You might also like
- Diminished Ovarian Reserve and Assisted Reproductive Technologies: Current Research and Clinical ManagementFrom EverandDiminished Ovarian Reserve and Assisted Reproductive Technologies: Current Research and Clinical ManagementOrhan BukulmezNo ratings yet
- Testing and Interpreting Measures of Ovarian Reserve A Committee 2015Document9 pagesTesting and Interpreting Measures of Ovarian Reserve A Committee 2015Ina BanacuNo ratings yet
- Cancer Treatment and the Ovary: Clinical and Laboratory Analysis of Ovarian ToxicityFrom EverandCancer Treatment and the Ovary: Clinical and Laboratory Analysis of Ovarian ToxicityNo ratings yet
- Age-Related Normograms of Antimullerian Hormone Level in Healthy Repoductive Woman A Single Center StudyDocument12 pagesAge-Related Normograms of Antimullerian Hormone Level in Healthy Repoductive Woman A Single Center StudyRosdi AbdullahNo ratings yet
- Ovulation Induction and Controlled Ovarian Stimulation: A Practical GuideFrom EverandOvulation Induction and Controlled Ovarian Stimulation: A Practical GuideNo ratings yet
- Amh 2015Document15 pagesAmh 2015Jessica Leguia LeguiaNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 9: GynecologyFrom EverandComplementary and Alternative Medical Lab Testing Part 9: GynecologyNo ratings yet
- Testing and Interpreting Measures of Ovarian Reserve-NoprintDocument9 pagesTesting and Interpreting Measures of Ovarian Reserve-NoprintVioleta OrsettiNo ratings yet
- Co618 Ovarian Reserve YestingDocument6 pagesCo618 Ovarian Reserve YestingernestosandNo ratings yet
- The Use of Hormonal Contraceptives in Fertility Treatments - A Committee OpinionDocument7 pagesThe Use of Hormonal Contraceptives in Fertility Treatments - A Committee Opinionjorge nnNo ratings yet
- The Use of Antimullerian Hormone in Women Not Seeking Fertility CareDocument5 pagesThe Use of Antimullerian Hormone in Women Not Seeking Fertility CareLaura RojasNo ratings yet
- Dor 1Document10 pagesDor 1Alce Alce EverdienNo ratings yet
- Hormone TestingDocument6 pagesHormone TestingAgung IstiawanNo ratings yet
- A:ACEP 疗法Dr.SherDocument6 pagesA:ACEP 疗法Dr.Shermeltwithsnow163.comNo ratings yet
- Embarazo EctopicoDocument10 pagesEmbarazo EctopicocfsaludNo ratings yet
- Jbra1117 PDFDocument4 pagesJbra1117 PDFAgusNo ratings yet
- Lukaszuk Et Al. - 2014 - Anti-Müllerian Hormone (AMH) Is A Strong Predictor of Live Birth in Women Undergoing Assisted Reproductive TDocument6 pagesLukaszuk Et Al. - 2014 - Anti-Müllerian Hormone (AMH) Is A Strong Predictor of Live Birth in Women Undergoing Assisted Reproductive TKrzysztof ŁukaszukNo ratings yet
- Dor 2Document10 pagesDor 2Alce Alce EverdienNo ratings yet
- 1 s2.0 S0140673610603558 MainDocument11 pages1 s2.0 S0140673610603558 MainDr. Eser AĞARNo ratings yet
- PIIS0015028222000644Document7 pagesPIIS0015028222000644gayathri maranNo ratings yet
- Anti-Mu Llerian Hormone: Ovarian Reserve Testing and Its Potential Clinical ImplicationsDocument14 pagesAnti-Mu Llerian Hormone: Ovarian Reserve Testing and Its Potential Clinical ImplicationsSri IriantiNo ratings yet
- Fertility PreservationDocument9 pagesFertility PreservationAnizkha MitternachtNo ratings yet
- Efecto de La Salpingectomia en La Funcion OvaricaDocument16 pagesEfecto de La Salpingectomia en La Funcion OvaricaHermus Espiritu MaturranoNo ratings yet
