h a d
provided data. Follow-up
els and no gross violations of this assumption were detected,
implying that the HR can be interpreted as a valid estimate of
time of rec ipients in the the average HR over the observed period.
d i f f e r e nt c o h o r t s w a s Separate models were run for the 2 different exposures
censored at the time the in- (ie, never-pregnant and ever-pregnant). For the no-donor-
c l u s i o n c r it e r i a f o r t h at mixture cohort, this meant exclusion of patients who
cohort were first violated. received any transfusions from the other exposure group,
To increase homogeneity, any transfusions with unknown pregnancy history, or a
Animated Summary Video
Mortality After Transfusion follow-up time of patients mixture of exposed (ie, ever-pregnant or never-pregnant,
From Female Blood Donors who received more than 15 depending on the analyses) and unexposed (ie, male) red
With and Without a History transfusions was censored at blood cell units. This way, the exposure group of interest
of Pregnancy
the time of the 16th transfu- was always compared directly with male donors, since all
sion. All analyses were strati- other units were excluded. For the full model, recipients of
fied by recipients’ sex. Trans- transfusions both from the exposure group of interest and
fusions of other blood products were ignored, because receipt from male donors were additionally included.
of these blood products was not correlated with sex and preg-
nancy history of the donor of red blood cells (eTable 3 in the Effect Measure Modification
Supplement). We previously reported effect measure modification by age
All reported P values are 2-sided, and P < .05 was consid- of the transfusion recipients.2 A primary objective of this
ered statistically significant. No adjustments for multiple com- study therefore was to repeat these analyses after stratifica-
parisons were performed. tion by age of the recipient for prespecified categories of age
(0-17, 18-50, 51-70, and ≥71 years). Effect-measure modifica-
Kaplan-Meier Analyses tion was formally quantified by adding interaction terms for
Kaplan-Meier curves were constructed for the single- age (P value for interaction trend across 4 categories, from
transfusion cohort. The analyses were limited to 3 years of a Z distribution using standard errors estimated from the
follow-up. At this time, differences in cumulative incidence observed information matrix) and sex of the recipient to
between different groups and 95% CIs for these differences the final model.
jama.com (Reprinted) JAMA October 17, 2017 Volume 318, Number 15 1473
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a University of Florida User on 10/21/2017
Research Original Investigation Association of Female-Donor Blood Transfusion and Recpient Mortality
Table 1. Characteristics of Female and Male Transfusion Recipients and Red Blood Cell Transfusions in the Different Cohorts
No-Donor-Mixture Cohorta Single-Transfusion Cohortb Full Cohort
Male Female Male Female Male Female
Characteristics (n=14 995) (n=16 123) (n=8463) (n=8496) (n=20 217) (n=21 915)
Deaths, No. (%) 1982 (13) 1987 (12) 606 (7) 590 (7) 3597 (18) 3378 (15)
Follow-up, 144 (6-1041) 351 (14-1275) 15 (1-717) 22 (1-781) 274 (18-1106) 479 (44-1316)
median (IQR), d
Person-time, 24 339 31 637 10 266 10 971 35 281 45 904
sum in years
Age of patients, 65 (45-75) 66 (39-78) 63 (3-75) 64 (21-78) 66 (50-75) 66 (43-78)
median (IQR), y
0 to 17 2813 (19) 2303 (14) 2534 (30) 2085 (25) 2986 (15) 2439 (11)
18 to 50 1427 (10) 2873 (18) 603 (7) 1073 (13) 2140 (11) 4246 (19)
51 to 70 5244 (35) 4253 (26) 2406 (28) 1966 (23) 7460 (37) 6112 (28)
≥71 5511 (37) 6694 (42) 2920 (35) 3372 (40) 7631 (38) 9118 (42)
Blood group,
No. (%)
O Rh+ 5426 (36) 5812 (36) 2945 (35) 2854 (34) 7366 (36) 7874 (36)
O Rh− 932 (6) 1024 (6) 502 (6) 562 (7) 1279 (6) 1388 (6)
A Rh+ 4977 (33) 5416 (34) 2670 (32) 2699 (32) 6805 (34) 7479 (34)
A Rh− 930 (6) 1051 (7) 476 (6) 548 (6) 1286 (6) 1433 (7)
B Rh+ 1240 (8) 1361 (8) 700 (8) 751 (9) 1698 (8) 1952 (9)
B Rh− 185 (1) 220 (1) 99 (1) 110 (1) 250 (1) 318 (1)
AB Rh+ 433 (3) 452 (3) 249 (3) 251 (3) 611 (3) 647 (3)
AB Rh− 75 (1) 86 (1) 50 (1) 45 (1) 114 (1) 115 (1)
Not defined 797 (5) 701 (4) 772 (9) 676 (8) 808 (4) 709 (3)
Transfusions 2 (1-2) 2 (1-2) 1 (1-1) 1 (1-1) 2 (1-3) 2 (2-3)
of red blood cell units
per patient, median (IQR)
Units of red blood cells 28 663 30 657 8463 8496 52 637 54 004
transfused, No. (%)
From male donors 25 190 (88) 27 155 (89) 6189 (73) 6243 (73) 40 022 (76) 41 267 (76)
From female 1818 (6) 1810 (6) 1190 (14) 1160 (14) 6528 (12) 6454 (12)
ever-pregnant donors
From female 1655 (6) 1692 (6) 1084 (13) 1093 (13) 6087 (12) 6283 (12)
never-pregnant donors
b
Abbreviation: IQR, interquartile range. Consists of patients with only a single red blood cell transfusion during the
a
Consists of all the follow-up time during which patients either received all their period in which they were followed up. Follow-up time was censored
red blood cell transfusions exclusively from male donors, or all exclusively at the time this inclusion criterion was violated.
from female donors without a history of pregnancy (never-pregnant donors),
or all exclusively from female donors with a history of pregnancy
(ever-pregnant donors).
