You might also like
- Principles of Basic Clinical Pharmacokinetic ParametersDocument7 pagesPrinciples of Basic Clinical Pharmacokinetic ParametersThe Ghost By HarethNo ratings yet
- Handbook of Drug Interaction and the Mechanism of InteractionFrom EverandHandbook of Drug Interaction and the Mechanism of InteractionRating: 1 out of 5 stars1/5 (1)
- Pharmacology: Pharmacokinetic & Dose: Ana Khusnul Faizah Farmasi FK Uht 2018Document27 pagesPharmacology: Pharmacokinetic & Dose: Ana Khusnul Faizah Farmasi FK Uht 2018Aulia rahmawatiNo ratings yet
- Pharmacology in Drug Discovery: Understanding Drug ResponseFrom EverandPharmacology in Drug Discovery: Understanding Drug ResponseNo ratings yet
- Intravenous InfusionDocument9 pagesIntravenous InfusionMarina MuradNo ratings yet
- Essential Pharmacokinetics: A Primer for Pharmaceutical ScientistsFrom EverandEssential Pharmacokinetics: A Primer for Pharmaceutical ScientistsRating: 5 out of 5 stars5/5 (1)
- Pharmacokinetics: Bioavailability Volume of Distribution (VD)Document2 pagesPharmacokinetics: Bioavailability Volume of Distribution (VD)Ibraheem SairiNo ratings yet
- Non Linear PharmacokineticsDocument94 pagesNon Linear PharmacokineticsJaspreet Guraya100% (1)
- Pharmacology- The Molecular Dance: Understanding Drug Interactions: Harmony and Chaos: The Symphony of Drug InteractionsFrom EverandPharmacology- The Molecular Dance: Understanding Drug Interactions: Harmony and Chaos: The Symphony of Drug InteractionsNo ratings yet
- PharmacologyDocument32 pagesPharmacologyHarleanne ParkNo ratings yet
- Kinetics of Single and Multple Idoses of DrugsDocument46 pagesKinetics of Single and Multple Idoses of DrugsSunilNo ratings yet
- Content PDFDocument35 pagesContent PDFRaza Shamim AkhtarNo ratings yet
- 1 IntroductionDocument68 pages1 Introductiondona donneNo ratings yet
- Pharmaco KineticsDocument10 pagesPharmaco KineticsVithyaah ParameswaranNo ratings yet
- Principles and Basic Concepts of PharmacokineticsDocument4 pagesPrinciples and Basic Concepts of PharmacokineticsSurjeet ChauhanNo ratings yet
- Topic 9. Non-Linear PKDocument17 pagesTopic 9. Non-Linear PKjoseNo ratings yet
- 3 - Pharmakcokinetics & Pharmacodynamics: Apparent VolumeDocument10 pages3 - Pharmakcokinetics & Pharmacodynamics: Apparent VolumexCadisRaiNo ratings yet
- Clinical Pharmacokinetics Sample ChapterDocument44 pagesClinical Pharmacokinetics Sample Chapterpinkbutter100% (1)
- Ceutics CAT 2Document9 pagesCeutics CAT 2Ria KitlerNo ratings yet
- Application of PK in Clinical SitutionDocument42 pagesApplication of PK in Clinical Situtionsafia mehmood100% (1)
- Concept of Drug Delivery SystemDocument60 pagesConcept of Drug Delivery SystemokNo ratings yet
- Makalah KBM Kel 3Document32 pagesMakalah KBM Kel 3Novia RozadiNo ratings yet
- BASIC PHARMACOKINETIC CONCEPTSDocument4 pagesBASIC PHARMACOKINETIC CONCEPTSanirudh811100% (1)
- Trepanier2013 Applying Pharmacokinetics To Veterinary Clinical PracticeDocument14 pagesTrepanier2013 Applying Pharmacokinetics To Veterinary Clinical PracticeSarahNo ratings yet
- Biopharmaceutics 4rth USTC-2Document60 pagesBiopharmaceutics 4rth USTC-2Sonia BaruaNo ratings yet
- Therapeutic Drug Monitoring GuideDocument12 pagesTherapeutic Drug Monitoring GuideSharon GabrielNo ratings yet
- Pharmacokinetics Explained: Absorption, Distribution, Clearance & MoreDocument3 pagesPharmacokinetics Explained: Absorption, Distribution, Clearance & MoreJennifer HerediaNo ratings yet
- 1important DefinitionsDocument3 pages1important DefinitionsBest VideoNo ratings yet
- Bio Availability and Bio EquivalenceDocument32 pagesBio Availability and Bio Equivalenceكسلان اكتب اسمي100% (1)
