You might also like
- Stanford CA-1 Tutorial Textbook 7-12-2022 FINALDocument108 pagesStanford CA-1 Tutorial Textbook 7-12-2022 FINALTudor Ghiara100% (3)
- Practice Guidelines For Central Venous Access 2020 An Updated Report by The American Society of Anesthesiologists Task Force On Central Venous Access PDFDocument36 pagesPractice Guidelines For Central Venous Access 2020 An Updated Report by The American Society of Anesthesiologists Task Force On Central Venous Access PDFDaniel Castro VeintimillaNo ratings yet
- The Pedicled TRAM Flap in Breast ReconstructionDocument22 pagesThe Pedicled TRAM Flap in Breast ReconstructionJose Mauricio Suarez BecerraNo ratings yet
- Anesthesia and Sedation Outside ofDocument9 pagesAnesthesia and Sedation Outside ofPutriRahayuMoidadyNo ratings yet
- Evaluation of A Radial Artery Cannulation Training Program For Intensive Care Nurses: A Descriptive, Explorative StudyDocument9 pagesEvaluation of A Radial Artery Cannulation Training Program For Intensive Care Nurses: A Descriptive, Explorative StudyAngelina PondeteNo ratings yet
- 2020 - Feasibility and Safety of Peripheral Intravenous Administration of Vasopressor Agents in Resource-Limited SettingsDocument7 pages2020 - Feasibility and Safety of Peripheral Intravenous Administration of Vasopressor Agents in Resource-Limited SettingsAndre OliveiraNo ratings yet
- Pal Ese 2011Document8 pagesPal Ese 2011retta tataNo ratings yet
- Safety and Effectiveness of Inferior Vena Cava Filters Used To Protect Against Pulmonary EmbolusDocument26 pagesSafety and Effectiveness of Inferior Vena Cava Filters Used To Protect Against Pulmonary EmbolusCalifornia Technology Assessment ForumNo ratings yet
- The Ann Arbor Criteria For Appropriate Urinary Catheter Use in Hospitalized Medical Patients: Results Obtained by Using The RAND/UCLA Appropriateness MethodDocument34 pagesThe Ann Arbor Criteria For Appropriate Urinary Catheter Use in Hospitalized Medical Patients: Results Obtained by Using The RAND/UCLA Appropriateness MethodCarissa SulaimanNo ratings yet
- The 2011 Infusion Nursing Standards of PracticeDocument12 pagesThe 2011 Infusion Nursing Standards of PracticeSugeng PrakosoNo ratings yet
- 1 s2.0 S2452247318300384 Main PDFDocument4 pages1 s2.0 S2452247318300384 Main PDFDinny ApriliaNo ratings yet
- Axillary Artery and Vein Cannulation 2015Document4 pagesAxillary Artery and Vein Cannulation 2015icen00bNo ratings yet
- Ins and Outs of Urinary Catheters: Indwelling Urethral Catheterisation (Short Term and Long Term)Document5 pagesIns and Outs of Urinary Catheters: Indwelling Urethral Catheterisation (Short Term and Long Term)Yudhi AuliaNo ratings yet
- Seldinger ModifiedseldingerDocument6 pagesSeldinger ModifiedseldingerThiago BañosNo ratings yet
- A Clinician's Perspective: KDOQI Vascular Access GuidelinesDocument2 pagesA Clinician's Perspective: KDOQI Vascular Access GuidelinestandiNo ratings yet
- Peripherally Inserted Central Venous Acces - 2021 - Seminars in Pediatric SurgerDocument8 pagesPeripherally Inserted Central Venous Acces - 2021 - Seminars in Pediatric Surgeralergo.ramirezNo ratings yet
- Device Selection: Nancy L. Moureau and Evan AlexandrouDocument19 pagesDevice Selection: Nancy L. Moureau and Evan AlexandrouCarmen T OrtizNo ratings yet
- Jurnal Uro 2Document8 pagesJurnal Uro 2Lisa HikmawanNo ratings yet
- Guidelines For Safety in The Gastrointestinal Endoscopy UnitDocument10 pagesGuidelines For Safety in The Gastrointestinal Endoscopy UnitDairotul KhasanahNo ratings yet
