You might also like
- IB Chemistry Lab Report GuideDocument10 pagesIB Chemistry Lab Report GuidePriscilla SANGANo ratings yet
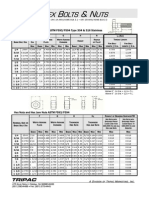
- Imperial Bolts Nuts & WashersDocument7 pagesImperial Bolts Nuts & WashersstugwynneNo ratings yet
- Epigenetics (Nilofer Saba Azad, M.D.)Document40 pagesEpigenetics (Nilofer Saba Azad, M.D.)National Press Foundation100% (2)
- Hagerman - Training The Energy SystemsDocument8 pagesHagerman - Training The Energy Systemsmkn1214100% (1)
- Basic Caculation in Chemotherapy (Risani)Document43 pagesBasic Caculation in Chemotherapy (Risani)Rizki Yulisetiawan100% (1)
- Albaflow JETDocument12 pagesAlbaflow JETTrinhTruong100% (1)
- Molecular Pathology of Breast CancerDocument42 pagesMolecular Pathology of Breast CancerleartaNo ratings yet
- Applied Eco - Q4 - M4Document12 pagesApplied Eco - Q4 - M4bernadette domoloan100% (2)
- Chemotherapy Plus Immunotherapy LungDocument46 pagesChemotherapy Plus Immunotherapy LungHemanth KumarNo ratings yet
- American J Hematol - 2023 - JoinerDocument4 pagesAmerican J Hematol - 2023 - Joinersalman mehriNo ratings yet
- Prostate Cancer Disease States: Castration-ResistantDocument59 pagesProstate Cancer Disease States: Castration-ResistantRohan BatraNo ratings yet
- Response Assessment in Neuro-OncologyDocument40 pagesResponse Assessment in Neuro-Oncologyimk_mithunNo ratings yet
- 2022 ESMO V AC Prostate Cancer Metastatic CRPC Standard Care RMDocument53 pages2022 ESMO V AC Prostate Cancer Metastatic CRPC Standard Care RMcatp38647No ratings yet
- Emergence of Immunotherapy As A Cancer Treatment - Feb 26 2018Document50 pagesEmergence of Immunotherapy As A Cancer Treatment - Feb 26 2018KaramSoftNo ratings yet
- CCO Hematology 2021 362Document12 pagesCCO Hematology 2021 362Tanya YankovaNo ratings yet
- Drug Interactions in Breast Cancer ChemotherapyDocument27 pagesDrug Interactions in Breast Cancer ChemotherapymayumikikiNo ratings yet
- 3625Document18 pages3625Camilo CaceresNo ratings yet
- Recurrent TonsilitisDocument16 pagesRecurrent TonsilitisAyen FornollesNo ratings yet
- Dr. Djohan Ardiansyah, SP.S (K)Document60 pagesDr. Djohan Ardiansyah, SP.S (K)satyagraha84No ratings yet
- Righ Choise TrialDocument17 pagesRigh Choise TrialOscar FloresNo ratings yet
- 7.4 - Targeted Therapy - Anti-Neoplastic Agents Dec2013-Dec2015-1Document14 pages7.4 - Targeted Therapy - Anti-Neoplastic Agents Dec2013-Dec2015-1Gabrielle NnomoNo ratings yet
- CNS Met From HER2+ BCDocument27 pagesCNS Met From HER2+ BChiroshima123No ratings yet
- Update On Evolving Therapies For Advanced Kidney CancerDocument72 pagesUpdate On Evolving Therapies For Advanced Kidney CancerBob MarchandNo ratings yet
- ESMO 2016 - Abstract 719ODocument17 pagesESMO 2016 - Abstract 719ODavid OlmosNo ratings yet
- Davis Symposium AdvancesInSarcomaDocument55 pagesDavis Symposium AdvancesInSarcomaFernando SilalahiNo ratings yet
- CCO Clinical Oncology 2021 4002Document13 pagesCCO Clinical Oncology 2021 4002veaceslav coscodanNo ratings yet
- Lo Coco FrancescoDocument61 pagesLo Coco FrancescoJess silvaNo ratings yet
- Armand Et Al. - 2013 - Detection of Circulating Tumour DNA in Patients With Aggressive B-Cell Non-Hodgkin Lymphoma PDFDocument4 pagesArmand Et Al. - 2013 - Detection of Circulating Tumour DNA in Patients With Aggressive B-Cell Non-Hodgkin Lymphoma PDFflashjetNo ratings yet
- Nitrogen-Containing Steroids As Potential Anticancer AgentsDocument31 pagesNitrogen-Containing Steroids As Potential Anticancer AgentsSamuelNo ratings yet
- Aml FLT3Document27 pagesAml FLT3Dea ReyesNo ratings yet
- Rtog 0813 Marina CousinsDocument22 pagesRtog 0813 Marina Cousinsapi-426094285No ratings yet