- (2016) Infertile Women Below The Age of 40 Have Similar Anti-Müllerian Hormone Levels and Antral Follicle Count Compared With Women of The Same Age With No History of InfertilityDocument12 pages(2016) Infertile Women Below The Age of 40 Have Similar Anti-Müllerian Hormone Levels and Antral Follicle Count Compared With Women of The Same Age With No History of Infertility7dc2s9tdrwNo ratings yet
- Amenorrhea - An Approach To Diagnosis and Management AFP 2013 PDFDocument8 pagesAmenorrhea - An Approach To Diagnosis and Management AFP 2013 PDFBabila CarvalhoNo ratings yet
- PCOSDocument9 pagesPCOSirmaNo ratings yet
- DHEA Final PresentationDocument140 pagesDHEA Final PresentationSundar Narayanan100% (1)
- Fendo 11 536100Document8 pagesFendo 11 536100Maged BedeawyNo ratings yet
- Acog Practice Bulletin: Antepartum Fetal SurveillanceDocument12 pagesAcog Practice Bulletin: Antepartum Fetal SurveillanceMariana Hernandez100% (10)
- Modul Pelatihan Inseminasi Intra UterinDocument47 pagesModul Pelatihan Inseminasi Intra UterindrnyolNo ratings yet
- Effects of Anti M Llerian Hormone and Follicle Sti - 2014 - Taiwanese Journal ofDocument4 pagesEffects of Anti M Llerian Hormone and Follicle Sti - 2014 - Taiwanese Journal ofSami KahtaniNo ratings yet
- A1zsu Ovarian Stimulation Protocols PDFDocument152 pagesA1zsu Ovarian Stimulation Protocols PDFAnca Negreanu100% (2)
- OB/Gyn Clinical PearlsDocument4 pagesOB/Gyn Clinical PearlsD50% (4)
- The Use of Aromatase Inhibitors in Infertility and GynecologyDocument9 pagesThe Use of Aromatase Inhibitors in Infertility and Gynecologyalan lowusNo ratings yet
- Relevance of Pharmacogeomics in Ovarian Stimulation: A ReviewDocument9 pagesRelevance of Pharmacogeomics in Ovarian Stimulation: A ReviewIJAR JOURNALNo ratings yet
- Adolescent Gynecologic Care QUESTIONS 1, 2, 3Document7 pagesAdolescent Gynecologic Care QUESTIONS 1, 2, 3patelkn_2005No ratings yet
- Prevalence of Congenital Malformation Among Neonates Born After The Use of Progesterone For Luteal Support During IVF and ICSI CyclesDocument7 pagesPrevalence of Congenital Malformation Among Neonates Born After The Use of Progesterone For Luteal Support During IVF and ICSI Cycleseditorial.boardNo ratings yet
- The Use of Aromatase Inhibitors in in Vitro Fertilization: Juan A. Garcia-Velasco, M.DDocument3 pagesThe Use of Aromatase Inhibitors in in Vitro Fertilization: Juan A. Garcia-Velasco, M.Dtipu42No ratings yet
- JurnalDocument6 pagesJurnalWidya Rachmania PutriNo ratings yet
- Jurnal English PCOSDocument12 pagesJurnal English PCOSAbdurrachman MachfudzNo ratings yet
- Fendo 12 801026Document10 pagesFendo 12 801026Shilpa DuttaNo ratings yet
- 10.1007@s00404 018 4680 1Document12 pages10.1007@s00404 018 4680 1Eva OretlaNo ratings yet
- Diagnostic InfertilDocument14 pagesDiagnostic InfertilMagister KebidananNo ratings yet
- Progestogens in Obstetrics and Gynecology 2015th Edition (PRG)Document213 pagesProgestogens in Obstetrics and Gynecology 2015th Edition (PRG)amenu_bizuneh100% (4)
- Piis0015028211013112 PDFDocument2 pagesPiis0015028211013112 PDFGayathriMaranNo ratings yet
- Mild Ovarian Stimulation For IVFDocument17 pagesMild Ovarian Stimulation For IVFanyka2No ratings yet