- Clinical PharmacologDocument81 pagesClinical PharmacologSHILOTANo ratings yet
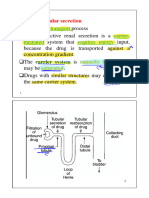
- 12) Drug Excretion and EliminationDocument14 pages12) Drug Excretion and EliminationManmeet Kohli IyerNo ratings yet
- IOM Pharmacology IDocument93 pagesIOM Pharmacology ISahara MahatNo ratings yet
- Pharmacokinetics of Anti-Epileptic DrugsDocument12 pagesPharmacokinetics of Anti-Epileptic Drugsrozina mulatNo ratings yet
- 1.1.1 Pharmacokinetics 2022 - 2023Document65 pages1.1.1 Pharmacokinetics 2022 - 2023brightgyan082No ratings yet
- Introduction To Biopharmaceutics and PharmacokineticsDocument29 pagesIntroduction To Biopharmaceutics and PharmacokineticsNasima Begum100% (1)
- 07 Dosage RegimenDocument44 pages07 Dosage Regimenzetttttttttt100% (3)
- C. Drug Action 1Document28 pagesC. Drug Action 1Jay Eamon Reyes MendrosNo ratings yet
- Bio PharmaceuticsDocument18 pagesBio PharmaceuticsHazel Ruth Yara Castillo100% (1)
- Updated NewDocument73 pagesUpdated NewAbhishek GaurNo ratings yet
- ChronopharmacokineticsDocument4 pagesChronopharmacokineticsTrương TrequartistaNo ratings yet
- Excretion and Elimination KineticsDocument39 pagesExcretion and Elimination KineticsYashasv BhatnagarNo ratings yet
- Pharmacokinetics: DR Narendra KumarDocument60 pagesPharmacokinetics: DR Narendra Kumarperala vinaykumarNo ratings yet
- بايو نظري المحاضرة الحادي عشرDocument25 pagesبايو نظري المحاضرة الحادي عشرtaha.21ph119No ratings yet
- PharmacokineticsDocument83 pagesPharmacokineticsdv94gw9zd8No ratings yet
- Bioavailability and Bioequivalence. Therapeutic Drug MonitoringDocument3 pagesBioavailability and Bioequivalence. Therapeutic Drug MonitoringJoel MathewNo ratings yet
- Intravenous Bolus Administration Part II PDFDocument44 pagesIntravenous Bolus Administration Part II PDFAlaa MansourNo ratings yet
- PharmacokineticsDocument10 pagesPharmacokineticsAnkit VermaNo ratings yet
- 2021-8-31 PharmacokineticsDocument25 pages2021-8-31 PharmacokineticsNOT ZUXNo ratings yet
- Sustained ReleasedDocument25 pagesSustained ReleasedKhalid HussainNo ratings yet
- Pharma 3Document12 pagesPharma 3Ibrahim dhainyNo ratings yet
- Adventist Medical Center College School of Nursing: Daverly M. Cañeda, R.N., M.NDocument174 pagesAdventist Medical Center College School of Nursing: Daverly M. Cañeda, R.N., M.NEvelyn MedinaNo ratings yet
- Multiple-Dosage Regimen (MDR) : Name: Md. Jabedul Alam Sarkar Id: 11715017 Department of Pharmacy, Comilla UniversityDocument14 pagesMultiple-Dosage Regimen (MDR) : Name: Md. Jabedul Alam Sarkar Id: 11715017 Department of Pharmacy, Comilla Universityjabed sarkarNo ratings yet
- Anesthesia Pharmacology CompiledDocument106 pagesAnesthesia Pharmacology CompiledJovy Tan-AmodiaNo ratings yet
- Sustained Release Drug Delivery System - A ReviewDocument14 pagesSustained Release Drug Delivery System - A ReviewPranav PatelNo ratings yet
- PRELIM WK 3 NCM 106 Phamacokenitics WeekDocument46 pagesPRELIM WK 3 NCM 106 Phamacokenitics WeekJaeNo ratings yet
- Assignment On-: "Pharmacokinetics of Drug Molecules in Different Disease Condition"Document19 pagesAssignment On-: "Pharmacokinetics of Drug Molecules in Different Disease Condition"Susmoy SinhaNo ratings yet
- Clinical Pharmacokinetics 2013Document68 pagesClinical Pharmacokinetics 2013Law YouNo ratings yet
- PHARMACOKINETICS & PharmacokineticsDocument60 pagesPHARMACOKINETICS & PharmacokineticsRaj PathakNo ratings yet
- Jan Aushadhi Yojana PMBJP BookDocument32 pagesJan Aushadhi Yojana PMBJP BookSRG100% (1)
- Case StudyDocument3 pagesCase StudyAJ BayNo ratings yet