These recipients were followed up for a median of 245
Results days (IQR, 9-1172) and had a median age of 65 years (IQR,
42-77); 16 123 (52%) were female. The number of deaths
Population in the no-donor-mixture cohort was 3969 (13%). Table 1
A total of 42 132 patients received 106 641 units of red blood shows a comparison of recipient characteristics between the
cells (76% from male donors, 12% from ever-pregnant no-donor-mixture cohort, single-transfusion cohort, and full
donors, 12% from never-pregnant female donors). The cohort, stratified by recipient sex.
median number of transfused units per recipient was 2 (inter-
quartile range [IQR], 2-3). These recipients were followed up Donors’ Pregnancy History and Mortality After Red Blood
for a median of 380 days (IQR, 27-1217), had a median age of Cell Transfusions
66 years (IQR, 46-77), and 21 915 (52%) were female. The Primary Analyses: No-Donor-Mixture Cohort
number of deaths was 6975 (17%). Among this full cohort, The HR for death after 1 additional unit of red blood cells from
31 118 patients received 59 320 units of red blood cells exclu- a never-pregnant female donor, compared with a unit from a
sively from 1 of the 3 types of donor (ie, the no-donor- male donor, was 0.93 (95% CI, 0.81 to 1.06) for male recipi-
mixture cohort: either all units exclusively from male donors, ents and 1.01 (95% CI, 0.88 to 1.15) for female recipients
exclusively from female donors without a history of preg- (Table 2).
nancy [never-pregnant donors], or exclusively from female The HR for death after 1 additional unit of red blood cells
donors with a history of pregnancy [ever-pregnant donors]). from an ever-pregnant female donor, compared with a unit
1474 JAMA October 17, 2017 Volume 318, Number 15 (Reprinted) jama.com
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a University of Florida User on 10/21/2017
Association of Female-Donor Blood Transfusion and Recpient Mortality Original Investigation Research
Table 2. Mortality Hazard Ratio of Male and Female Transfusion Recipients Exposed to Red Blood Cell Transfusions From Female
(Never-Pregnant or Ever-Pregnant) Donors vs Male Donors in the No-Donor-Mixture, Single-Transfusion, and Full Cohortsa
Male Recipients Female Recipients
No. of Deaths No. of Deaths
Among Recipients/ Among Recipients/
Donor Category No. of Recipients HR (95% CI)b P Value No. of Recipients HR (95% CI)b P Value
No-Donor-Mixture Cohortc
Male 1722/12 212 1 [Reference] 1752/13 332 1 [Reference]
Ever-pregnant female 1873/13 669 1.13 (1.01-1.26) .03 1871/14 770 0.99 (0.87-1.13) .92
Never-pregnant female 1831/13 538 0.93 (0.81-1.06) .29 1868/14 685 1.01 (0.88-1.15) .92
Single-Transfusion Cohortd
Male 434/6189 1 [Reference] 433/6243 1 [Reference]
Ever-pregnant female 532/7379 1.23 (0.98-1.54) .08 517/7403 1.12 (0.88-1.42) .37
Never-pregnant female 508/7273 0.96 (0.74-1.25) .75 506/7336 1.00 (0.77-1.30) .99
Full Cohorte
Ever-pregnant analysis
Male 2538/15 304 1 [Reference] 2448/16 617 1 [Reference]
Ever-pregnant female 2689/16 338 1.08 (1.02-1.15) .02 2567/17 654 0.99 (0.93-1.07) .87
Never-pregnant analysis
Male 2521/15 163 1 [Reference] 2447/16 608 1 [Reference]
Never-pregnant female 2630/16 091 1.06 (0.99-1.14) .08 2563/17 593 0.96 (0.89-1.03) .23
Abbreviation: HR, hazard ratio. from female donors with a history of pregnancy (ever-pregnant donors).
a d
All models adjusted for calendar year, blood group (ABO-RhD), hospital, age of Consists of participants who received only a single red blood cell transfusion
donor, cumulative number of transfusions, and an interaction term for hospital during the period of follow-up. Follow-up time was censored at the time this
and cumulative number of transfusions. inclusion criterion was violated.
b e
Hazard ratios per transfused unit compared with receiving a unit from a male Recipients in the full cohort could receive mixed blood from never-pregnant
blood donor. and male donors (for the never-pregnant analysis) or from ever-pregnant and
c
Consists of all the follow-up time during which patients received all their red blood male donors (for the ever-pregnant analysis); therefore, the number of male
cell transfusions exclusively from male donors, or all exclusively from female do- recipients receiving blood from never-pregnant female donors differs from the
nors without a history of pregnancy (never-pregnant donors), or all exclusively number receiving blood from ever-pregnant female donors.
from a male donor, was 1.13 (95% CI, 1.01 to 1.26) for male re- 18 through 50 years (Table 3). For female recipients, the HR
cipients and 0.99 (95% CI, 0.87 to 1.13) for female recipients for death after 1 additional unit of red blood cells from an ever-
(Table 2). pregnant female donor, compared with a male donor, was 0.99
The highest HRs for death after transfusion of red blood (95% CI, 0.93 to 1.07).