- Smith - Diagnosis and Management of Female InfertilityDocument4 pagesSmith - Diagnosis and Management of Female InfertilityAmanda SaphiraNo ratings yet
- Polycystic Ovary Syndrome 2016 NEJMDocument11 pagesPolycystic Ovary Syndrome 2016 NEJMGabrielaNo ratings yet
- Management of Infertility: Clinical ReviewDocument4 pagesManagement of Infertility: Clinical ReviewHartanto LieNo ratings yet
- The Use of Acupuncture With in Vitro Fertilization: Is There A Point?Document10 pagesThe Use of Acupuncture With in Vitro Fertilization: Is There A Point?lu salviaNo ratings yet
- Case Presentation Obstetrics & Gynecology Rumc: Attending: Dr. ShatsDocument14 pagesCase Presentation Obstetrics & Gynecology Rumc: Attending: Dr. ShatsNirmita J PatelNo ratings yet
- Aromatase Inhibitors For Ovulation Induction and Ovarian StimulationDocument13 pagesAromatase Inhibitors For Ovulation Induction and Ovarian StimulationGinecologia Aseptică 1No ratings yet
- 1 s2.0 S1110569013000022 MainDocument5 pages1 s2.0 S1110569013000022 MainAripinSyarifudinNo ratings yet
- 5f33a63892ff020200812article - PDF - FileStep-up Protocol Versus Conventional Dosage of Letrozole For Ovulation Induction in Women With PCOSDocument4 pages5f33a63892ff020200812article - PDF - FileStep-up Protocol Versus Conventional Dosage of Letrozole For Ovulation Induction in Women With PCOSAhmed AnwarNo ratings yet
- HyfvDocument5 pagesHyfvAgusNo ratings yet
- Diagnosis and Treatment of Unexplained InfertilityDocument8 pagesDiagnosis and Treatment of Unexplained InfertilityudjkwNo ratings yet
- Low Antimullerian Hormone Levels Improve Fertility Outcome in Patients With Polycystic Ovary Syndrome 1665Document5 pagesLow Antimullerian Hormone Levels Improve Fertility Outcome in Patients With Polycystic Ovary Syndrome 1665GayathriMaranNo ratings yet
- PIIS0015028219324847Document18 pagesPIIS0015028219324847Maged BedeawyNo ratings yet
- Laparoscopic ClomipenDocument5 pagesLaparoscopic ClomipenHar YudhaNo ratings yet
- Efficacy of Progestogens in The Maintenance of Early Pregnancy in Women With Threatened Miscarriage or Recurrent MiscarriageDocument20 pagesEfficacy of Progestogens in The Maintenance of Early Pregnancy in Women With Threatened Miscarriage or Recurrent MiscarriagesilviuNo ratings yet
- Physiology of Amniotic Fluid Volume RegulationDocument8 pagesPhysiology of Amniotic Fluid Volume RegulationYosep SutandarNo ratings yet
- Meta-Analysis of Second-Trimester Markers For Trisomy 21. 2013Document15 pagesMeta-Analysis of Second-Trimester Markers For Trisomy 21. 2013risos7No ratings yet
- Maxillary Gap at 11-13 WeeksDocument5 pagesMaxillary Gap at 11-13 Weekscarlos cobeloNo ratings yet
- Uog 10054Document22 pagesUog 10054Aswin ChristantoNo ratings yet
- IETADocument10 pagesIETAJose Luis Morales BautistaNo ratings yet
- PIIS000293781502102XDocument1 pagePIIS000293781502102XYosep SutandarNo ratings yet
- Routine Firsttrimester Ultrasound Screening Using A Standardized Anatomical ProtocolDocument15 pagesRoutine Firsttrimester Ultrasound Screening Using A Standardized Anatomical ProtocolYosep SutandarNo ratings yet
- Musa 2015Document15 pagesMusa 2015Jose Luis Morales BautistaNo ratings yet
- Clostridium Perfringens Sepsis Following A Molar Pregnancy: ASE EportDocument2 pagesClostridium Perfringens Sepsis Following A Molar Pregnancy: ASE EportYosep SutandarNo ratings yet