- CVC Acceso 2020Document36 pagesCVC Acceso 2020Jose David Flores PérezNo ratings yet
- About Time: Diagnostic Guidelines That Help CliniciansDocument5 pagesAbout Time: Diagnostic Guidelines That Help Cliniciansujangketul62No ratings yet
- The Michigan Appropriateness Guide For Intravenous Catheters (MAGIC) : Results From A Multispecialty Panel Using The RAND/UCLA Appropriateness MethodDocument48 pagesThe Michigan Appropriateness Guide For Intravenous Catheters (MAGIC) : Results From A Multispecialty Panel Using The RAND/UCLA Appropriateness Methodnanang criztaNo ratings yet
- Bona Witz 2012Document4 pagesBona Witz 2012Bahadır ÇAKIRNo ratings yet
- Temporary Inferior Vena Cava Filters: How Do We Move Forward?Document3 pagesTemporary Inferior Vena Cava Filters: How Do We Move Forward?MostafaNo ratings yet
- Implementation of The Modified Canadian C Spine Rule by ParamedicsDocument10 pagesImplementation of The Modified Canadian C Spine Rule by Paramedicscarper454No ratings yet
- Pocus Periferal Access Vs PiccDocument5 pagesPocus Periferal Access Vs Piccsalem.pvjNo ratings yet
- CVC AnesthesiaDocument36 pagesCVC AnesthesianadiaNo ratings yet
- Positive Effect of Care Bundles On Patients With Central Venous Catheter Insertions at A Tertiary Hospital in Beijing, ChinaDocument10 pagesPositive Effect of Care Bundles On Patients With Central Venous Catheter Insertions at A Tertiary Hospital in Beijing, ChinaElfina NataliaNo ratings yet
- Bmjopen 2014 007257Document7 pagesBmjopen 2014 007257rezzkNo ratings yet
- A Systematic Review of Extravasation and Local Tissue Injury FromDocument10 pagesA Systematic Review of Extravasation and Local Tissue Injury FromJustin AllisterNo ratings yet
- Controversiesin Microvascular Maxillofacial Reconstruction: Adam P. Fagin,, Daniel PetrisorDocument10 pagesControversiesin Microvascular Maxillofacial Reconstruction: Adam P. Fagin,, Daniel PetrisorSheetal HNo ratings yet
- The Use of A Spring-Loaded Silo For Gastroschisis: Impact On Practice Patterns and OutcomesDocument4 pagesThe Use of A Spring-Loaded Silo For Gastroschisis: Impact On Practice Patterns and OutcomesEnvhy WinaNo ratings yet
- 2014 - Guidelines For Safety in The Gastrointestinal Endoscopy Unit PDFDocument10 pages2014 - Guidelines For Safety in The Gastrointestinal Endoscopy Unit PDFBaim FarmaNo ratings yet
- External Jugular Vein Peripheral IntravenousDocument7 pagesExternal Jugular Vein Peripheral Intravenoushector nuñezNo ratings yet
- Bernstein 2004Document6 pagesBernstein 2004Diana PânteaNo ratings yet
- Cathet Cardio Intervent - 2005 - Chambers - Infection Control Guidelines For The Cardiac Catheterization LaboratoryDocument9 pagesCathet Cardio Intervent - 2005 - Chambers - Infection Control Guidelines For The Cardiac Catheterization Laboratorygadhang dewanggaNo ratings yet
- A Descriptive Study of Peripheral Intravenous Catheters in Patients... - Foster L Et Al - J Infusion Nursing - 2002Document9 pagesA Descriptive Study of Peripheral Intravenous Catheters in Patients... - Foster L Et Al - J Infusion Nursing - 2002pareshNo ratings yet
- 06 2010 Jun Central-Venous-CatheterDocument6 pages06 2010 Jun Central-Venous-CatheterFrancisco VigenorNo ratings yet
- 321971029397/virtualeducation/20122/anuncios/37790/CVC Femoral NEJM PDFDocument3 pages321971029397/virtualeducation/20122/anuncios/37790/CVC Femoral NEJM PDFvalentina cadena correaNo ratings yet
