You might also like
- TMP 1 F64Document18 pagesTMP 1 F64FrontiersNo ratings yet
- Chaos in Ocular Aberration Dynamics of The Human Eye: Karen M. Hampson and Edward A. H. MallenDocument15 pagesChaos in Ocular Aberration Dynamics of The Human Eye: Karen M. Hampson and Edward A. H. MallenFrank smith Condor loarteNo ratings yet
- Millisecond Infrared Laser Pulses Depolarize and Elicit Action Potentials On In-Vitro Dorsal Root Ganglion NeuronsDocument11 pagesMillisecond Infrared Laser Pulses Depolarize and Elicit Action Potentials On In-Vitro Dorsal Root Ganglion Neuronsender000No ratings yet
- Imaging Cone Photoreceptors in Three Dimensions and in Time Using Ultrahigh Resolution Optical Coherence Tomography With Adaptive OpticsDocument16 pagesImaging Cone Photoreceptors in Three Dimensions and in Time Using Ultrahigh Resolution Optical Coherence Tomography With Adaptive OpticsChuanlin FanNo ratings yet
- Oe 21 3 3213Document12 pagesOe 21 3 3213Adarsh VishwakarmaNo ratings yet
- Quantifying Tissue Mechanical Properties Using PhotoplethysmographyDocument14 pagesQuantifying Tissue Mechanical Properties Using PhotoplethysmographyCalm YourselfNo ratings yet
- BOE Puszka CorrectedDocument15 pagesBOE Puszka CorrectedEsraa AymanNo ratings yet
- Electrifying Catheters With LightDocument16 pagesElectrifying Catheters With LightasifnewazuccNo ratings yet
- SHG THGDocument16 pagesSHG THGZeynep Nilüfer Güven ÖztürkNo ratings yet
- Field-Portable Reflection and Transmission Microscopy Based On Lensless HolographyDocument10 pagesField-Portable Reflection and Transmission Microscopy Based On Lensless HolographyShiva GaddamNo ratings yet
- Neuro ImagingDocument48 pagesNeuro ImagingSeiska MegaNo ratings yet
- Oe 16 009884Document11 pagesOe 16 009884benetorio.tNo ratings yet
- 2012 BOE v3 n8 p1774 LiewDocument13 pages2012 BOE v3 n8 p1774 LiewYih Miin LiewNo ratings yet
- UT Dallas Syllabus For hcs6310.001.07s Taught by Emily Tobey (Etobey)Document5 pagesUT Dallas Syllabus For hcs6310.001.07s Taught by Emily Tobey (Etobey)UT Dallas Provost's Technology GroupNo ratings yet
- Integration of Optical Components On-Chip For Scattering and Fluorescence Detection in An Optofluidic DeviceDocument10 pagesIntegration of Optical Components On-Chip For Scattering and Fluorescence Detection in An Optofluidic DeviceDaniel MăriuțaNo ratings yet
- Selyem - Holographically Controlled Three-Dimensional Atomic Population PatternsDocument10 pagesSelyem - Holographically Controlled Three-Dimensional Atomic Population PatternsJos JedanNo ratings yet
- Optics 35Document9 pagesOptics 35z.umul9031No ratings yet
- TMP 34 FDDocument17 pagesTMP 34 FDFrontiersNo ratings yet
- Three-Dimensional-Printed Gas Dynamic Virtual Nozzles For X-Ray Laser Sample DeliveryDocument16 pagesThree-Dimensional-Printed Gas Dynamic Virtual Nozzles For X-Ray Laser Sample DeliverykhaleelkhamjanNo ratings yet
- Boe 7 9 3355Document22 pagesBoe 7 9 3355api-310329774No ratings yet
- Oe 13 23 9361Document13 pagesOe 13 23 9361Aggelos StefopoulosNo ratings yet
- On-Chip Generation of Time-And Wavelength-Division Multiplexed Multiple Time-Bin EntanglementDocument10 pagesOn-Chip Generation of Time-And Wavelength-Division Multiplexed Multiple Time-Bin EntanglementBukhariNo ratings yet
