You might also like
- Pharmacokinetics: DR Narendra KumarDocument60 pagesPharmacokinetics: DR Narendra Kumarperala vinaykumarNo ratings yet
- Handbook of Drug Interaction and the Mechanism of InteractionFrom EverandHandbook of Drug Interaction and the Mechanism of InteractionRating: 1 out of 5 stars1/5 (1)
- Pharmacokinetics ADME GuideDocument81 pagesPharmacokinetics ADME GuideSiddh PatelNo ratings yet
- Drug Metabolism and EliminationDocument62 pagesDrug Metabolism and EliminationAshmita DhakalNo ratings yet
- Pharmacokinetics and Drug Disposition ExplainedDocument15 pagesPharmacokinetics and Drug Disposition Explainedsachin kumarNo ratings yet
- Pharmacology Guide to Pharmacokinetics and PharmacodynamicsDocument47 pagesPharmacology Guide to Pharmacokinetics and PharmacodynamicsْNo ratings yet
- PharmacokineticsDocument17 pagesPharmacokineticsღ آلَعٌرآقُيِة نِوٌر ღNo ratings yet
- 1 General PharmacologyDocument29 pages1 General PharmacologyAli EllaffiNo ratings yet
- Gen. Pharmacology Tests PDFDocument69 pagesGen. Pharmacology Tests PDFibrahim100% (2)
- Pharmaco KineticsDocument42 pagesPharmaco KineticsNaghman ZuberiNo ratings yet
- Elimination: G. SrikarDocument23 pagesElimination: G. SrikarSowjanya NekuriNo ratings yet
- Cell Response 2 NotesDocument15 pagesCell Response 2 Notespranjal shahNo ratings yet
- 1997 Pharmacology Semester 1 Page 1 of 4Document4 pages1997 Pharmacology Semester 1 Page 1 of 4ravi2like100% (1)
- 3.Unit.pharmacokinetics 2Document40 pages3.Unit.pharmacokinetics 22020253350No ratings yet
- Pharmacokinetics: Biological MembraneDocument18 pagesPharmacokinetics: Biological MembraneRahul PalsNo ratings yet
- Metabolic Pathway & Renal ExcretionDocument29 pagesMetabolic Pathway & Renal ExcretionRadha krishnaNo ratings yet
- Pharmacokinetics and Drug DistributionDocument6 pagesPharmacokinetics and Drug DistributionRumana ShaikhNo ratings yet
- PsychopharmacologyDocument64 pagesPsychopharmacologyGaurav Tandon100% (2)
- Fate of The Drug: Joanne Katherine T. Manlusoc, MSCDocument29 pagesFate of The Drug: Joanne Katherine T. Manlusoc, MSCChinenye AkwueNo ratings yet
- Pharmacokinetics: "What The Body Does To The Drug"Document41 pagesPharmacokinetics: "What The Body Does To The Drug"Virgo Eri SendiNo ratings yet
- Lecture 2 - Basic Concepts of PharmacokineticsDocument63 pagesLecture 2 - Basic Concepts of Pharmacokineticsahmadslayman1No ratings yet
- Drug Metabolism and EliminationDocument67 pagesDrug Metabolism and EliminationPrasiddhika LamsalNo ratings yet
- PharmacologyDocument92 pagesPharmacologyAbdallah Essam Al-ZireeniNo ratings yet
- بيDocument48 pagesبيMojied AmeerNo ratings yet
- 1.1.1 Pharmacokinetics 2022 - 2023Document65 pages1.1.1 Pharmacokinetics 2022 - 2023brightgyan082No ratings yet
- Lecture PharmacokineticsDocument55 pagesLecture Pharmacokineticssatya narayan100% (2)
- PharmaDocument147 pagesPharmaDrChauhanNo ratings yet
- 2021-8-31 PharmacokineticsDocument25 pages2021-8-31 PharmacokineticsNOT ZUXNo ratings yet
- 1 - Renal Excretion of DrugsDocument18 pages1 - Renal Excretion of DrugsKashar SaeedNo ratings yet
- Pharmacokinetics 1Document18 pagesPharmacokinetics 1mitranazari036No ratings yet
- Per 1 - 4 Farmakologi UmumDocument98 pagesPer 1 - 4 Farmakologi UmumamaliahriskaikaNo ratings yet