- CNS Control in Subgroup DESTINY Trial Oral PresentDocument19 pagesCNS Control in Subgroup DESTINY Trial Oral Presenthiroshima123No ratings yet
- Journal Reading Nasopharyngeal Carcinoma: Current Treatment Options and Future DirectionsDocument28 pagesJournal Reading Nasopharyngeal Carcinoma: Current Treatment Options and Future DirectionsyuliNo ratings yet
- Perioperative Medicine:: Management of Chronic SteroidsDocument20 pagesPerioperative Medicine:: Management of Chronic SteroidsGus LionsNo ratings yet
- Treatment Strategies and Current Therapeutic OptionsDocument32 pagesTreatment Strategies and Current Therapeutic OptionsFiricel PaulNo ratings yet
- Protocol Rtog 1119 1Document18 pagesProtocol Rtog 1119 1api-540888060No ratings yet
- University College of Medical Sciences - Delhi - QuotationDocument2 pagesUniversity College of Medical Sciences - Delhi - QuotationPunit MahapatraNo ratings yet
- 28 Research in Therapi MolecularDocument14 pages28 Research in Therapi MolecularherminNo ratings yet
- Thyroid New Treatment For Advanced Thyroid Cancer M Cabanillas 2021 05Document49 pagesThyroid New Treatment For Advanced Thyroid Cancer M Cabanillas 2021 05Marcos LVNo ratings yet
- 107.11.1 GlycopeptidePK - 20181101 - GIOCP - Case - Part2Document4 pages107.11.1 GlycopeptidePK - 20181101 - GIOCP - Case - Part2ft84nzzc92No ratings yet
- P200010S010BDocument33 pagesP200010S010Bmetech8xNo ratings yet
- Gaudy Marqueste2017Document11 pagesGaudy Marqueste2017Marco GornattiNo ratings yet
- Bi Omar CadresDocument33 pagesBi Omar CadresNataly Butrón BustamanteNo ratings yet
- The REGULATE-PCI Randomized Clinical TrialDocument26 pagesThe REGULATE-PCI Randomized Clinical TrialstacayNo ratings yet
- An Updated Analysis of The Survival Endpoints of Ascende-Rt: Clinical InvestigationDocument10 pagesAn Updated Analysis of The Survival Endpoints of Ascende-Rt: Clinical InvestigationfumadelabuenaNo ratings yet
- AdvancedDocument12 pagesAdvancedapi-675909478No ratings yet
- Trial: Tailorx: Trial Assigning Individualized Options For Treatment (RX)Document4 pagesTrial: Tailorx: Trial Assigning Individualized Options For Treatment (RX)Natalia QuinteroNo ratings yet
- Z Devd FMKDocument12 pagesZ Devd FMKAdnan FojnicaNo ratings yet
- Reproducible Quantification in PET - CT: Clinical Relevance and Technological ApproachesDocument28 pagesReproducible Quantification in PET - CT: Clinical Relevance and Technological ApproachesFandoNo ratings yet
- St. Gallen 2021Document41 pagesSt. Gallen 2021Alis PoonaNo ratings yet
- JC RapidoDocument30 pagesJC RapidoSudip ShakyaNo ratings yet
- ASH CaplacizumabDocument4 pagesASH CaplacizumabMagdalena Górska-KosickaNo ratings yet
- CCO Melanoma Clin Impact Slideset2Document27 pagesCCO Melanoma Clin Impact Slideset2Paola Yepez LugoNo ratings yet
- Original Article: High Expression of WDR1 in Primary Glioblastoma Is Associated With Poor PrognosisDocument12 pagesOriginal Article: High Expression of WDR1 in Primary Glioblastoma Is Associated With Poor PrognosisALINo ratings yet
- Dosimetric Evaluation of PlansDocument8 pagesDosimetric Evaluation of PlansQuang-Vu TranNo ratings yet
- Management of Status Epilepticus 2022Document8 pagesManagement of Status Epilepticus 2022albert siraitNo ratings yet
- IntroRDCM DrugDiscovery23 24Document55 pagesIntroRDCM DrugDiscovery23 24JoelSandovalNo ratings yet
- Curriculum Vitae: Lulus Handayani, MDDocument31 pagesCurriculum Vitae: Lulus Handayani, MDpisangphoeNo ratings yet
- Carole Mitnick EndtbDocument15 pagesCarole Mitnick Endtbeko kartiniNo ratings yet
- Role of Tipanat in MCRC and Gastroesophageal Junction Adenocarcinoma FinalDocument42 pagesRole of Tipanat in MCRC and Gastroesophageal Junction Adenocarcinoma FinalIndranil GhoshNo ratings yet