- Application of Physics in MedicineDocument9 pagesApplication of Physics in MedicineShreyash PolNo ratings yet
- Stanislas Dehaene Le Code La Conscience PDF 5Document21 pagesStanislas Dehaene Le Code La Conscience PDF 5geroimoNo ratings yet
- Observation of Live Chromatin Dynamics in Cells Via 3D Localization Microscopy Using Tetrapod Point Spread FunctionsDocument14 pagesObservation of Live Chromatin Dynamics in Cells Via 3D Localization Microscopy Using Tetrapod Point Spread FunctionsnimasolhjooNo ratings yet
- Dynamic Three-Dimensional Tracking of Single Fluorescent Nanoparticles Deep Inside Living TissueDocument11 pagesDynamic Three-Dimensional Tracking of Single Fluorescent Nanoparticles Deep Inside Living TissueRicardo AlvaradoNo ratings yet
- ITISRefernces V4Document15 pagesITISRefernces V4PATI�O BERNAL MARLONNo ratings yet
- FNIRS2018 AbstractDocument312 pagesFNIRS2018 AbstractJn5omEghSU0j0FNo ratings yet
- Smartphone Instrument For Portable Enzyme-Linked Immunosorbent AssaysDocument15 pagesSmartphone Instrument For Portable Enzyme-Linked Immunosorbent AssaysHarry YucraNo ratings yet
- Azucena 2010Document12 pagesAzucena 2010mahmoud khedrNo ratings yet
- Human Brain ProjectDocument9 pagesHuman Brain ProjectAndre L'HuillierNo ratings yet
- FlemingDocument14 pagesFlemingJames XueNo ratings yet
- Motion Integration Postdiction Visual Awareness Eagleman 2000Document4 pagesMotion Integration Postdiction Visual Awareness Eagleman 2000Francis CrimminsNo ratings yet
- Microphotography - A ReviewDocument3 pagesMicrophotography - A ReviewIJAR JOURNALNo ratings yet
- Barber y Brown 1984Document564 pagesBarber y Brown 1984Carlos Daniel AliagaNo ratings yet
- Determining The Optical Properties of Gelatine GelDocument17 pagesDetermining The Optical Properties of Gelatine GelCorynaNo ratings yet
- Frequency-Modulated Continuous-Wave Lidar Compressive Depth-MappingDocument16 pagesFrequency-Modulated Continuous-Wave Lidar Compressive Depth-Mappingflv_91No ratings yet
- Biomedical Engineering 2: Recent Developments: Proceedings of the Second Southern Biomedical Engineering ConferenceFrom EverandBiomedical Engineering 2: Recent Developments: Proceedings of the Second Southern Biomedical Engineering ConferenceC. William HallNo ratings yet
- Fluorescence Microscopy: Super-Resolution and other Novel TechniquesFrom EverandFluorescence Microscopy: Super-Resolution and other Novel TechniquesAnda CorneaNo ratings yet
- Oe 12 21 5178Document13 pagesOe 12 21 5178Fauzan AdamNo ratings yet
- Three-Dimensional Optical Memory Using A Human FingernailDocument8 pagesThree-Dimensional Optical Memory Using A Human FingernailPuja srinija AtukuriNo ratings yet
- Tissue Optics and Photonics: Biological Tissue StructuresDocument19 pagesTissue Optics and Photonics: Biological Tissue StructuresAnonymous efLc7hSit5No ratings yet
- Biophoton Papers PDFDocument5 pagesBiophoton Papers PDFBrightchip TechnologiesNo ratings yet
- Projects - 2023Document5 pagesProjects - 2023Gary Thomas JobNo ratings yet
- Raman PaperDocument7 pagesRaman PaperShamim khanNo ratings yet
- Isinya Tidak DibacaDocument6 pagesIsinya Tidak DibacaFajar Rudy QimindraNo ratings yet
- Clinical Aspects of Sensory Motor IntegrationDocument350 pagesClinical Aspects of Sensory Motor IntegrationAlexandra AiftimieNo ratings yet
