You might also like
- Research Penis EnlargementDocument10 pagesResearch Penis Enlargementalan100% (1)
- Opossum Orphan Care Booklet 2018Document53 pagesOpossum Orphan Care Booklet 2018Sonia Samaniego100% (1)
- Nursing ResearchDocument24 pagesNursing ResearchCamaligan Rocky0% (1)
- Socratic Dialogue and Guided Discovery in PDFDocument10 pagesSocratic Dialogue and Guided Discovery in PDFDaniel DragulescuNo ratings yet
- Shoulder Post-Operative Rehabilitation ProtocolsDocument6 pagesShoulder Post-Operative Rehabilitation ProtocolsShrutiNo ratings yet
- ACT Course HandbookDocument21 pagesACT Course HandbookRupali SharmaNo ratings yet
- CHN QuestionsDocument52 pagesCHN QuestionsJustin VergaraNo ratings yet
- Classification Systems in RPDDocument99 pagesClassification Systems in RPDRicky ArhiNo ratings yet
- Anti-Diabetic Medication - Wikipedia, The Free EncyclopediaDocument12 pagesAnti-Diabetic Medication - Wikipedia, The Free Encyclopediaumesh123patilNo ratings yet
- Nclex Review Pneumonia COPD AsDocument11 pagesNclex Review Pneumonia COPD Asmj078No ratings yet
- Prelim Exam PharmaDocument2 pagesPrelim Exam Pharmamj CanilangNo ratings yet
- Internet Addiction:: The Counselor'S EyeviewDocument125 pagesInternet Addiction:: The Counselor'S EyeviewDesiree Obtial LabioNo ratings yet
- CancerDocument5 pagesCancerDins PutrajayaNo ratings yet
- Exam Progam May 2024 PnleDocument3 pagesExam Progam May 2024 Pnlejimenezchristian1003No ratings yet
- CRRT Flex Operator Manual 5.1) PDFDocument284 pagesCRRT Flex Operator Manual 5.1) PDFalexNo ratings yet
- Fearless Forecast Nle 2019Document12 pagesFearless Forecast Nle 2019Mee AmorèNo ratings yet
- Allan Ocampo Tutorials: Mobile:0920-5583476 Bus.:273-2245Document55 pagesAllan Ocampo Tutorials: Mobile:0920-5583476 Bus.:273-2245ocampotutorials100% (1)
- PNLE IV For Care of Clients With Physiologic and Psychosocial Alterations (Part 2)Document23 pagesPNLE IV For Care of Clients With Physiologic and Psychosocial Alterations (Part 2)ASDF ASDFNo ratings yet
- NP1 Oxygenation PDFDocument21 pagesNP1 Oxygenation PDFLot RositNo ratings yet
- DM & DI ExamsDocument11 pagesDM & DI ExamsTomzki CornelioNo ratings yet
- July 2011 Nurse Licensure Examination Result July 2011 Nurse Board Exam ResultDocument28 pagesJuly 2011 Nurse Licensure Examination Result July 2011 Nurse Board Exam ResultDarren FloresNo ratings yet
- Neuro Senses Onco OrthoDocument11 pagesNeuro Senses Onco OrthoNom NomNo ratings yet
- Nursing Fundamentals Questions With RationaleDocument2 pagesNursing Fundamentals Questions With Rationalemae7777No ratings yet
- Set 4Document19 pagesSet 4Dick Morgan FerrerNo ratings yet
- CHNDocument7 pagesCHNRichard GeeNo ratings yet
- NP3Document12 pagesNP3rexinne noahNo ratings yet
- Community Health Nursing - Nclex QuestionsDocument13 pagesCommunity Health Nursing - Nclex QuestionsJESLINE ANTONYNo ratings yet
- EsblDocument16 pagesEsblsharmamaddy32No ratings yet
- Scope of This Nursing Test I Is Parallel To The NP1 NLE CoverageDocument15 pagesScope of This Nursing Test I Is Parallel To The NP1 NLE CoverageHanah Kanashiro AlcoverNo ratings yet
- Competency Appraisal - Diagnostic TestsDocument7 pagesCompetency Appraisal - Diagnostic TestsMj BrionesNo ratings yet
- Ca1 Diagnostic ExamDocument17 pagesCa1 Diagnostic ExamMJ O. JulianoNo ratings yet
- Siadh and Di QuestionsDocument18 pagesSiadh and Di QuestionsRegiever Salvante100% (1)
- Nurses Baguio 05-2024 (First Timer/Repeaters)Document59 pagesNurses Baguio 05-2024 (First Timer/Repeaters)PRC BaguioNo ratings yet
- Toprank Cardio Hema Post TestDocument5 pagesToprank Cardio Hema Post TestJoyce ObraNo ratings yet
- Test Questionson Leadershipand Management 28 Autosaved 29Document22 pagesTest Questionson Leadershipand Management 28 Autosaved 29Andrea Joy J. FAULANNo ratings yet