- Basics of Pharmacology: Speaker - DR - SantoshDocument76 pagesBasics of Pharmacology: Speaker - DR - SantoshRamya ChallaNo ratings yet
- PK, PD, Drug Interaction and Toxicology Bmls3 2020 2Document189 pagesPK, PD, Drug Interaction and Toxicology Bmls3 2020 2Kenny NgowiNo ratings yet
- Absorption DistributionDocument49 pagesAbsorption DistributionNorms Yoram100% (1)
- Lecture-4.Drug Metabolism and EliminationDocument47 pagesLecture-4.Drug Metabolism and EliminationC/fataax C/xakiimNo ratings yet
- EliminationDocument35 pagesEliminationPrathamesh PatilNo ratings yet
- PK, PD and Fate of Drug-1Document59 pagesPK, PD and Fate of Drug-1Kenny NgowiNo ratings yet
- Pharmacokinetics Metabolism 2020Document70 pagesPharmacokinetics Metabolism 2020Levani KartvelishviliNo ratings yet
- RRR Pharma NotesDocument202 pagesRRR Pharma Notesarchana singhNo ratings yet
- Unit 1, Part 4 Clin. PKDocument11 pagesUnit 1, Part 4 Clin. PKshammaNo ratings yet
- Module 1: Part A: Pharmacological Principles and Safe Medication AdministrationDocument56 pagesModule 1: Part A: Pharmacological Principles and Safe Medication AdministrationKamil MominNo ratings yet
- Cyp 450Document32 pagesCyp 450kondaveeti sreenivasulu NaiduNo ratings yet
- Half Life & BioavailabilityDocument12 pagesHalf Life & Bioavailabilitydavid5king-3119No ratings yet
- Shahed Unit I Principles of Drug Therapy Part IIDocument2 pagesShahed Unit I Principles of Drug Therapy Part IIEsdras DountioNo ratings yet
- Nasib Obat Dalam Tubuh (Farmakokinetika) : Dr. Edy Suwarso, S.U., AptDocument32 pagesNasib Obat Dalam Tubuh (Farmakokinetika) : Dr. Edy Suwarso, S.U., AptpintataNo ratings yet
- Pharmacokinetics: Dr. Mizanur RahmanDocument46 pagesPharmacokinetics: Dr. Mizanur Rahmangl tousifNo ratings yet
- Absorption of DrugsDocument41 pagesAbsorption of DrugsSibtain100% (2)
- Drug Elimination Processes and FactorsDocument28 pagesDrug Elimination Processes and Factorsaman vermaNo ratings yet
- Principles of Drug ActionDocument42 pagesPrinciples of Drug ActionkjghlkdfjgNo ratings yet
- Introduction to PharmacologyDocument59 pagesIntroduction to PharmacologyMoza AlanziNo ratings yet
- Pharmacokinetics: "What The Body Does To The Drug"Document54 pagesPharmacokinetics: "What The Body Does To The Drug"Nur FadhilahNo ratings yet
- Non Linear PharmacokineticsDocument94 pagesNon Linear PharmacokineticsJaspreet Guraya100% (1)
- 3a Introduction To Drug TherapyDocument69 pages3a Introduction To Drug TherapynipoNo ratings yet
- Excretion Biotransformation Metabolism: Dr. AA Yas Drug Elimination and Clearance Drug EliminationDocument31 pagesExcretion Biotransformation Metabolism: Dr. AA Yas Drug Elimination and Clearance Drug EliminationMohannad AlfadhalNo ratings yet
- PharmacokineticsDocument25 pagesPharmacokineticsRajkishor YadavNo ratings yet
- C. Drug Action 1Document28 pagesC. Drug Action 1Jay Eamon Reyes MendrosNo ratings yet
- PHARMACOKINETICSDocument74 pagesPHARMACOKINETICSAndrew SilungweNo ratings yet
- Pharmacotherapeutics, Pharmacodynamics & Pharmacokinetics ExplainedDocument47 pagesPharmacotherapeutics, Pharmacodynamics & Pharmacokinetics ExplainedAshaNo ratings yet
- Pharmacology: Pharmacokinetic & Dose: Ana Khusnul Faizah Farmasi FK Uht 2018Document27 pagesPharmacology: Pharmacokinetic & Dose: Ana Khusnul Faizah Farmasi FK Uht 2018Aulia rahmawatiNo ratings yet