- Using Noninvasive Multi-Harmonic Generation Microscopy: in Vivo Developmental Biology StudyDocument7 pagesUsing Noninvasive Multi-Harmonic Generation Microscopy: in Vivo Developmental Biology StudyMinces JewelsNo ratings yet
- Ultrasound: Its Applications in Medicine and BiologyFrom EverandUltrasound: Its Applications in Medicine and BiologyNo ratings yet
- 2007 - Heifetz Et Al. - Subdiffraction Optical Resolution of A Gold Nanosphere Located Within The Nanojet of A Mie-Resonant Dielectric MDocument9 pages2007 - Heifetz Et Al. - Subdiffraction Optical Resolution of A Gold Nanosphere Located Within The Nanojet of A Mie-Resonant Dielectric MClaudio BiaginiNo ratings yet
- Referensi: Palsi SerebralDocument10 pagesReferensi: Palsi SerebralRully Aditya WardhanaNo ratings yet
- Ex-Vivo Characterization of Human Colon Cancer: by Mueller Polarimetric ImagingDocument12 pagesEx-Vivo Characterization of Human Colon Cancer: by Mueller Polarimetric ImagingnuralitarpNo ratings yet
- Electromyography in CNS Disorders: Central EMGFrom EverandElectromyography in CNS Disorders: Central EMGBhagwan T. ShahaniNo ratings yet
- Data Acquisition and Processing: In Biology and MedicineFrom EverandData Acquisition and Processing: In Biology and MedicineKurt EnsleinNo ratings yet
- Noninvasive Glucose Monitoring Using Midinfrared Absorption Spectroscopy Based OnDocument14 pagesNoninvasive Glucose Monitoring Using Midinfrared Absorption Spectroscopy Based OnLevente BalázsNo ratings yet
- Applications in Clinical and Biomedical Research. Technical University of DenmarkDocument2 pagesApplications in Clinical and Biomedical Research. Technical University of DenmarkMIRANDARISKINo ratings yet
- Fabricating Micro-Bragg Reflectors in 3-D Photorefractive WaveguidesDocument6 pagesFabricating Micro-Bragg Reflectors in 3-D Photorefractive Waveguidesz.umul9031No ratings yet
- Non Linearly Induced Self Waveguiding Structure in Dye Doped Nematic Liquid Crystals Confined in CapillariesDocument8 pagesNon Linearly Induced Self Waveguiding Structure in Dye Doped Nematic Liquid Crystals Confined in Capillariesz.umul9031No ratings yet
- Holographic Recording in Specially Doped Lithium Niobate CrystalsDocument12 pagesHolographic Recording in Specially Doped Lithium Niobate Crystalsz.umul9031No ratings yet
- Optics 36Document6 pagesOptics 36z.umul9031No ratings yet
- Optics 39Document14 pagesOptics 39z.umul9031No ratings yet
- Speckle Photography Using Optically Addressed Multiple Quantum Well Spatial Light ModulatorsDocument5 pagesSpeckle Photography Using Optically Addressed Multiple Quantum Well Spatial Light Modulatorsz.umul9031No ratings yet
- Low-Threshold Laser Oscillation Due To Group-Velocity Anomaly Peculiar To Two-And Three-Dimensional Photonic CrystalsDocument9 pagesLow-Threshold Laser Oscillation Due To Group-Velocity Anomaly Peculiar To Two-And Three-Dimensional Photonic Crystalsz.umul9031No ratings yet
- Three-Dimensional Field Structure in Open Unstable Resonators Part I: Passive Cavity ResultsDocument12 pagesThree-Dimensional Field Structure in Open Unstable Resonators Part I: Passive Cavity Resultsz.umul9031No ratings yet
- Transient Dynamics During Two-Wave Mixing in Photorefractive Quantum Well Diodes Using Moving GratingsDocument7 pagesTransient Dynamics During Two-Wave Mixing in Photorefractive Quantum Well Diodes Using Moving Gratingsz.umul9031No ratings yet