- Nur 111 Session 18 Sas 1Document11 pagesNur 111 Session 18 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- Ipass Processing: "Your International Exam Application Solution"Document2 pagesIpass Processing: "Your International Exam Application Solution"Pal Lex Lerons100% (1)
- Answers For Mentoring Activity #8Document5 pagesAnswers For Mentoring Activity #8Jazzmin Angel ComalingNo ratings yet
- Nursing Questions& AnswersDocument42 pagesNursing Questions& AnswersSanjeev Kumar100% (1)
- Critical Thinking Nursing Care LippincotsDocument35 pagesCritical Thinking Nursing Care Lippincotseric100% (1)
- COAP-Medical-Surgical-Nursing-Gastrointestinal-System-30-Items-JIZ DE ORTEGADocument9 pagesCOAP-Medical-Surgical-Nursing-Gastrointestinal-System-30-Items-JIZ DE ORTEGANicole OrtegaNo ratings yet
- Sudaria Ivy G. AnswerKeysDocument25 pagesSudaria Ivy G. AnswerKeysDeinielle Magdangal RomeroNo ratings yet
- NP 1 Nov 2014 NleDocument5 pagesNP 1 Nov 2014 NleSitts YhyNo ratings yet
- Diagnostic Exam IDocument14 pagesDiagnostic Exam IVia LatrasNo ratings yet
- ASTIG NURSE TOPIC 22 To 29Document7 pagesASTIG NURSE TOPIC 22 To 29Freddie BulsaraNo ratings yet
- Local Media5645742536622696181Document45 pagesLocal Media5645742536622696181Karen mae alvarroNo ratings yet
- Carl Rogers Erik Erikson Ivan Pavlov Albert Ellis B.F SkinnerDocument3 pagesCarl Rogers Erik Erikson Ivan Pavlov Albert Ellis B.F Skinnermark OrpillaNo ratings yet
- NCLEX Questions PneumoniaDocument2 pagesNCLEX Questions PneumoniaLovely Laranjo100% (1)
- Medical Surgical Nursing Review Questions Part 3Document8 pagesMedical Surgical Nursing Review Questions Part 3angelfire23phNo ratings yet
- CD One Exanthem GiDocument7 pagesCD One Exanthem GiNae OrdanozoNo ratings yet
- June 2007-NPT 4-Questions and RationaleDocument34 pagesJune 2007-NPT 4-Questions and RationaleLarissa AquinoNo ratings yet
- CHN RabeDocument24 pagesCHN RabeMichael Angelo Seña100% (1)
- 260 QuestionsDocument42 pages260 QuestionsMaryjoy Mertalla50% (4)
- Post Op Worksheet FinalDocument5 pagesPost Op Worksheet FinalRiza Angela BarazanNo ratings yet
- Nursing ExamDocument11 pagesNursing ExamGunan DwynethNo ratings yet
- Nle - July 2011Document12 pagesNle - July 2011shenric16100% (1)
- Cardiogenic Shock NCLEX Review QuizDocument6 pagesCardiogenic Shock NCLEX Review QuizRegie Marie EvangelistaNo ratings yet
- Nursing Board Exam Topics and Questions June 2009Document3 pagesNursing Board Exam Topics and Questions June 2009menuloud33% (3)
- Nursing Seminar 1 SAS Session 5Document8 pagesNursing Seminar 1 SAS Session 5Casey lopez BlandoNo ratings yet
- Nursing Practice IVDocument16 pagesNursing Practice IVJohn wewNo ratings yet
- CramsheetDocument54 pagesCramsheetRussel ManganopNo ratings yet
- Nursing Practice IVDocument11 pagesNursing Practice IVapi-3718174100% (1)
- np1 5Document25 pagesnp1 5Sittie Haya LazimNo ratings yet
- Nle 2019Document4 pagesNle 2019Jackie AbarraNo ratings yet
- Nursing Practice I Set A Nov 18Document11 pagesNursing Practice I Set A Nov 18Joshua GoNo ratings yet
- June 2009Document89 pagesJune 2009nokolip100% (2)
- Asthma and COPDDocument27 pagesAsthma and COPDTzaddi EaileyNo ratings yet
- Worksheet On Obstruction and AsthmaDocument14 pagesWorksheet On Obstruction and AsthmaKaye CorNo ratings yet
- Respiratory AnswersDocument8 pagesRespiratory AnswersMichael Jann Mendoza MoronesNo ratings yet
- Pharmacology MCQDocument1 pagePharmacology MCQmj CanilangNo ratings yet
- Chapter 46 Chest AssessmentDocument12 pagesChapter 46 Chest Assessmentmj CanilangNo ratings yet
- WHO Core Nurse Educator CompetenciesDocument1 pageWHO Core Nurse Educator Competenciesmj CanilangNo ratings yet
- Wifi HackingDocument3 pagesWifi Hackingmj CanilangNo ratings yet
- Grading System For NCM 103 - 103A - Funda SL and RDDocument2 pagesGrading System For NCM 103 - 103A - Funda SL and RDmj CanilangNo ratings yet
