You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Psoriasis Clinical Presentation - History, Physical Examination, Ocular ManifestationsDocument6 pagesPsoriasis Clinical Presentation - History, Physical Examination, Ocular ManifestationsclarissapamudjiNo ratings yet
- Lichen Simplex Chronicus - TreatmentDocument5 pagesLichen Simplex Chronicus - TreatmentclarissapamudjiNo ratings yet
- Jealous Nick JonasDocument2 pagesJealous Nick JonasclarissapamudjiNo ratings yet
- Divine SNSDDocument2 pagesDivine SNSDclarissapamudjiNo ratings yet
- Better Than Love - Sherina: I Didn't Even Know You Before Kept My Distance, Closing in I Don't Mind Caressing Your SkinDocument2 pagesBetter Than Love - Sherina: I Didn't Even Know You Before Kept My Distance, Closing in I Don't Mind Caressing Your SkinclarissapamudjiNo ratings yet
- Thyssenkrupp Industrial Solutions (India) Job Safety Analysis 1 6Document6 pagesThyssenkrupp Industrial Solutions (India) Job Safety Analysis 1 6Nitesh kumar yadavNo ratings yet
- L30-L132 RSDocument8 pagesL30-L132 RSMaulana FathanyNo ratings yet
- Guia InglesDocument13 pagesGuia InglesKevin Alexis Amaya Pinto “cuberlite”No ratings yet
- Chapter-2 PERCEPTIONDocument29 pagesChapter-2 PERCEPTIONSuman BhandariNo ratings yet
- Safety and Product Information: Blackberry Curve 9300 SmartphoneDocument46 pagesSafety and Product Information: Blackberry Curve 9300 SmartphonebienanwarNo ratings yet
- Introducing The Adafruit Bluefruit LE Sniffer: Created by Kevin TownsendDocument44 pagesIntroducing The Adafruit Bluefruit LE Sniffer: Created by Kevin TownsendRickScheck4567No ratings yet
- Aman Foundation Internship Application FormDocument4 pagesAman Foundation Internship Application Formabdullahnisar92No ratings yet
- Latitudes and LongitudesDocument31 pagesLatitudes and LongitudesHarsh Vardhan BaranwalNo ratings yet
- Covid 19 y Trombosis VacunasDocument7 pagesCovid 19 y Trombosis VacunasSMIBA MedicinaNo ratings yet
- Industrial Training Presentation: University of Engineering & Technology, Lahore, KSK CampusDocument30 pagesIndustrial Training Presentation: University of Engineering & Technology, Lahore, KSK CampusAbid HussainNo ratings yet
- SCP Dharamshala 1Document50 pagesSCP Dharamshala 1rhythm subediNo ratings yet
- DeforestationDocument27 pagesDeforestationRabi'atul Adawiyah Ismail100% (1)
- Introduction To RR SignalingDocument118 pagesIntroduction To RR SignalingPaulo100% (1)
- Textbook Philosophy For Life Teach Yourself The Ideas That Shape Our World and How To Use Them Mel Thompson Ebook All Chapter PDFDocument53 pagesTextbook Philosophy For Life Teach Yourself The Ideas That Shape Our World and How To Use Them Mel Thompson Ebook All Chapter PDFricky.fetterman649100% (8)
- Animal Breeding CourseDocument3 pagesAnimal Breeding CourselizardinluckNo ratings yet
- Assignment Society (T)Document5 pagesAssignment Society (T)Noor FatihahNo ratings yet
- Neet 2 PDFDocument23 pagesNeet 2 PDFchandru100% (1)
- Cable TrunkingDocument5 pagesCable TrunkingLeo GeeNo ratings yet
- MTB Grade 6 Clarinet: Select Two Pieces From The Following List (25 Marks Each)Document4 pagesMTB Grade 6 Clarinet: Select Two Pieces From The Following List (25 Marks Each)Δημήτρης ΑργυρόςNo ratings yet
- Project On Measuring The Solubility of A Saturated SolutionDocument9 pagesProject On Measuring The Solubility of A Saturated SolutionSaurabh SinghNo ratings yet
- Vedic Life Vs Modern LifeDocument5 pagesVedic Life Vs Modern LifeDILKHUSH KUMARNo ratings yet
- An Efficient Micropropagation Protocol For Eclipta AlbaDocument6 pagesAn Efficient Micropropagation Protocol For Eclipta AlbaSuprabuddha KunduNo ratings yet
- Ginni International Limited-1Document17 pagesGinni International Limited-1Charanpreet SinghNo ratings yet
- Is-11682.1985 (Staging For Overhead Water Tanks)Document27 pagesIs-11682.1985 (Staging For Overhead Water Tanks)amithcivil100% (2)
- Idustrial Q & ADocument6 pagesIdustrial Q & ARegie SalidagaNo ratings yet
- Biographical Sketch: As Nursing, Include Postdoctoral Training and Residency Training If Applicable.)Document4 pagesBiographical Sketch: As Nursing, Include Postdoctoral Training and Residency Training If Applicable.)dfgdfgdfgdfgdfgNo ratings yet
- Types of FabricDocument33 pagesTypes of FabricShabana Waqar100% (1)
- Ride - June 2018 UkDocument124 pagesRide - June 2018 UkDương TúNo ratings yet
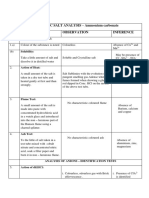
- INORGANIC SALT ANALYSIS - Ammonium Carbonate S.No Experiment Observation InferenceDocument24 pagesINORGANIC SALT ANALYSIS - Ammonium Carbonate S.No Experiment Observation InferenceRyoshiNo ratings yet
- Drugs For Bone MetabolismDocument15 pagesDrugs For Bone MetabolismkwennybiangNo ratings yet