- Analysis and Design of Arrayed Waveguide Gratings With MMI CouplersDocument11 pagesAnalysis and Design of Arrayed Waveguide Gratings With MMI Couplersz.umul9031No ratings yet
- Diffraction of A Transverse Electric (Te) : X-Wave by Conducting ObjectsDocument32 pagesDiffraction of A Transverse Electric (Te) : X-Wave by Conducting Objectsz.umul9031No ratings yet
- Optics PaperDocument6 pagesOptics Paperz.umul9031No ratings yet
- Optics 35Document9 pagesOptics 35z.umul9031No ratings yet
- Modified Diffraction Theory of Kirchhoff: Yusuf Z. UmulDocument11 pagesModified Diffraction Theory of Kirchhoff: Yusuf Z. Umulz.umul9031No ratings yet
- Longitudinal Fiber Parameter Measurements of Multi-Core Fiber Using OTDRDocument11 pagesLongitudinal Fiber Parameter Measurements of Multi-Core Fiber Using OTDRz.umul9031No ratings yet
- Thermally Induced Mode Loss Evolution in The Coiled Ytterbium Doped Large Mode Area FiberDocument14 pagesThermally Induced Mode Loss Evolution in The Coiled Ytterbium Doped Large Mode Area Fiberz.umul9031No ratings yet
- Electrically Optofluidic Zoom System With A Large Zoom Range and High-Resolution ImageDocument12 pagesElectrically Optofluidic Zoom System With A Large Zoom Range and High-Resolution Imagez.umul9031No ratings yet
- Coupling of Spatially Partially Coherent Beams Into Planar WaveguidesDocument15 pagesCoupling of Spatially Partially Coherent Beams Into Planar Waveguidesz.umul9031No ratings yet
- Optik 20-2-1617Document12 pagesOptik 20-2-1617z.umul9031No ratings yet
- Four-Wave Mixing Stability in Hybrid Photonic Crystal Fibers With Two Zero-Dispersion WavelengthsDocument15 pagesFour-Wave Mixing Stability in Hybrid Photonic Crystal Fibers With Two Zero-Dispersion Wavelengthsz.umul9031No ratings yet
- Theory of Carrier Depletion and Light Amplification in Active Slow Light Photonic Crystal WaveguidesDocument9 pagesTheory of Carrier Depletion and Light Amplification in Active Slow Light Photonic Crystal Waveguidesz.umul9031No ratings yet
- High Power Ultra-Widely Tuneable Femtosecond Pulses From A Non-Collinear Optical Parametric Oscillator (NOPO)Document6 pagesHigh Power Ultra-Widely Tuneable Femtosecond Pulses From A Non-Collinear Optical Parametric Oscillator (NOPO)z.umul9031No ratings yet
- Graphene-Based Polymer Waveguide Polarizer: Jin Tae Kim and Choon-Gi ChoiDocument7 pagesGraphene-Based Polymer Waveguide Polarizer: Jin Tae Kim and Choon-Gi Choiz.umul9031No ratings yet
- Non-Linear Optoelectronic Phase-Locked Loop For Stabilization of Opto-Millimeter Waves: Towards A Narrow Linewidth Tunable THZ SourceDocument7 pagesNon-Linear Optoelectronic Phase-Locked Loop For Stabilization of Opto-Millimeter Waves: Towards A Narrow Linewidth Tunable THZ Sourcez.umul9031No ratings yet
- Oblique Incidence and Polarization Effects in Coupled GratingsDocument7 pagesOblique Incidence and Polarization Effects in Coupled Gratingsz.umul9031No ratings yet
- Terahertz Photoconductive Antenna With Metal Nanoislands: Sang-Gil Park, Yongje Choi, Young-Jae Oh, and Ki-Hun JeongDocument6 pagesTerahertz Photoconductive Antenna With Metal Nanoislands: Sang-Gil Park, Yongje Choi, Young-Jae Oh, and Ki-Hun Jeongz.umul9031No ratings yet
- Catalogo Aesculap PDFDocument16 pagesCatalogo Aesculap PDFHansNo ratings yet