- QuestranDocument2 pagesQuestranENo ratings yet
- RJPT AzithromycinDocument6 pagesRJPT AzithromycinRICKY GONZALI MAGONo ratings yet
- Pharmaco KineticsDocument427 pagesPharmaco KineticsMehrdad AvestaNo ratings yet
- Whole Bowel Irrigation For Gastrointestinal Decontamination of Overdose Patients Clin Tox 2014Document8 pagesWhole Bowel Irrigation For Gastrointestinal Decontamination of Overdose Patients Clin Tox 2014JOHANNA CATHERINE RUIZ CASTILLONo ratings yet
- Pharmacology I MCQs on General Pharmacological PrinciplesDocument34 pagesPharmacology I MCQs on General Pharmacological PrinciplesAman Gurjar100% (1)
- Top 40 SKU inventory reportDocument35 pagesTop 40 SKU inventory reportleidy andrea serrano caceresNo ratings yet
- Brief Guide To Common PainkillersDocument1 pageBrief Guide To Common Painkillers11113432No ratings yet
- Pharma Now or Never (V)Document27 pagesPharma Now or Never (V)Saktai DiyamiNo ratings yet
- Comparison of Hyperbaric Levobupivacaine/ Bupivacaine For Ceserean SectionDocument6 pagesComparison of Hyperbaric Levobupivacaine/ Bupivacaine For Ceserean SectionIJAR JOURNALNo ratings yet
- Astrazeneca India Private Limited: Advantage KarnatakaDocument3 pagesAstrazeneca India Private Limited: Advantage KarnatakaPrasath GNo ratings yet
- AnaesthesiaDocument5 pagesAnaesthesiaMagesh G Kshathriyan CheyyurNo ratings yet
- Algesia: 37.5 MG / 325 MG Film-Coated TABLET AnalgesicDocument1 pageAlgesia: 37.5 MG / 325 MG Film-Coated TABLET AnalgesicEsel WazowskiNo ratings yet
- Heartburn, and Acid Indigestion: Peptic Ulcer Pain, Acidity, HeartburnDocument2 pagesHeartburn, and Acid Indigestion: Peptic Ulcer Pain, Acidity, HeartburnPaoloNo ratings yet
- Drug Safety Monitoring GuidelinesDocument6 pagesDrug Safety Monitoring GuidelinesShivam Malik100% (1)
- Respiratory PharmacologyDocument26 pagesRespiratory PharmacologyShashanka PoudelNo ratings yet
- MetronidazoleDocument2 pagesMetronidazoleGwyn RosalesNo ratings yet
- Module 16 - Pharmacotherapy For Psychiatric DisordersDocument157 pagesModule 16 - Pharmacotherapy For Psychiatric Disordersgeekay79No ratings yet
- FlunitrazepamDocument20 pagesFlunitrazepamFemyNo ratings yet
- ProdrugsDocument23 pagesProdrugsMankaran SinghNo ratings yet
- ZPH EOPD Pharmacy - CDocument6 pagesZPH EOPD Pharmacy - CwondwossenNo ratings yet
- Pharmacogenetics and PharmacogenomicsDocument25 pagesPharmacogenetics and PharmacogenomicsBogdan CoșmanNo ratings yet
- Daftar Obat Apotek KumaraDocument36 pagesDaftar Obat Apotek Kumaraigd ponekNo ratings yet
- Leaflet - Clofazimine Tablets 100mgDocument1 pageLeaflet - Clofazimine Tablets 100mgdillah azhariNo ratings yet
- Inmed Product List InmesDocument16 pagesInmed Product List InmesInmed TherapeuticsNo ratings yet
- List Harga ObatDocument11 pagesList Harga Obatklinik girimukti medical centerNo ratings yet
- Patient Information Leaflet Loratadine 10mg TabletsDocument2 pagesPatient Information Leaflet Loratadine 10mg TabletsFREDNo ratings yet
- Update Stok 19 Maret 2019Document14 pagesUpdate Stok 19 Maret 2019ayu RachmawatiNo ratings yet
- Is That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeFrom EverandIs That a Fact?: Frauds, Quacks, and the Real Science of Everyday LifeRating: 4.5 out of 5 stars4.5/5 (3)
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincFrom EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincRating: 3.5 out of 5 stars3.5/5 (137)
- The Disappearing Spoon: And Other True Tales of Madness, Love, and the History of the World from the Periodic Table of the ElementsFrom EverandThe Disappearing Spoon: And Other True Tales of Madness, Love, and the History of the World from the Periodic Table of the ElementsRating: 4 out of 5 stars4/5 (146)