cells from ever-pregnant female donors were observed in male
recipients 50 years and younger (Table 3). Additional Results
Cumulative incidences of death, in the single-transfusion
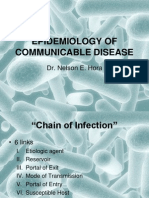
Secondary Analyses 1: Single-Transfusion Cohort cohort, at different follow-up times, are reported in eFigure
The 3 years cumulative incidence of death among male recipi- 3 and eTable 5 in the Supplement. eTable 3 reports the dis-
ents was 13.5% after a transfusion from a male donor, 13.1% tribution of donor types according to recipient sex and
after a transfusion from a never-pregnant female donor (dif- plasma and platelets transfusions received. Data on num-
ference, 0.4% [95% CI, −3.8% to 3.0%]), and 16.9% after a trans- bers of recipients, transfusions, and deaths per subgroup—
fusion from an ever-pregnant female donor (difference, 3.5% also for all female donors combined, regardless of preg-
[95% CI, −0.3% to 7.2%]) (Figure). nancy history—are reported in eTable 2 and eTables 6-8 in
The cumulative incidence of death among female recipi- the Supplement. Results of analyses of red blood cells cor-
ents was 12.6% after a transfusion from a male donor, 12.0% rected for plasma and platelet transfusions are reported in
after a transfusion from a never-pregnant female donor (dif- eTables 9-10 in the Supplement. Results of analyses for
ference, 0.6% [95% CI, −3.7% to 2.6%]), and 15.9% after a trans- female donors with unknown pregnancy history are shown
fusion from an ever-pregnant female donor (difference, 3.3% in eTable 11 and eFigure 4 in the Supplement. A direct com-
[95% CI, −0.5% to 7.1%]) (Figure). parison between ever-pregnant and never-pregnant female
donors is reported in eTable 12 in the Supplement. Analyses
Secondary Analyses 2: Full Cohort of platelet transfusions are reported in eTables 13-14 in the
The HR for death after 1 additional unit of red blood cells from Supplement.
an ever-pregnant female donor, compared with a male do-
nor, was 1.08 (95% CI, 1.02 to 1.15) for all male recipients, 1.18 Effect Measure Modification
(95% CI, 0.82 to 1.69) for male recipients aged 0 through 17 The tests for interaction for the association between transfu-
years, and 1.43 (95% CI, 1.13 to 1.82) for male recipients aged sion of red blood cells from ever-pregnant donors vs male
jama.com (Reprinted) JAMA October 17, 2017 Volume 318, Number 15 1475
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a University of Florida User on 10/21/2017
Research Original Investigation Association of Female-Donor Blood Transfusion and Recpient Mortality
Table 3. Mortality Hazard Ratio of Male Transfusion Recipients Exposed to Red Blood Cell Transfusions From Female Ever-Pregnant Donors
vs Male Donors in the No-Donor-Mixture, Single-Transfusion, and Full Cohorts, Stratified by Patient Agea
No. of Deaths Among Recipients/No. of Recipients, by Recipient Age
P Value for
Donor Category 0-17 y 18-50 y 51-70 y ≥71 y Interactionb
No-Donor-Mixture Cohortc
Male (reference) 107/2251 84/1170 598/4292 933/4499
Ever-pregnant female 124/2556 94/1296 645/4775 1010/5042
HR (95% CI)d 1.63 (1.02-2.61) 1.50 (0.98-2.30) 1.10 (0.91-1.33) 1.06 (0.90-1.26) .10
P value .04 .06 .31 .47
Single-Transfusion Cohorte
Male (reference) 53/1993 16/411 129/1686 236/2099
Ever-pregnant female 70/2287 23/504 152/2049 287/2539
HR (95% CI)d 2.84 (1.58-5.12) 2.29 (0.89-5.93) 0.79 (0.50-1.25) 1.06 (0.78-1.46) <.001
P value .001 .09 .32 .71
Full Cohort
Male (reference) 124/2421 146/1565 922/5570 1346/5748
Ever-pregnant female 141/2645 156/1649 969/5917 1423/6127
HR (95% CI)d 1.18 (0.82-1.69) 1.43 (1.13-1.82) 1.01 (0.91-1.12) 1.02 (0.93-1.12) <.001
P value .37 .003 .85 .63
Abbreviation: HR, hazard ratio. exclusively from female donors with a history of pregnancy (ever-pregnant
a
All models are adjusted for calendar year, blood group (ABO-RhD), hospital, donors).
d
age of donor, cumulative number of transfusions, and an interaction term for Hazard ratios per transfused unit compared with receiving a unit from a male
hospital and cumulative number of transfusions. blood donor.
b e
For the trend in interaction across the 4 presented categories of patient age. Consists of patients who received only a single red blood cell transfusion
c
Consists of all the follow-up time during which patients received all their red during the period of follow-up. Follow-up time was censored at the time this
blood cell transfusions exclusively from male donors, or all exclusively from inclusion criterion was violated.