- Central Venous Catheter Insertion Checklist1Document1 pageCentral Venous Catheter Insertion Checklist1أركان هيلث Arkan healthNo ratings yet
- Protocolos Weaining 2011Document14 pagesProtocolos Weaining 2011perla islasNo ratings yet
- Ava Poster Cincinnati Childrens Hospital Medical CenterDocument1 pageAva Poster Cincinnati Childrens Hospital Medical Centeringrid.naruto.fbNo ratings yet
- Repair CDLDocument6 pagesRepair CDLYuliastuti Mamah ChelseaNo ratings yet
- Academic Emergency Medicine - July 1996 - Shoemaker - Noninvasive Hemodynamic Monitoring of Critical Patients in TheDocument9 pagesAcademic Emergency Medicine - July 1996 - Shoemaker - Noninvasive Hemodynamic Monitoring of Critical Patients in TheAndres Pimentel AlvarezNo ratings yet
- More Advantages of Trocar Compared Than Steel.55Document4 pagesMore Advantages of Trocar Compared Than Steel.55Yoan RahmahNo ratings yet
- Use of Short Peripheral Intravenous Catheters: Characteristics, Management, and Outcomes WorldwideDocument7 pagesUse of Short Peripheral Intravenous Catheters: Characteristics, Management, and Outcomes WorldwidemochkurniawanNo ratings yet
- Complications Critically: Rectal Tube IllDocument3 pagesComplications Critically: Rectal Tube IllSoulNo ratings yet
- 295 QsDocument3 pages295 Qsujangketul62No ratings yet
- Role of Ultrsonography in Detecting The Location of Tip of Percutaneous Central Venous Catheters in Neonates at Hi-Tech Medical College and Hospital, BhubaneswarDocument5 pagesRole of Ultrsonography in Detecting The Location of Tip of Percutaneous Central Venous Catheters in Neonates at Hi-Tech Medical College and Hospital, BhubaneswarInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 2009 Venous AccessDocument3 pages2009 Venous AccessDaniela MéndezNo ratings yet
- Fixation of The Short-Term Central Venous Catheter. A Comparison of Two TechniquesDocument11 pagesFixation of The Short-Term Central Venous Catheter. A Comparison of Two TechniquesJaime Augusto Quimbayo GuarnizoNo ratings yet
- Improving Patient Safety in Haemodialysis: Editorial CommentDocument3 pagesImproving Patient Safety in Haemodialysis: Editorial CommentNurul Maliki Rayun IttaqaNo ratings yet
- Rosier 2016Document18 pagesRosier 2016Habib G. Moutran BarrosoNo ratings yet
- Score Predicting The Need For Hospitalization in Scorpion EnvenomationDocument7 pagesScore Predicting The Need For Hospitalization in Scorpion EnvenomationWalaa YousefNo ratings yet
- A Survey of Ventilation Strategies During Cardiopulmonary ResuscitationDocument6 pagesA Survey of Ventilation Strategies During Cardiopulmonary ResuscitationGiseleNo ratings yet
- ENDODocument14 pagesENDOmichakishaNo ratings yet
- Prevalence of Phlebitis Among Patients Receiving Peripheral Intravenous Therapy in A Tertiary Care Hospital in IndiaDocument6 pagesPrevalence of Phlebitis Among Patients Receiving Peripheral Intravenous Therapy in A Tertiary Care Hospital in IndiaIJAR JOURNALNo ratings yet
- Percutaneous NephrosDocument17 pagesPercutaneous NephrosIan HuangNo ratings yet
- Catéter Central y USDocument11 pagesCatéter Central y USfabio1595No ratings yet
- Abstract No. 301 - Angiographic Catheters - A Comprehensive Review For The Interventionalist In-TrainingDocument2 pagesAbstract No. 301 - Angiographic Catheters - A Comprehensive Review For The Interventionalist In-TrainingPeter LiNo ratings yet
- Quality Improvement Guidelines For PercuDocument5 pagesQuality Improvement Guidelines For PercuSumpah Dokter Batch III 2022No ratings yet