- Coating and Drying Defects: Troubleshooting Operating ProblemsFrom EverandCoating and Drying Defects: Troubleshooting Operating ProblemsRating: 5 out of 5 stars5/5 (1)
- Essential Oil Chemistry Formulating Essential Oil Blends that Heal - Aldehyde - Ketone - Lactone: Healing with Essential OilFrom EverandEssential Oil Chemistry Formulating Essential Oil Blends that Heal - Aldehyde - Ketone - Lactone: Healing with Essential OilRating: 5 out of 5 stars5/5 (1)
- Guidelines for Asset Integrity ManagementFrom EverandGuidelines for Asset Integrity ManagementRating: 5 out of 5 stars5/5 (1)
- Organic Chemistry for Schools: Advanced Level and Senior High SchoolFrom EverandOrganic Chemistry for Schools: Advanced Level and Senior High SchoolNo ratings yet
- Meltdown: Nuclear disaster and the human cost of going criticalFrom EverandMeltdown: Nuclear disaster and the human cost of going criticalRating: 5 out of 5 stars5/5 (5)
- An Introduction to the Periodic Table of Elements : Chemistry Textbook Grade 8 | Children's Chemistry BooksFrom EverandAn Introduction to the Periodic Table of Elements : Chemistry Textbook Grade 8 | Children's Chemistry BooksRating: 5 out of 5 stars5/5 (1)
- The Periodic Table of Elements - Post-Transition Metals, Metalloids and Nonmetals | Children's Chemistry BookFrom EverandThe Periodic Table of Elements - Post-Transition Metals, Metalloids and Nonmetals | Children's Chemistry BookNo ratings yet
- Chemistry at Home - A Collection of Experiments and Formulas for the Chemistry EnthusiastFrom EverandChemistry at Home - A Collection of Experiments and Formulas for the Chemistry EnthusiastNo ratings yet
- The Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsFrom EverandThe Regenerative Grower's Guide to Garden Amendments: Using Locally Sourced Materials to Make Mineral and Biological Extracts and FermentsRating: 5 out of 5 stars5/5 (3)
- Chemistry: a QuickStudy Laminated Reference GuideFrom EverandChemistry: a QuickStudy Laminated Reference GuideRating: 5 out of 5 stars5/5 (1)
- The Elements We Live By: How Iron Helps Us Breathe, Potassium Lets Us See, and Other Surprising Superpowers of the Periodic TableFrom EverandThe Elements We Live By: How Iron Helps Us Breathe, Potassium Lets Us See, and Other Surprising Superpowers of the Periodic TableRating: 3.5 out of 5 stars3.5/5 (22)
- The Periodic Table: A Very Short IntroductionFrom EverandThe Periodic Table: A Very Short IntroductionRating: 4.5 out of 5 stars4.5/5 (3)
- Science Goes Viral: Captivating Accounts of Science in Everyday LifeFrom EverandScience Goes Viral: Captivating Accounts of Science in Everyday LifeRating: 5 out of 5 stars5/5 (1)
- Stuff Matters: Exploring the Marvelous Materials That Shape Our Man-Made WorldFrom EverandStuff Matters: Exploring the Marvelous Materials That Shape Our Man-Made WorldRating: 4 out of 5 stars4/5 (289)
- Chemistry for Breakfast: The Amazing Science of Everyday LifeFrom EverandChemistry for Breakfast: The Amazing Science of Everyday LifeRating: 4.5 out of 5 stars4.5/5 (14)
- Gas-Liquid And Liquid-Liquid SeparatorsFrom EverandGas-Liquid And Liquid-Liquid SeparatorsRating: 3.5 out of 5 stars3.5/5 (3)
- Monkeys, Myths, and Molecules: Separating Fact from Fiction in the Science of Everyday LifeFrom EverandMonkeys, Myths, and Molecules: Separating Fact from Fiction in the Science of Everyday LifeRating: 4 out of 5 stars4/5 (9)
- Taste: Surprising Stories and Science About Why Food Tastes GoodFrom EverandTaste: Surprising Stories and Science About Why Food Tastes GoodRating: 3 out of 5 stars3/5 (20)