female donors without a history of pregnancy (never-pregnant donors), or all
Figure. Cumulative Incidence of Death According to Sex of the Transfusion Recipient and Sex and Pregnancy History of the Donor
in the Single-Transfusion Cohort
Male recipients of red blood cell transfusions Female recipients of red blood cell transfusions
18 18
16 16
14 14
Cumulative Mortality, %
Cumulative Mortality, %
12 12
10 10
8 8
Blood donor group
6 Male 6
Female
4 Ever pregnant 4
2 Never pregnant 2
0 0
0 0.5 1.0 1.5 2.0 2.5 3.0 0 0.5 1.0 1.5 2.0 2.5 3.0
Years Years
No. at risk by donor group
Male 6189 2408 2102 1833 1624 1421 1236 6243 2598 2296 1990 1726 1484 1278
Female
Ever pregnant 1190 438 367 305 245 197 163 1160 456 371 303 243 197 166
Never pregnant 1084 393 331 279 225 177 146 1093 425 353 294 255 211 172
The single-transfusion cohort consists of all the follow-up time during which 1-567) days; and to female never-pregnant donors, 14 (IQR, 1-563) days. Median
patients had received only a single transfusion. Follow-up time was censored at follow-up for female recipients of red blood cell transfusions exposed to male
the time this inclusion criterion was violated. Median follow-up for male donors, 24 (IQR, 1-846) days; to female ever-pregnant donors, 21 (IQR, 1-584)
recipients of red blood cell transfusions exposed to male donors, 16 days; to female never-pregnant donors, 17 (IQR, 1-640) days.
(interquartile range [IQR], 1-780) days; to female ever-pregnant donors, 12 (IQR,
donors and mortality among male vs female recipients cohort, P = .54 for the single-transfusion cohort. and P = .58
regardless of recipient age did not meet statistical signifi- for the full cohort). The strength of the association between
cance (P = .30 for interaction for the no-donor-mixture transfusion of red blood cells from ever-pregnant donors and
1476 JAMA October 17, 2017 Volume 318, Number 15 (Reprinted) jama.com
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a University of Florida User on 10/21/2017
Association of Female-Donor Blood Transfusion and Recpient Mortality Original Investigation Research
mortality of male recipients was different for recipients of naturally occurring variation, quality control standards allow
different ages, as indicated by the P value for interaction up to 5 million leukocytes in a small percentage of products.
trend (Table 3). These could include both antigen-specific lymphocytes or
Similarly, the differences between male and female recipi- regulatory T cells.
ents in the strength of association of transfusions from ever- Some differences exist between results reported from stud-
pregnant donors with mortality of recipients 50 years and ies on the association between donor sex and recipient
younger were statistically significant (P = .03 for interaction mortality.2-6 These differences could, in the light of the cur-
for the no-donor-mixture cohort, P = .01 for the single- rent results, potentially be explained by a combination of dif-
transfusion cohort, and P = .01 for the full cohort). ferences in prevalence of a history of pregnancy among do-
nors and differences in age distribution of recipients.
This study has several strengths. The large size of the
cohort allowed selection of the no-donor-mixture cohort and
Discussion enabled study of patients who received blood transfusions
The results from this large retrospective cohort study suggest from only 1 type of donor (ie, male vs previously pregnant
that the association of transfusions of red blood cells from female vs never pregnant female). However, the selection of
female donors with increased mortality among male recipi- a no-donor-mixture cohort could limit generalizability. The
ents was related to the pregnancy history of female donors recipients in the no-donor-mixture cohort receive fewer
and the age of the patient. Male recipients who received a transfusions, since the probability of receiving mixed trans-
transfusion from an ever-pregnant female donor had a statis- fusions increases with the total number of transfusions. Simi-
tically significant increase in mortality compared with those larly, the censoring of recipients who received 16 or more
who received a transfusion from a male donor or from a transfusions could limit generalizability to this group.
female donor without a history of pregnancy. There was no This study also has limitations. First, the difference in ef-
significant association between pregnancy status of female fect size and direction between male and female recipients was
donors of red blood cells and mortality among female recipi- not significant among recipients of all ages, only among those
ents of red blood cell transfusions. 50 years and younger. This makes the findings very tentative,
The association of increased mortality among male and they require validation in other studies. Second, this study
patients who received transfusions from ever-pregnant was retrospective, and data were recorded for routine clinical
donors suggests a possible mechanism based on immuno- practice and not specifically for this study. This could cause
logic changes occurring during pregnancy. Of all changes both inaccuracy of data and unavailability of data. Third, there
occurring during pregnancy, the immunologic ones are the were missing data, particularly regarding pregnancy status for
most enduring. An alternative explanation could be a differ- the women donating red blood cells. Fourth, information on
ence in iron status between ever-pregnant female and male cause of death was not available. Fifth, there may have been
donors. Iron deficiency in donors has recently been shown to residual confounding or confounding by an unidentified vari-
be associated with worse recovery of red blood cells after able. Sixth, the analysis included a large number of compari-
transfusion in a murine model.17 Some studies also report sons, but there was no adjustment for multiple comparisons.
differences in red blood cell physiology between the
sexes.13-17 Results from studies on the association of donor
sex and recipient mortality, including the current study, tend
to be consistent in showing associations for male recipients
Conclusions
but not for female recipients.2-6 This specificity for male Among patients who received red blood cell transfusions, re-
recipients seems difficult to explain based on differences in ceipt of a transfusion from an ever-pregnant female donor,
red blood cell physiology, supporting a possible role for a sex- compared with a male donor, was associated with increased
specific immunologic mechanism. It is difficult to predict all-cause mortality among male recipients but not among fe-
whether the small amount of plasma in red blood cell trans- male recipients. Transfusions from never-pregnant female do-
fusions contains enough antibodies to confer an increased nors were not associated with increased mortality among male
risk of mortality, but it cannot be ruled out. Furthermore, or female recipients. Further research is needed to replicate
leukocyte-depleted red blood cell transfusions routinely con- these findings, determine their clinical significance, and iden-
tain fewer than 1 million leukocytes. However, to allow for tify the underlying mechanism.