- Epithelial Tissues MnemonicsDocument3 pagesEpithelial Tissues MnemonicsDaniel AyanlekeNo ratings yet
- Module or JAKEDocument10 pagesModule or JAKEJake Yvan DizonNo ratings yet
- Airway Management: Azzam Nawab Mbbs Aanawab@imamu - Edu.saDocument48 pagesAirway Management: Azzam Nawab Mbbs Aanawab@imamu - Edu.sasamhNo ratings yet
- Crown LengtheningDocument54 pagesCrown LengtheningMehdi MoshaveriNo ratings yet
- Anyridge: The 21St Century Premium Implant SystemDocument80 pagesAnyridge: The 21St Century Premium Implant Systemvaleriu vatamanNo ratings yet
- Definisi Transverse LieDocument5 pagesDefinisi Transverse LieErmi MarlinaNo ratings yet
- SUHNA Dental Manpower-1Document28 pagesSUHNA Dental Manpower-1Suhna MohammedNo ratings yet
- Treatment of Class III Malocclusions Using Temporary Anchorage Devices (TADs) The Alt RAMEC Protocol and Inermaxillary Class III Elastics in The Growing PatientDocument144 pagesTreatment of Class III Malocclusions Using Temporary Anchorage Devices (TADs) The Alt RAMEC Protocol and Inermaxillary Class III Elastics in The Growing PatientJulio Ugás ZapataNo ratings yet
- Perioperative Optimization of Patients With Neuromuscular Disorders Undergoing Scoliosis Corrective Surgery: A Multidisciplinary Team ApproachDocument9 pagesPerioperative Optimization of Patients With Neuromuscular Disorders Undergoing Scoliosis Corrective Surgery: A Multidisciplinary Team ApproachZvonkitza CertanecNo ratings yet
- Birth Canal Injuries Final LectureDocument63 pagesBirth Canal Injuries Final Lecturepeter njoguNo ratings yet
- MCN Review Guide QuestionsDocument16 pagesMCN Review Guide Questionspjpajarit1522 nunezNo ratings yet
- A Glossary of Anesthetic Jargon .8Document4 pagesA Glossary of Anesthetic Jargon .8TonyNo ratings yet
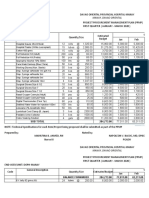
- PPMP Medical Supplies 2020Document16 pagesPPMP Medical Supplies 2020Jan Oneille Y. VallesNo ratings yet
- 2005 The Diary of An Orthognathic Patient Aged 30Â (Retrieved - 2023-06-05)Document6 pages2005 The Diary of An Orthognathic Patient Aged 30Â (Retrieved - 2023-06-05)Peter SerNo ratings yet
- Hypothyroidism and MyxedemaDocument2 pagesHypothyroidism and MyxedemaMajj MajjNo ratings yet
- Arco en C PhillipsDocument7 pagesArco en C PhillipsjuanNo ratings yet
- Modul Saccrum and CoxigeusDocument7 pagesModul Saccrum and Coxigeusmazidah fauziyyah24No ratings yet
- 23 4 2021Document3 pages23 4 2021izat husseinNo ratings yet
- Nasal Angiofibroma in A Female: A Rare Case Report: OtolaryngologyDocument2 pagesNasal Angiofibroma in A Female: A Rare Case Report: OtolaryngologyKhumaira SantaNo ratings yet
- RCH - Peds Emergency Reference Card - Jan 2013Document2 pagesRCH - Peds Emergency Reference Card - Jan 2013Bob YongNo ratings yet
- Nur 111 Session 11 Sas 1Document9 pagesNur 111 Session 11 Sas 1Zzimply Tri Sha UmaliNo ratings yet
- Aer 06 29Document4 pagesAer 06 29Vimal NishadNo ratings yet
- 2020 Medical GuidelinesDocument406 pages2020 Medical Guidelinesanitn2020No ratings yet
- Knots & Sutures Surgical SutureDocument29 pagesKnots & Sutures Surgical SutureAlexandra MacsimNo ratings yet
- Phlebolymphology: Vol 28 - No. 1 - 2021 - P1-36 No. 103Document39 pagesPhlebolymphology: Vol 28 - No. 1 - 2021 - P1-36 No. 103Jing CruzNo ratings yet
- Our Sacrospinous FixationDocument3 pagesOur Sacrospinous Fixationopi setiaNo ratings yet
- 978 1 5275 1795 0 SampleDocument30 pages978 1 5275 1795 0 SampleDANIEL SIMASIKUNo ratings yet
- балонный синусDocument5 pagesбалонный синусIrinaBorodulinaNo ratings yet