- The Broadband ForumDocument21 pagesThe Broadband ForumAnouar AleyaNo ratings yet
- Presentation On 4G TechnologyDocument23 pagesPresentation On 4G TechnologyFresh EpicNo ratings yet
- D 6000Document6 pagesD 6000os_ja@hotmail.comNo ratings yet
- 300 PSI CTS (MP-1115) Operation Manual Rev1.3Document18 pages300 PSI CTS (MP-1115) Operation Manual Rev1.3Juan Manuel VizosoNo ratings yet
- Module-4 (PDFDrive)Document67 pagesModule-4 (PDFDrive)Divya priya KNo ratings yet
- Niir Integrated Organic Farming Handbook PDFDocument13 pagesNiir Integrated Organic Farming Handbook PDFNatalieNo ratings yet
- EXP4 The Diels Alder ReactionsDocument3 pagesEXP4 The Diels Alder ReactionsLaura GuidoNo ratings yet
- Lesson Plan in Science 9: I. ObjectivesDocument8 pagesLesson Plan in Science 9: I. ObjectivesmarichuNo ratings yet
- LG250CDocument2 pagesLG250CCarlosNo ratings yet
- Piriformis Syndrome: Hardi Adiyatma, Shahdevi Nandar KusumaDocument6 pagesPiriformis Syndrome: Hardi Adiyatma, Shahdevi Nandar Kusumaismael wandikboNo ratings yet
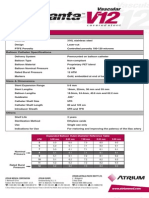
- Advanta V12 Data SheetDocument2 pagesAdvanta V12 Data SheetJuliana MiyagiNo ratings yet
- 12 Key Principles On Bhava AnalysisDocument28 pages12 Key Principles On Bhava AnalysisDhineshNo ratings yet
- Cisco 2500 Series RoutersDocument16 pagesCisco 2500 Series RoutersJull Quintero DazaNo ratings yet
- 18 Ray Optics Revision Notes QuizrrDocument108 pages18 Ray Optics Revision Notes Quizrraafaf.sdfddfaNo ratings yet
- Elements of Romanticism in The Poetry of W. B. Yeats: Romantic InfluencesDocument8 pagesElements of Romanticism in The Poetry of W. B. Yeats: Romantic InfluencesSadman Shaid SaadNo ratings yet
- Shree New Price List 2016-17Document13 pagesShree New Price List 2016-17ontimeNo ratings yet
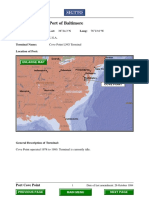
- Port Name: Port of BaltimoreDocument17 pagesPort Name: Port of Baltimoremohd1khairul1anuarNo ratings yet
- Course Registration SlipDocument2 pagesCourse Registration SlipMics EntertainmentNo ratings yet
- Fully Automatic Coffee Machine - Slimissimo - IB - SCOTT UK - 2019Document20 pagesFully Automatic Coffee Machine - Slimissimo - IB - SCOTT UK - 2019lazareviciNo ratings yet
- Runyankore-Rukiga Dictionary Launch: President Yoweri Museveni's SpeechDocument28 pagesRunyankore-Rukiga Dictionary Launch: President Yoweri Museveni's SpeechThe New Vision50% (2)
- Why Are Solids Are Floating On My Secondary Clarifier - Biological Waste TreatmDocument6 pagesWhy Are Solids Are Floating On My Secondary Clarifier - Biological Waste TreatmIsaac FernándezNo ratings yet
- Eng DS Epp-2314 1410Document2 pagesEng DS Epp-2314 1410MarkusAldoMaquNo ratings yet
- 5G Transport Slice Control in End-To-End 5G NetworksDocument19 pages5G Transport Slice Control in End-To-End 5G NetworksmorganNo ratings yet
- Manual PipsDocument5 pagesManual PipsOzzyNo ratings yet
- JC Series Jaw Crusher PDFDocument8 pagesJC Series Jaw Crusher PDFgarrybieber100% (1)
- Logic NotesDocument19 pagesLogic NotesCielo PulmaNo ratings yet
- Bomba MixerDocument2 pagesBomba MixerBinelli79No ratings yet
- Electric ScootorDocument40 pagesElectric Scootor01fe19bme079No ratings yet
- Esteem 1999 2000 1.3L 1.6LDocument45 pagesEsteem 1999 2000 1.3L 1.6LArnold Hernández CarvajalNo ratings yet