ARTICLE INFORMATION Leiden University Medical Centre, Leiden, Hospital, ‘s-Hertogenbosch, the Netherlands
Accepted for Publication: September 8, 2017. the Netherlands (Evers, Zwaginga); Department of (Péquériaux); LabWest, Haga Teaching Hospital,
Clinical Chemistry and Haematology, University The Hague, the Netherlands (Hudig).
Author Affiliations: Center for Clinical Transfusion Medical Center Utrecht, Utrecht, the Netherlands
Research, Sanquin Research, Leiden, the Author Contributions: Ms Caram-Deelder and
(de Vooght); Department of Clinical Chemistry Dr Middelburg had full access to all of the data in
Netherlands (Caram-Deelder, Kreuger, Evers, and Haematology, Catharina Hospital, Eindhoven,
Zwaginga, van der Bom, Middelburg); Department the study and take responsibility for the integrity of
the Netherlands (van de Kerkhof); Department the data and the accuracy of the data analysis.
of Clinical Epidemiology, Leiden University Medical of Haematology, VU Medical Center, Amsterdam,
Center, Leiden, the Netherlands (Caram-Deelder, Concept and design: Caram-Deelder, Zwaginga,
the Netherlands (Visser); Department of Clinical van der Bom, Middelburg.
Kreuger, van der Bom, Middelburg); Department of Chemistry and Haematology, Jeroen Bosch
Immunohaematology and Blood Transfusion,
jama.com (Reprinted) JAMA October 17, 2017 Volume 318, Number 15 1477
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a University of Florida User on 10/21/2017
Research Original Investigation Association of Female-Donor Blood Transfusion and Recpient Mortality
Acquisition, analysis, or interpretation of data: REFERENCES 9. West FB, Silliman CC. Transfusion-related acute
Caram-Deelder, Kreuger, Evers, de Vooght, 1. Pfuntner A, Wier LM, Stocks C. Most Frequent lung injury: advances in understanding the role of
van de Kerkhof, Visser, Péquériaux, Hudig, Procedures Performed in U.S. Hospitals, 2011. proinflammatory mediators in its genesis. Expert
van der Bom, Middelburg. Rockville, MD: Agency for Healthcare Research and Rev Hematol. 2013;6(3):265-276.
Drafting of the manuscript: Caram-Deelder, Quality; 2006. Statistical Brief 165. 10. Middelburg RA, Van Stein D, Zupanska B, et al.
Middelburg. Female donors and transfusion-related acute lung
Critical revision of the manuscript for important 2. Middelburg RA, Briët E, van der Bom JG.
Mortality after transfusions, relation to donor sex. injury: a case-referent study from the International
intellectual content: All authors. TRALI Unisex Research Group. Transfusion. 2010;
Statistical analysis: Caram-Deelder, Kreuger, Vox Sang. 2011;101(3):221-229.
50(11):2447-2454.
van der Bom. 3. Barty RL, Cook RJ, Lui Y, Acker JP, Eikelboom JW,
Obtained funding: van der Bom, Middelburg. Heddle NM. Exploratory analysis of the association 11. Middelburg RA, van Stein D, Atsma F, et al.
Administrative, technical, or material support: Evers, between donor sex and in hospital mortality in Alloexposed blood donors and transfusion-related
de Vooght, van de Kerkhof, Péquériaux, Hudig. transfusion recipients. Presented at: AABB Annual acute lung injury: a case-referent study. Transfusion.
Supervision: Visser, van der Bom, Middelburg. Meeting 2015; October 24-27, 2015; Anaheim, CA. 2011;51(10):2111-2117.
Conflict of Interest Disclosures: All authors have 4. Bjursten H, Dardashti A, Björk J, Wierup P, 12. Middelburg RA, Porcelijn L, Lardy N, Briët E,
completed and submitted the ICMJE Form for Algotsson L, Ederoth P. Transfusion of Vrielink H. Prevalence of leucocyte antibodies in the
Disclosure of Potential Conflicts of Interest. sex-mismatched and non-leukocyte-depleted red Dutch donor population. Vox Sang. 2011;100(3):
Dr Zwaginga reported receiving a speaking fee from blood cells in cardiac surgery increases mortality. 327-335.
Vifor Pharma and serving on the advisory councils J Thorac Cardiovasc Surg. 2016;152(1):223-232. 13. Evers D, Middelburg RA, de Haas M, et al.
of Novartis and Amgen Science. No other authors 5. Desmarets M, Bardiaux L, Benzenine E, et al. Red-blood-cell alloimmunisation in relation to
reported disclosures. Effect of storage time and donor sex of transfused antigens’ exposure and their immunogenicity:
Funding/Support: This study was funded by red blood cells on 1-year survival in patients a cohort study. Lancet Haematol. 2016;3(6):e284-
the Dutch Ministry of Health, Welfare and Sports undergoing cardiac surgery: an observational study. e292.
(grant PPOC-11-005). Transfusion. 2016;56(5):1213-1222. 14. Zalpuri S, Zwaginga JJ, van der Bom JG.
Role of the Funder/Sponsor: The Dutch Ministry of 6. Chassé M, Tinmouth A, English SW, et al. Risk factors for alloimmunisation after red blood
Health, Welfare and Sports had no role in the design Association of blood donor age and sex with cell transfusions (R-FACT): a case cohort study
and conduct of the study; collection, management, recipient survival after red blood cell transfusion. [published online May 4, 2012]. BMJ Open.
analysis, and interpretation of the data; JAMA Intern Med. 2016;176(9):1307-1314. doi:10.1136/bmjopen-2012-001150
preparation, review, or approval of the manuscript; 7. Chassé M, McIntyre L, English SW, et al. Effect of 15. Rubin DB. Inference and missing data. Biometrika.
and the decision to submit the manuscript for blood donor characteristics on transfusion 1976;63(3):581-592.
publication. outcomes: a systematic review and meta-analysis. 16. Stata Statistical Software [computer program].