- Gregersen JeremyDocument27 pagesGregersen Jeremyapi-610233914No ratings yet
- Hamid 2018Document5 pagesHamid 2018AbulHasan Idrus IstarNo ratings yet
- ROICAM2015 Current Concept & Treatment of MMDocument66 pagesROICAM2015 Current Concept & Treatment of MMWilliamRayCassidyNo ratings yet
- UK Prostate Trials For 10th Uro-Onc Meeting 2013Document30 pagesUK Prostate Trials For 10th Uro-Onc Meeting 2013Prof_Nick_JamesNo ratings yet
- Q2 Mod6Document26 pagesQ2 Mod6Jermaine Francel TalampasNo ratings yet
- Livelihood Due To Establishment of Sitakunda Eco ParkDocument10 pagesLivelihood Due To Establishment of Sitakunda Eco ParkDr. Mohammad Shamsuddoha100% (1)
- Improvement of Voltage Profile Through The Optimal Placement of FACTS Using L-Index MethodDocument5 pagesImprovement of Voltage Profile Through The Optimal Placement of FACTS Using L-Index MethodRavishankar KankaleNo ratings yet
- Hotels: Discuss The Questions Below in A Small Group and Share Your Responses With The ClassDocument6 pagesHotels: Discuss The Questions Below in A Small Group and Share Your Responses With The ClassRoci roblesNo ratings yet
- Fly Ash Bricks and World Bank's CDM ProgramDocument21 pagesFly Ash Bricks and World Bank's CDM ProgramBhavesh KatariaNo ratings yet
- Ws c2960l 16ps LL DatasheetDocument5 pagesWs c2960l 16ps LL DatasheetjuanNo ratings yet
- Celiac Disease in ChildrenDocument59 pagesCeliac Disease in Childrend-fbuser-57045067No ratings yet
- Breaking Waves: A New Concept For Pile Supported Skirt BreakwatersDocument22 pagesBreaking Waves: A New Concept For Pile Supported Skirt BreakwaterspsuvarnasNo ratings yet
- A Remark On The Relationship Between Relativity Theory and Idealistic PhilosophDocument6 pagesA Remark On The Relationship Between Relativity Theory and Idealistic PhilosophAugast CorneliusNo ratings yet
- Anekal BOQDocument9 pagesAnekal BOQpavan3961No ratings yet
- 1555692-SB Daily Schedule Week 2Document3 pages1555692-SB Daily Schedule Week 2Niharika ChoudharyNo ratings yet
- Method Statement - Handover NotesDocument5 pagesMethod Statement - Handover NotesHamza NadeemNo ratings yet
- Idoc - Pub Ic4l2t1to8akeyDocument1 pageIdoc - Pub Ic4l2t1to8akeySantiago MadridNo ratings yet
- Lesson 2 Operation On Fractions (Addition and Subtraction) PDFDocument5 pagesLesson 2 Operation On Fractions (Addition and Subtraction) PDFMarie MargaretteNo ratings yet
- Eibl 1979Document57 pagesEibl 1979MarkNo ratings yet
- 2x16 BOGIE SPARE PARTSDocument7 pages2x16 BOGIE SPARE PARTSVignesh PrabhuNo ratings yet
- The Value of Scripture: ChaptersDocument15 pagesThe Value of Scripture: Chaptersakshay patriNo ratings yet
- Preparation Outline - ExercicesDocument5 pagesPreparation Outline - ExercicesTatianaLVNo ratings yet
- Modeling in Respiratory Movement Using Labview and SimulinkDocument27 pagesModeling in Respiratory Movement Using Labview and SimulinkNashitah AlwazNo ratings yet
- 1.1 Husqvarna Motorcycles Service TimesDocument4 pages1.1 Husqvarna Motorcycles Service TimesaaaaaNo ratings yet
- Aspen Spinal Cord InjuryDocument8 pagesAspen Spinal Cord InjuryLuis Javier CastroNo ratings yet
- ARTON-32F: Operational ManualDocument42 pagesARTON-32F: Operational ManualAbdalmohaimin SeifNo ratings yet
- Unit 2 (B) Rate of DemandDocument9 pagesUnit 2 (B) Rate of DemandAkshit GuptaNo ratings yet
- 9 Desember 2022 SRF22-0413 Volvo D16 SN036063 PDFDocument2 pages9 Desember 2022 SRF22-0413 Volvo D16 SN036063 PDFFajra Nada NadifaNo ratings yet
- Three-Dimensional Structure of A Supersonic Jet Impinging On An Inclined PlateDocument5 pagesThree-Dimensional Structure of A Supersonic Jet Impinging On An Inclined PlateShadaan KhanNo ratings yet