- Structure and function of sucroseDocument73 pagesStructure and function of sucrosetess_15No ratings yet
- Antigen Presentation SlidesDocument53 pagesAntigen Presentation SlidesShakti PatelNo ratings yet
- WEEK 6 BIOCHEMDocument9 pagesWEEK 6 BIOCHEMRobaina WisNo ratings yet
- chapter-3-CELL STRUCTURE TAXONOMYDocument54 pageschapter-3-CELL STRUCTURE TAXONOMYCza Mae ArsenalNo ratings yet
- Capitulo 1 Webster and Weber Introduction to FungiDocument39 pagesCapitulo 1 Webster and Weber Introduction to Fungidianacarranza148No ratings yet
- Cancer BiologyDocument31 pagesCancer BiologyGEETA MOHAN100% (1)
- BIOLOGYFINALanswers (1stedition)Document61 pagesBIOLOGYFINALanswers (1stedition)Abhinav VermaNo ratings yet
- Basic Chemistry (M.Phil)Document5 pagesBasic Chemistry (M.Phil)Shahidullah Kaisar ShovonNo ratings yet
- IX Class NotesDocument60 pagesIX Class NotesNitin ThakurNo ratings yet
- CHPT 3-4 Practice QuizDocument5 pagesCHPT 3-4 Practice QuizShanti Loyd100% (1)
- CSEC 1. Cell StructureDocument2 pagesCSEC 1. Cell Structureamanda whipple100% (1)
- LEC18 MembraneLipids 08Document12 pagesLEC18 MembraneLipids 08Mây Chính ChủNo ratings yet
- Laboratory Experiment 1 Water and Its PropertiesDocument6 pagesLaboratory Experiment 1 Water and Its PropertiesRenee Dwi Permata Messakaraeng100% (1)
- Materi Kuliah BHL (Moluska - Jurnal - 3) - 2021 DaringDocument20 pagesMateri Kuliah BHL (Moluska - Jurnal - 3) - 2021 DaringAlifia Nabilla PutriNo ratings yet
- Reaction of LipidsDocument5 pagesReaction of LipidsJason Raquin Roque89% (9)
- CH - 6, Vesicular TransportDocument29 pagesCH - 6, Vesicular TransportTony StarkNo ratings yet
- BM1011 2021 Study Guide Module 1 An Introduction To The Human BodyDocument45 pagesBM1011 2021 Study Guide Module 1 An Introduction To The Human BodyLaetitia ReyesNo ratings yet
- CELL-THE BASIC UNIT OF LIFEDocument79 pagesCELL-THE BASIC UNIT OF LIFEEkta Manglani100% (1)
- NUMS Extra Topics Highlighted SyllabusDocument82 pagesNUMS Extra Topics Highlighted SyllabusTariqNo ratings yet
- Presentation For Reporting in BiologyDocument61 pagesPresentation For Reporting in BiologyLovely Nhel EslomotNo ratings yet
- Yeast Micronutrient Requirements 2017Document4 pagesYeast Micronutrient Requirements 2017Vy NguyenNo ratings yet
- Formulation and Evaluation of Ketoconazole NiosomaDocument7 pagesFormulation and Evaluation of Ketoconazole NiosomaKevin Nauval KarimNo ratings yet
- Bms 07Document110 pagesBms 07Sabyasachi DasNo ratings yet
- Similarities and Differences Among Living ThingsDocument100 pagesSimilarities and Differences Among Living ThingsJordi Calderon MontesNo ratings yet
- Hormone Practice Test: StudentDocument17 pagesHormone Practice Test: StudentKayne SuratosNo ratings yet
- Catalogo MINICARTUCHOS-CAPSULAS - INGLSDocument18 pagesCatalogo MINICARTUCHOS-CAPSULAS - INGLSPapaleguas gamesNo ratings yet
- Biology of T Cruzi Annurev - Mi.27.100173.002023 73Document36 pagesBiology of T Cruzi Annurev - Mi.27.100173.002023 73mflorezmNo ratings yet
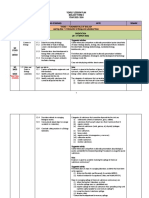
- Yearly Lesson Plan Bio F4 2023Document35 pagesYearly Lesson Plan Bio F4 2023Mss MinaNo ratings yet
- OsmosislabDocument8 pagesOsmosislabapi-328190492No ratings yet
- Paper For 01 11 09 Safe Hands Target GD andDocument1 pagePaper For 01 11 09 Safe Hands Target GD andnitinNo ratings yet