Additional Contributions: We thank Bert Transfus Med Rev. 2016;30(2):69-80. Version 14.1. College Station, TX: StataCorp; 2015.
Mesman, BSc, and Herman Geerlings, BSc (Sanquin 8. Toy P, Popovsky MA, Abraham E, et al; National 17. Bandyopadhyay S, Brittenham GM, Francis RO,
Amsterdam), for data on the Dutch donor Heart, Lung and Blood Institute Working Group on Zimring JC, Hod EA, Spitalnik SL. Iron-deficient
population. No compensation was provided for TRALI. Transfusion-related acute lung injury: erythropoiesis in blood donors and red blood cell
this service. definition and review. Crit Care Med. 2005;33(4): recovery after transfusion: initial studies with a
721-726. mouse model. Blood Transfus. 2017;15(2):158-164.
1478 JAMA October 17, 2017 Volume 318, Number 15 (Reprinted) jama.com
© 2017 American Medical Association. All rights reserved.
Downloaded From: by a University of Florida User on 10/21/2017
You might also like
- Detailed Lesson Plan About BacteriaDocument7 pagesDetailed Lesson Plan About BacteriaLexter Gabica100% (3)
- Blood TransfusionDocument7 pagesBlood Transfusionmuhammad_ariefNo ratings yet
- Jama Neal 2023 Ed 230070 1696973944.14124Document2 pagesJama Neal 2023 Ed 230070 1696973944.14124Luz Elena ValderramaNo ratings yet
- Plasma Convalesen HLADocument19 pagesPlasma Convalesen HLAVincentius Michael WilliantoNo ratings yet
- TDR1Document7 pagesTDR1Santanico De CVT deozaNo ratings yet
- Karakteristik Pasien Transfusi Darah Dengan Inkompatibilitas Crossmatch Di UTD RSUP DR M Djamil PadangDocument5 pagesKarakteristik Pasien Transfusi Darah Dengan Inkompatibilitas Crossmatch Di UTD RSUP DR M Djamil PadangAesthetic GirlNo ratings yet
- Hubungan Hasil Uji Saring Darah Pada Donor Sukarela Dan Pengganti Di Rsud Rokan HuluDocument7 pagesHubungan Hasil Uji Saring Darah Pada Donor Sukarela Dan Pengganti Di Rsud Rokan HuluAulia NurrohmahNo ratings yet
- Articula 43de100Document14 pagesArticula 43de100RUBEN DARIO GUALOTU�A AYONo ratings yet
- Jurnal 1 MaterDocument4 pagesJurnal 1 MaterEvaliaRahmatPuzianNo ratings yet
- WJN 4 148Document13 pagesWJN 4 148Rafela Agatha ChristyNo ratings yet
- Accepted Manuscript: The American Journal of CardiologyDocument22 pagesAccepted Manuscript: The American Journal of CardiologyAlamgirNo ratings yet
- Dr. Manoj KumarDocument7 pagesDr. Manoj KumarPatna Journal of MedicineNo ratings yet
- Aloinmunizacion en IndiaDocument4 pagesAloinmunizacion en Indiabioqclin20No ratings yet
- Serum Neopterin Is Not Influenced by Age and BloodDocument7 pagesSerum Neopterin Is Not Influenced by Age and BloodPakSci MissionNo ratings yet
- Finch 2014Document8 pagesFinch 2014juanda raynaldiNo ratings yet
- Chec 2Document7 pagesChec 2JOSE PORTILLONo ratings yet
- Potential Harm of Prophylactic Platelet Transfusion in Adult Dengue PatientsDocument10 pagesPotential Harm of Prophylactic Platelet Transfusion in Adult Dengue PatientsReynaldo Rahima PutraNo ratings yet
- Transfusiones ECN Febrero 2018Document5 pagesTransfusiones ECN Febrero 2018alyss yasminNo ratings yet
- Prevalence of Rhesus Negativity Among Pregnant Women: Research ArticleDocument5 pagesPrevalence of Rhesus Negativity Among Pregnant Women: Research ArticlecindyamandaNo ratings yet
- 1 s2.0 S0735109710020851 MainDocument11 pages1 s2.0 S0735109710020851 Mainblooom_00No ratings yet
- Alloimmunization and Red Cellautoimmunization in Multitransfused Thalassemic of Indian OriginDocument5 pagesAlloimmunization and Red Cellautoimmunization in Multitransfused Thalassemic of Indian OriginFatimatuzzahra ShahabNo ratings yet
- Academic Emergency Medicine 2024 Long Fluid Volumes in Adults WithDocument2 pagesAcademic Emergency Medicine 2024 Long Fluid Volumes in Adults WithAdrianaIDCNo ratings yet
- Gender and Bladder CancerDocument11 pagesGender and Bladder CancernimaelhajjiNo ratings yet
- Transfusion RBCsDocument2 pagesTransfusion RBCsbrookswalshNo ratings yet
- Anemia After Kidney Transplantation in Adult Recipients Prevalence and Risk Factors (Đã In)Document3 pagesAnemia After Kidney Transplantation in Adult Recipients Prevalence and Risk Factors (Đã In)Mỹ HoàiNo ratings yet
- Diagnosis Treatment DVT Scarvelis CMAJ 061024Document4 pagesDiagnosis Treatment DVT Scarvelis CMAJ 061024farhanomeNo ratings yet