- Soliman SchedDocument1 pageSoliman Schedmj CanilangNo ratings yet
- Grading System For NCM 100 - Skills Lectute and RDDocument2 pagesGrading System For NCM 100 - Skills Lectute and RDmj CanilangNo ratings yet
- Funda RLE RD Time TableDocument4 pagesFunda RLE RD Time Tablemj CanilangNo ratings yet
- Alignment Matrix For PLOs Health AssessmentDocument4 pagesAlignment Matrix For PLOs Health Assessmentmj CanilangNo ratings yet
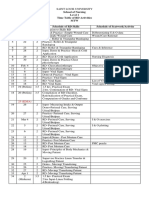
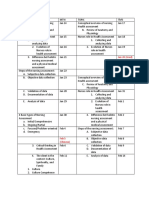
- School of Nursing Level 1 Time Table of RD Activities MTW Day Dates Hrs. Schedule of RD Skills Schedule of Seatwork/ActivityDocument4 pagesSchool of Nursing Level 1 Time Table of RD Activities MTW Day Dates Hrs. Schedule of RD Skills Schedule of Seatwork/Activitymj CanilangNo ratings yet
- PA Lec SchedDocument5 pagesPA Lec Schedmj CanilangNo ratings yet
- Wound CareDocument3 pagesWound Caremj CanilangNo ratings yet
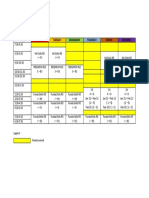
- Time Monday Tuesday Wednesday Thursday Friday SaturdayDocument1 pageTime Monday Tuesday Wednesday Thursday Friday Saturdaymj CanilangNo ratings yet
- Grading System For NCM 100 - Skills Lectute and RDDocument2 pagesGrading System For NCM 100 - Skills Lectute and RDmj CanilangNo ratings yet
- Schedule For Faculty Use - DHDocument1 pageSchedule For Faculty Use - DHmj CanilangNo ratings yet
- Time Monday Tuesday Wednesday Thursday Friday SaturdayDocument1 pageTime Monday Tuesday Wednesday Thursday Friday Saturdaymj CanilangNo ratings yet
- Teaching Problem Solving in Large Introductory Classes: The View From PhysicsDocument48 pagesTeaching Problem Solving in Large Introductory Classes: The View From PhysicsAlvaro H GalvisNo ratings yet
- 2016, Biofunctional ProstheticDocument6 pages2016, Biofunctional ProstheticlupitaNo ratings yet
- Burst Abdomen DR TotoDocument37 pagesBurst Abdomen DR TotofahlevyNo ratings yet
- 2023 Otago Exercise Program Guidance StatementDocument6 pages2023 Otago Exercise Program Guidance StatementAdultos Mayores Autovalentes CESFAM MAIPUNo ratings yet
- A Client Comes To The WalkDocument5 pagesA Client Comes To The WalkNovelyn Kaye Ramos CalanogaNo ratings yet
- A Study On Brand Awareness With Special Reference To Sna Oushadhasala Pvt. Ltd. ThrissurDocument45 pagesA Study On Brand Awareness With Special Reference To Sna Oushadhasala Pvt. Ltd. ThrissurT M Jishnu Das100% (1)
- Cervical Radiculopathy, How To Fix It - Google SearchDocument1 pageCervical Radiculopathy, How To Fix It - Google SearchMiguel AttiehNo ratings yet
- Procedure Sick Bay 2017Document6 pagesProcedure Sick Bay 2017Syed FareedNo ratings yet
- A.2003 - Distrofia Simpático-ReflexaDocument4 pagesA.2003 - Distrofia Simpático-ReflexaMisael RabeloNo ratings yet
- Pediatric Nursing NotesDocument21 pagesPediatric Nursing NotesFaye Nervanna Alecha AlferezNo ratings yet
- UntitledDocument12 pagesUntitledapi-241264935100% (1)
- Edwin Balita Job ResumeDocument5 pagesEdwin Balita Job Resumeedmybalita421No ratings yet
- Basic TB FactsDocument75 pagesBasic TB FactsFebrian Ivan PePeNo ratings yet
- US Cancer Generics Market Outlook 2022Document5 pagesUS Cancer Generics Market Outlook 2022Neeraj ChawlaNo ratings yet
- All About Rhabdo - Breaking Muscle: Delayed Onset Muscle SorenessDocument9 pagesAll About Rhabdo - Breaking Muscle: Delayed Onset Muscle SorenessChinmaya PatilNo ratings yet
- Diabetes in PregnancyDocument5 pagesDiabetes in PregnancyDoxo RubicinNo ratings yet
- Daptomycin: Eric ScholarDocument5 pagesDaptomycin: Eric ScholargluveNo ratings yet
- WFA Competency LevelsDocument5 pagesWFA Competency LevelsTroy Lyons DunowNo ratings yet
- Orthopedic DisordersDocument9 pagesOrthopedic DisordersDanielle_Liedt_563No ratings yet
- Chapter 15 - Obsessive-Ompulsive and Related DisordersDocument7 pagesChapter 15 - Obsessive-Ompulsive and Related Disordersmyer pasandalanNo ratings yet