- PIIS0015028207001161Document8 pagesPIIS0015028207001161Yosep SutandarNo ratings yet
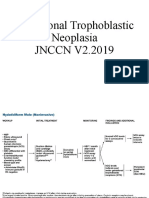
- Gestational Trophoblastic NeoplasiaDocument14 pagesGestational Trophoblastic NeoplasiaYosep SutandarNo ratings yet
- ISUOG - Fetal Heart ExaminationDocument12 pagesISUOG - Fetal Heart ExaminationAzucenaNo ratings yet
- Diagnosis of Fetal Non-Chromosomal Abnormalities On Routine Ultrasound Examination at 11-13 Weeks' GestationDocument10 pagesDiagnosis of Fetal Non-Chromosomal Abnormalities On Routine Ultrasound Examination at 11-13 Weeks' GestationYosep SutandarNo ratings yet
- Pi Is 0002937817310955Document11 pagesPi Is 0002937817310955Yosep SutandarNo ratings yet
- Ferra RettiDocument51 pagesFerra RettiYosep SutandarNo ratings yet
- PDFDocument9 pagesPDFYosep SutandarNo ratings yet
- Effect of Pregnancy On Sexual Function of Couples: AbstractDocument8 pagesEffect of Pregnancy On Sexual Function of Couples: AbstractYosep SutandarNo ratings yet
- Acog Committee Opinion: Dysmenorrhea and Endometriosis in The AdolescentDocument10 pagesAcog Committee Opinion: Dysmenorrhea and Endometriosis in The AdolescentYosep SutandarNo ratings yet
- Emergency Contraception: Sogc Clinical Practice GuidelineDocument9 pagesEmergency Contraception: Sogc Clinical Practice GuidelineYosep SutandarNo ratings yet
- Changes in The Sexual Function During Pregnancy: Aim. MethodsDocument10 pagesChanges in The Sexual Function During Pregnancy: Aim. MethodsYosep SutandarNo ratings yet
- Mao2014 Article ImagingOfPelvicLymphNodesDocument13 pagesMao2014 Article ImagingOfPelvicLymphNodesYosep SutandarNo ratings yet
- Murtagh 2010Document9 pagesMurtagh 2010Yosep SutandarNo ratings yet
- Eng - PDF JsessionidDocument34 pagesEng - PDF JsessionidYosep SutandarNo ratings yet
- Systematic Reviews To Support Evidence-Based Medicine (2nd Edition)Document216 pagesSystematic Reviews To Support Evidence-Based Medicine (2nd Edition)Yosep Sutandar100% (1)
- Enteral NutritionDocument73 pagesEnteral NutritionYosep SutandarNo ratings yet
- NSAMR Systematic ReviewDocument8 pagesNSAMR Systematic ReviewYosep SutandarNo ratings yet
- Practice Bullet In: Emergency ContraceptionDocument11 pagesPractice Bullet In: Emergency ContraceptionYosep SutandarNo ratings yet
- Pi Is 0884217517304100Document3 pagesPi Is 0884217517304100Yosep SutandarNo ratings yet
- FSFI Questionnaire2000Document5 pagesFSFI Questionnaire2000Dewi AsmalindaNo ratings yet
- Faktor Risiko Hemorrhage Pasca Post PartumDocument8 pagesFaktor Risiko Hemorrhage Pasca Post PartumDiniNo ratings yet
- Ofe & MveDocument5 pagesOfe & MvePencenk AzznewNo ratings yet
- Literature ReviewDocument2 pagesLiterature ReviewTaroobNo ratings yet
- Https://d1c0fc7ib89kee - Cloudfront.net/uploads/attachment/file//reproduction Exam QuestionDocument8 pagesHttps://d1c0fc7ib89kee - Cloudfront.net/uploads/attachment/file//reproduction Exam QuestionAmaya AliNo ratings yet
- Policy On Family PlanningDocument2 pagesPolicy On Family PlanningLILIW RHUNo ratings yet
- A Study On Menstrual Hygiene Among High School Students of Panachikkad Locality at Kottayam DistrictDocument11 pagesA Study On Menstrual Hygiene Among High School Students of Panachikkad Locality at Kottayam Districtnamitha sureshNo ratings yet