- Aplastic Anemia During Pregnancy: A Review of Obstetric and Anesthetic ConsiderationsDocument9 pagesAplastic Anemia During Pregnancy: A Review of Obstetric and Anesthetic Considerationsalston96No ratings yet
- Estudio RefillDocument15 pagesEstudio RefillmiltoncesargomezNo ratings yet
- Tranfusion Masiva y RetrasoDocument6 pagesTranfusion Masiva y RetrasoSergio ZhinaNo ratings yet
- Stroke in AusieDocument9 pagesStroke in AusieAnna AzizahNo ratings yet
- Thalassemia IndiaDocument4 pagesThalassemia IndiaDr Laxmikant Basavraj DamaNo ratings yet
- Postpartum Hemorrhage Is Related To The Hemoglobin Levels at Labor: Observational StudyDocument5 pagesPostpartum Hemorrhage Is Related To The Hemoglobin Levels at Labor: Observational StudyFeisal MoulanaNo ratings yet
- Restrictive or Liberal Red-Cell Transfusion For Cardiac SurgeryDocument11 pagesRestrictive or Liberal Red-Cell Transfusion For Cardiac SurgeryRadmila KaranNo ratings yet
- Anticoagulant Prophylaxis in Pregnant Women With A History of Venous ThromboembolismDocument23 pagesAnticoagulant Prophylaxis in Pregnant Women With A History of Venous ThromboembolismWilliam BarreraNo ratings yet
- Blooddonorsandbloodcollection: Blood Donors With Positive Direct Antiglobulin Tests Are at Increased Risk For CancerDocument5 pagesBlooddonorsandbloodcollection: Blood Donors With Positive Direct Antiglobulin Tests Are at Increased Risk For CancerLuis Enrique Tinoco JuradoNo ratings yet
- El Riesgo de Las Infecciones Trasmitidas Por TransfusionDocument6 pagesEl Riesgo de Las Infecciones Trasmitidas Por TransfusionArturo sagasteguiNo ratings yet
- NIH Public Access: Author ManuscriptDocument20 pagesNIH Public Access: Author ManuscriptSantiago PilataxiNo ratings yet
- The Effects of HIV Infection On Pregnancy Hormones Within 28 Weeks of PregnancyDocument5 pagesThe Effects of HIV Infection On Pregnancy Hormones Within 28 Weeks of PregnancyFani DisastraNo ratings yet
- Hepatic Encephalopathy Is A Strong Predictor of Early Hospital Readmission Among Cirrhosis PatientsDocument7 pagesHepatic Encephalopathy Is A Strong Predictor of Early Hospital Readmission Among Cirrhosis PatientsAhmad Harissul IbadNo ratings yet
- Albayrak 2016Document7 pagesAlbayrak 2016DavorIvanićNo ratings yet
- Osborn 2017Document22 pagesOsborn 2017uci 2No ratings yet
- DMSO 451628 Gender Differences in The Incidence of Nephropathy and ChangDocument15 pagesDMSO 451628 Gender Differences in The Incidence of Nephropathy and ChangBBD BBDNo ratings yet
- Efficacy of Red Blood Cell Transfusion in The Critically Ill (Original Article)Document8 pagesEfficacy of Red Blood Cell Transfusion in The Critically Ill (Original Article)Rayhan OemarNo ratings yet
- Stroke Prevention in Atrial Fibrillation....Document3 pagesStroke Prevention in Atrial Fibrillation....tristan9454No ratings yet
- MLR Untuk Deteksi TB AktifDocument7 pagesMLR Untuk Deteksi TB AktifDwika AudiyanandaNo ratings yet
- 加拿大食道癌Document8 pages加拿大食道癌Joseph ChenNo ratings yet
- Restrictive or Liberal Red-Cell Transfusion For Cardiac SurgeryDocument12 pagesRestrictive or Liberal Red-Cell Transfusion For Cardiac SurgeryFredy Alcides Ramos VelasquezNo ratings yet
- The PROPPR Randomized Clinical TrialDocument12 pagesThe PROPPR Randomized Clinical Trialnageur2017No ratings yet
- Allo 4 ProspectiveDocument4 pagesAllo 4 ProspectiveA ANo ratings yet
- Edit Translate Massive Blood Transfusions Post Trauma in The Elderly Compared To Younger PatientsDocument8 pagesEdit Translate Massive Blood Transfusions Post Trauma in The Elderly Compared To Younger PatientsrendysamanosukeNo ratings yet
- How We Diagnose and Treat Deep Vein Thrombosis.: Author InformationDocument18 pagesHow We Diagnose and Treat Deep Vein Thrombosis.: Author InformationligitafitranandaNo ratings yet
- MMF Si VHC TransplantDocument11 pagesMMF Si VHC TransplantdeliaNo ratings yet
- Proppr TrialDocument12 pagesProppr Trialriks21No ratings yet
- HPP Pengaruh Pada HBDocument6 pagesHPP Pengaruh Pada HBchanyundaNo ratings yet
- Bloodproducttransfusions Andreactions: Jessica L. Osterman,, Sanjay AroraDocument12 pagesBloodproducttransfusions Andreactions: Jessica L. Osterman,, Sanjay AroraAdi ParamarthaNo ratings yet
- Etude Transf PQDocument10 pagesEtude Transf PQLincan RoxanaNo ratings yet
- Gestational Hypertension and Preeclampsia in Living Kidney DonorsDocument10 pagesGestational Hypertension and Preeclampsia in Living Kidney Donorshidayatul rahmoNo ratings yet