- Clinical Case Presentation:: Premature Rupture of MembranesDocument31 pagesClinical Case Presentation:: Premature Rupture of Membranesjoshua remonNo ratings yet
- Science10 Q3 SLM5 1 PDFDocument17 pagesScience10 Q3 SLM5 1 PDFBien DivinaflorNo ratings yet
- Antara Provider LeafletDocument2 pagesAntara Provider Leafletganapa247No ratings yet
- Contraception ChartDocument4 pagesContraception ChartTJNo ratings yet
- 3 - Puerperium and LactationDocument29 pages3 - Puerperium and LactationKholoud KholoudNo ratings yet
- Ovarian Cyst FinalDocument26 pagesOvarian Cyst FinalReicy Aquino SacularNo ratings yet
- Natural Family Planning Your GuideDocument9 pagesNatural Family Planning Your GuideeltonNo ratings yet
- IuiDocument34 pagesIuiDenis100% (1)
- Feminism and MotherhoodDocument1 pageFeminism and Motherhoodgeovidiella1No ratings yet
- Cervical Mucus LectureDocument5 pagesCervical Mucus LectureJay AdamzNo ratings yet
- Gynecological ExaminationDocument18 pagesGynecological ExaminationPutri NoviyantiNo ratings yet
- Hormone FertilityDocument2 pagesHormone FertilityTAHIRANo ratings yet
- Reproductive HistologyDocument24 pagesReproductive HistologyTiffany MaxwellNo ratings yet
- Screenshot 2024-01-19 at 5.10.09 PMDocument1 pageScreenshot 2024-01-19 at 5.10.09 PMdhruvrana1133No ratings yet
- Shaking OrgasmDocument71 pagesShaking OrgasmNicholasNo ratings yet
- Pregnancy Test LectureDocument2 pagesPregnancy Test Lecturejacynda linsanganNo ratings yet
- Embryology of Cervix & OvaryDocument40 pagesEmbryology of Cervix & Ovaryshrinkhala bhattaraiNo ratings yet
- A Space of Her Own: Personal Narratives of Twelve Women: Take Home Assignment: Book ReviewDocument3 pagesA Space of Her Own: Personal Narratives of Twelve Women: Take Home Assignment: Book ReviewNandini SinghNo ratings yet
- Wacs Revision Course Final Program (March 2012)Document8 pagesWacs Revision Course Final Program (March 2012)ifeanyi_osiNo ratings yet
- OB-GYN MCQs (1) - 124-129Document6 pagesOB-GYN MCQs (1) - 124-129KyunaNo ratings yet
- Primary Amenorrhea NotesDocument2 pagesPrimary Amenorrhea NotesRomulo Vincent PerezNo ratings yet
- Nilai Normal ElisaDocument3 pagesNilai Normal ElisaMiftakhul JannaNo ratings yet
- Abnormal Labour: Case-Based LearningDocument7 pagesAbnormal Labour: Case-Based LearningFatimatul Syahirah Mohd Badli ShahNo ratings yet
- Faktor Yang Mempengaruhi Kejadian Dismenorea Pada Remaja Putri Kelas X Di MAN Rantauprapat Tahun 2021 Rika Handayani1Document17 pagesFaktor Yang Mempengaruhi Kejadian Dismenorea Pada Remaja Putri Kelas X Di MAN Rantauprapat Tahun 2021 Rika Handayani1Rika HandayaniNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (403)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (20)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- 12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosFrom Everand12 Rules for Life by Jordan B. Peterson - Book Summary: An Antidote to ChaosRating: 4.5 out of 5 stars4.5/5 (207)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Algorithms to Live By: The Computer Science of Human DecisionsFrom EverandAlgorithms to Live By: The Computer Science of Human DecisionsRating: 4.5 out of 5 stars4.5/5 (722)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)