- Vascular Access Type, Inflammatory Markers, and Mortality in Incident Hemodialysis PatientsDocument18 pagesVascular Access Type, Inflammatory Markers, and Mortality in Incident Hemodialysis PatientsYulius DonyNo ratings yet
- EstradiolmortalDocument9 pagesEstradiolmortalapi-3728652No ratings yet
- Umbilical Cord Blood Transplantation For The Treatment of Hematologic MalignanciesDocument15 pagesUmbilical Cord Blood Transplantation For The Treatment of Hematologic MalignanciesFederica AltomareNo ratings yet
- Blood Group Testing - An Experiment To Determine The Blood GroupDocument12 pagesBlood Group Testing - An Experiment To Determine The Blood GroupAbhay Kishore KaulNo ratings yet
- Blood AgarDocument4 pagesBlood Agarsyafa latifahNo ratings yet
- Sysmex KX 21 Histogram Interpretation HandbookDocument28 pagesSysmex KX 21 Histogram Interpretation Handbookسعد الطائع100% (4)
- Epidemiology of Communicable DiseaseDocument21 pagesEpidemiology of Communicable DiseaseElmer Patrick100% (2)
- Ubiquity and Cultural Characteristics of MicroorganismsDocument1 pageUbiquity and Cultural Characteristics of MicroorganismsM Pedroso100% (2)
- Administrative Order No. 201 S. 1973: Vela, Christine Jane V. September 16, 2020 MMLS 2-1Document44 pagesAdministrative Order No. 201 S. 1973: Vela, Christine Jane V. September 16, 2020 MMLS 2-1Jeanne ClaireNo ratings yet
- 1.4 Blood Types & RH FactorDocument1 page1.4 Blood Types & RH FactorTori RolandNo ratings yet
- Blood Component TherapyDocument10 pagesBlood Component TherapyMunish DograNo ratings yet
- Nosocomial InfectionDocument13 pagesNosocomial InfectionwabalyNo ratings yet
- Pathogenic Gram Positive BacteriaDocument34 pagesPathogenic Gram Positive BacteriaFahimRazmandehNo ratings yet
- CULTURE METHOD 2ndDocument3 pagesCULTURE METHOD 2ndsanu MinzNo ratings yet
- 2a Boardworks - Infectious Diseases 2 PDFDocument17 pages2a Boardworks - Infectious Diseases 2 PDFArshad KhanNo ratings yet
- Blood Typing GameDocument4 pagesBlood Typing GameWidjaya HS TeacherNo ratings yet
- Agar-Agar, Granulated: Product MonographsDocument1 pageAgar-Agar, Granulated: Product MonographsThiary CarvalhoNo ratings yet
- Abcd 20759Document1 pageAbcd 20759vaibhav shuklaNo ratings yet
- 26 Year Male 61620503543: Patient NameDocument2 pages26 Year Male 61620503543: Patient NameMoataz NazeemNo ratings yet
- VAN MHUTE - Microbiology and IDDocument4 pagesVAN MHUTE - Microbiology and IDVon Valentine MhuteNo ratings yet
- History of Antimicrobial Agents & Resistant BacteriaDocument6 pagesHistory of Antimicrobial Agents & Resistant BacteriaAnurrag KumarNo ratings yet
- Catheter Associated Urinary Tract InfectionsDocument16 pagesCatheter Associated Urinary Tract InfectionssalmaNo ratings yet
- Aloa Chromogenic Media For Listeria Sales Flyer Du407a PDFDocument2 pagesAloa Chromogenic Media For Listeria Sales Flyer Du407a PDFazalea freyaNo ratings yet
- Report On Etiology, Epidemiology, Clinic, DD, Treatment, Profilaxis of Typhoid Fever & ParathyphoidDocument3 pagesReport On Etiology, Epidemiology, Clinic, DD, Treatment, Profilaxis of Typhoid Fever & ParathyphoidAdnan Akram, MD (Latvia)No ratings yet
- Blood Bank Data Collection FormDocument3 pagesBlood Bank Data Collection Formpbta punjab100% (1)
- Mel John "MJ" Detabali Del Barrio: Employment Highlights Aotea Pathology: July 2009 To PresentDocument6 pagesMel John "MJ" Detabali Del Barrio: Employment Highlights Aotea Pathology: July 2009 To PresentMelJohn Detabali DelBarrioNo ratings yet
- List of Diseases Caused by Virus, Bacteria, Protozoa and WormDocument5 pagesList of Diseases Caused by Virus, Bacteria, Protozoa and WormShaik JainuddinNo ratings yet
- SPECIMEN COLLECTION and Processing For BACTERIOLOGY PDFDocument19 pagesSPECIMEN COLLECTION and Processing For BACTERIOLOGY PDFLPDF010596No ratings yet
- Serum Plate Agglutination SPA Test Demo E4bDocument1 pageSerum Plate Agglutination SPA Test Demo E4bRyan DevantaraNo ratings yet
- Ubiquity of MicroorganismsDocument17 pagesUbiquity of MicroorganismsAbdallah Essam Al-Zireeni75% (4)
- Human Health and DiseasesDocument72 pagesHuman Health and DiseasesBiju MylachalNo ratings yet
- Pretransfusion or Compatibility Testing: NotesDocument7 pagesPretransfusion or Compatibility Testing: NotesABHINABA GUPTANo ratings yet